Dementia - Role of MRI - 2026 update
Frederik Barkhof and Robin Smithuis
Alzheimer Centre and Image Analysis Centre, Vrije Universiteit Medical Center, Amsterdam and the Alrijne Hospital, Leiden, The Netherlands
Publicationdate
This presentation will focus on the role of MRI in the diagnosis of dementia and related diseases.
The following topics will be addressed:
- Systematic assessment of MRI in patients with suspected dementia
- MR protocol for dementia
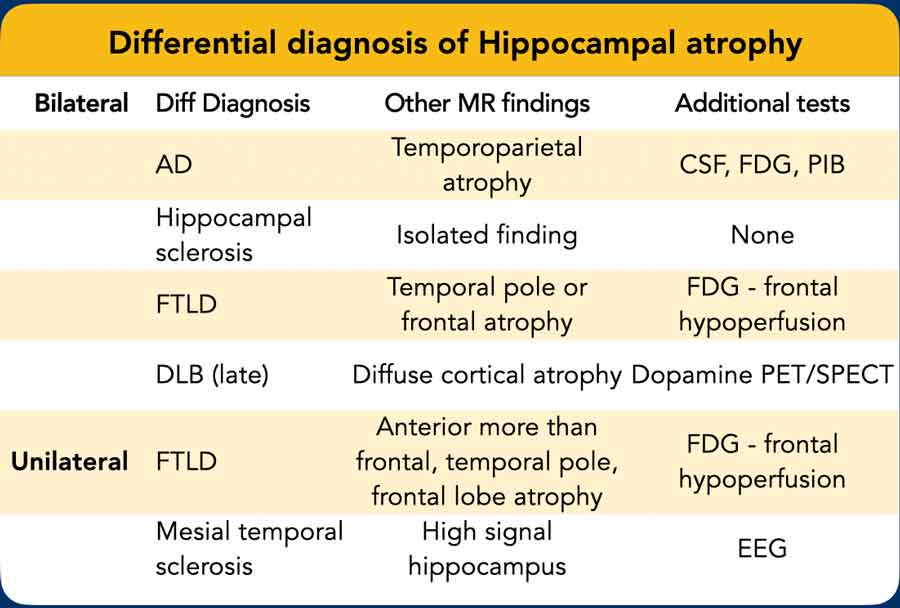
- Characteristic imaging findings in common dementia syndromes
- Alzheimer's disease (AD)
- Vascular Dementia (VaD)
- Frontotemporal lobe dementia (FTLD)
- Brief overview of other neurodegenerative disorders associated with dementia
Introduction.
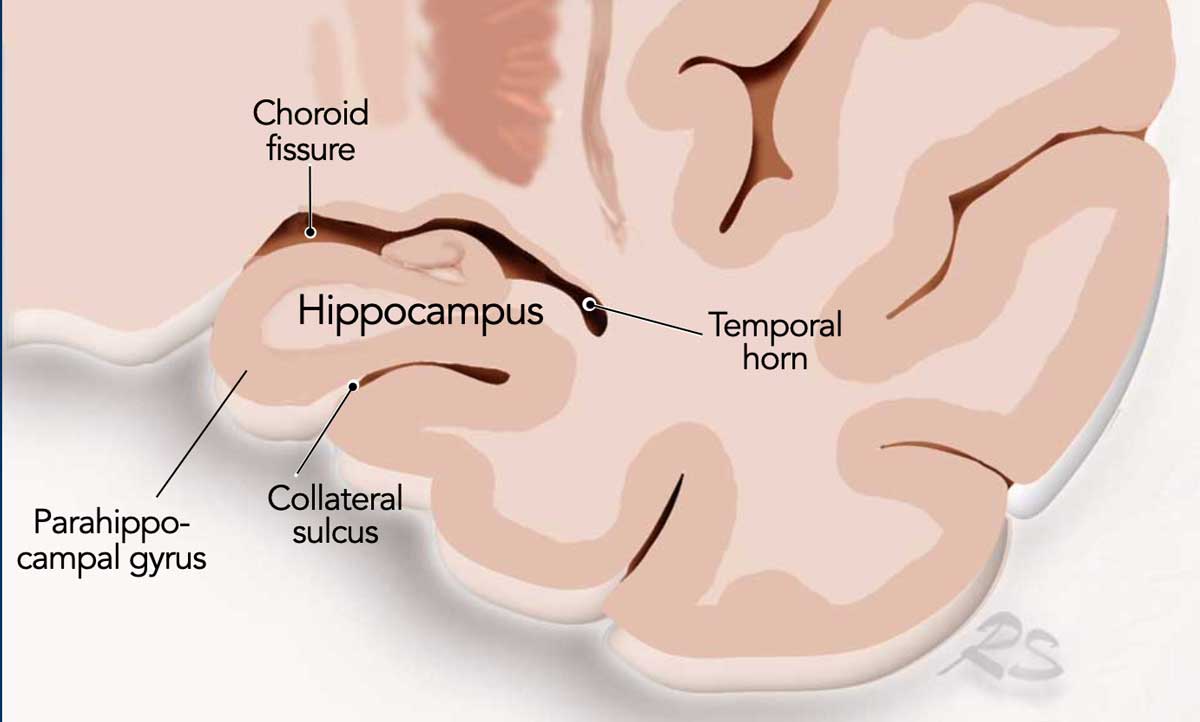 Coronal image of the hippocampus.
Coronal image of the hippocampus.
The role of neuroimaging in the assessment of dementia has evolved significantly. It is no longer limited to the exclusion of neurosurgical or structural lesions such as tumors or hydrocephalus.
MRI findings can now support, and in some cases are essential for, the diagnosis of specific neurodegenerative diseases.
Early diagnosis is one of the current challenges in the field of neuroimaging, particularly for diseases such as Alzheimer’s disease (AD). This includes the identification of prodromal stages, such as Mild Cognitive Impairment (MCI).
Early detection is important, as it may allow timely intervention with current or future therapeutic strategies.
Neuroimaging also plays a vital role in monitoring disease progression and is increasingly utilized in clinical trials focusing on Mild Cognitive Impairment and Alzheimer’s disease.
The coronal image shows the hippocampus, the main structure involved in Alzheimer’s disease.
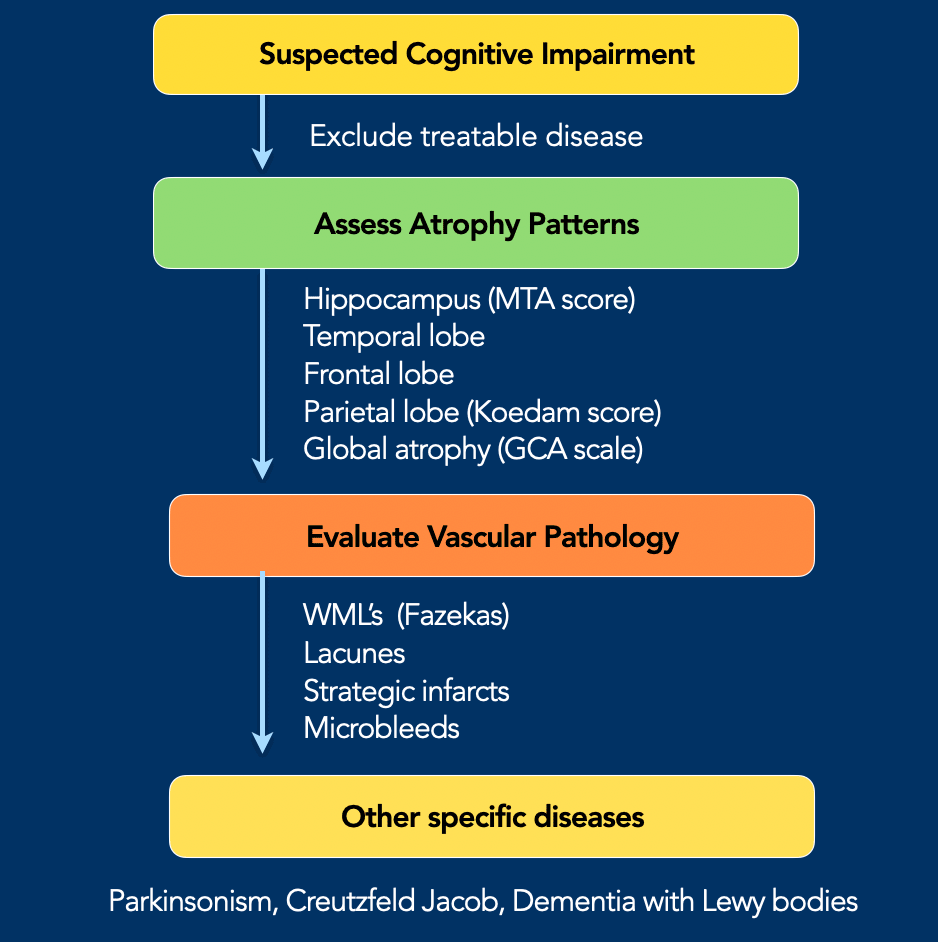
Systematic MRI Evaluation in Suspected Cognitive Impairment
- Exclude Treatable Conditions
Rule out reversible or treatable causes, such as:- Subdural hematomas
- Intracranial tumors
- Normal pressure hydrocephalus
- Assess Atrophy Patterns
Identify atrophy patterns suggestive of specific dementia subtypes.
Use quantitative scoring tables to measure the degree of atrophy (see accompanying table). - Evaluate Vascular Pathology
- Pure vascular dementia is rare, but vascular comorbidity is common and can exacerbate clinical symptoms.
- The vascular component may serve as a separate therapeutic target.
- Look for specific Dementias
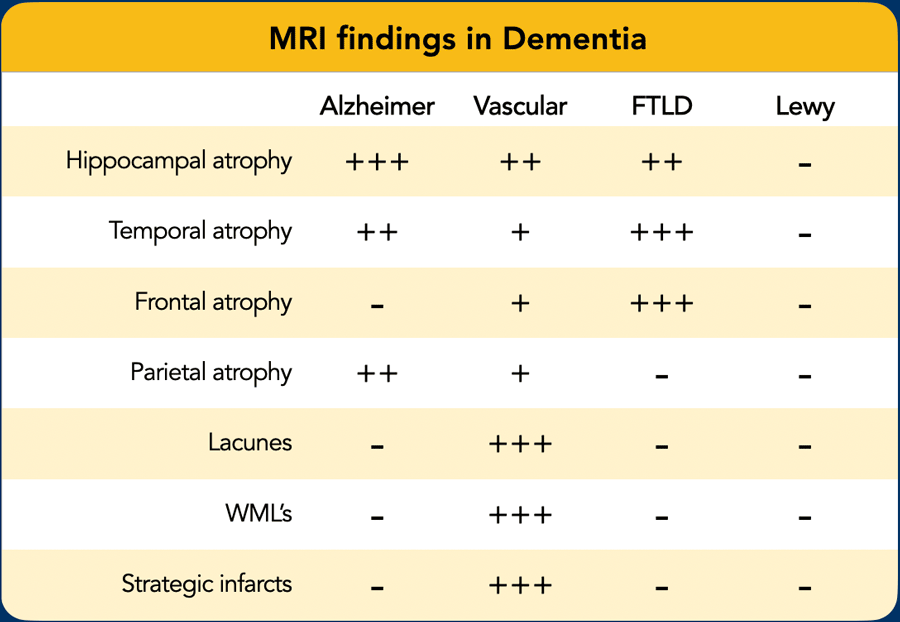
Assess for imaging features suggestive of specific dementia subtypes:
- Alzheimer’s Disease (AD):
- Medial temporal lobe atrophy (MTA)
- Parietal lobe atrophy (especially posterior)
- Frontotemporal Lobar Degeneration (FTLD):
- Asymmetric frontal lobe atrophy
- Temporal pole atrophy
- Vascular Dementia (VaD):
- Generalized cerebral atrophy
- Confluent white matter hyperintensities
- Lacunar infarcts
- Strategic infarcts (i.e., infarcts in areas involved in cognition)
- Dementia with Lewy Bodies (DLB):
- Typically, no specific MRI abnormalities
Atrophy Assessment
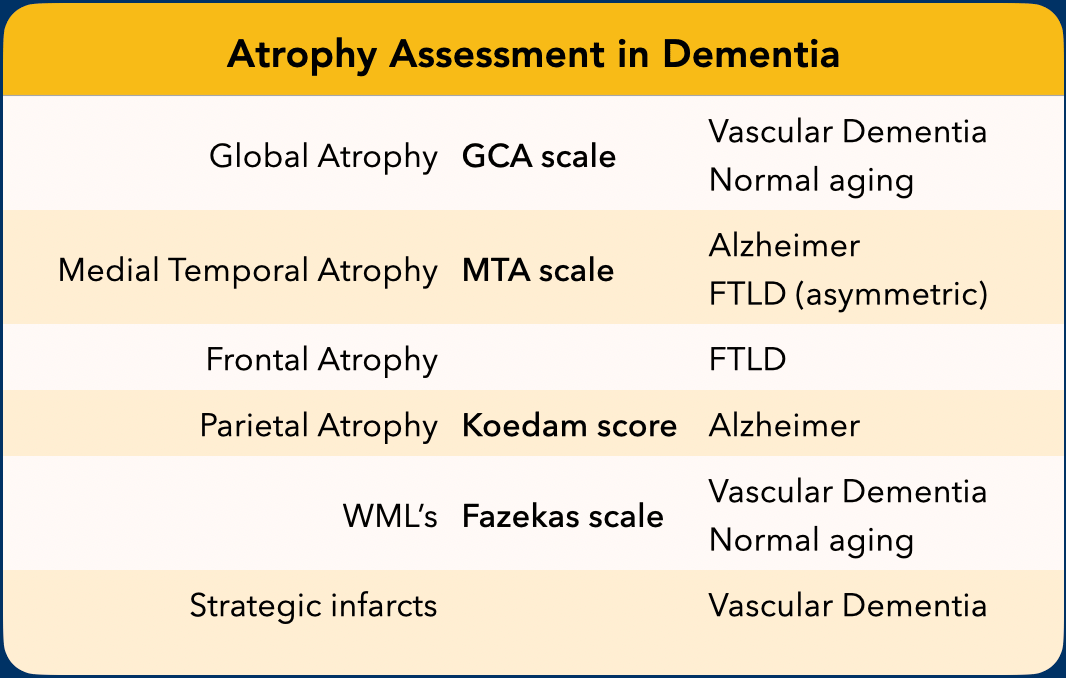
When we study the MR images we must systematically score for global atrophy, focal atrophy and for vascular disease (i.e. infarcts, white matter lesions, lacunes).
This standardized assessment of the MR findings in a patient suspected of having a cognitive disorder includes:
- GCA-scale for Global Cortical Atrophy
- MTA-scale for Medial Temporal lobe Atrophy
- Koedam score for parietal atrophy
- Fazekas scale for WM lesions
- Looking for strategic infarcts
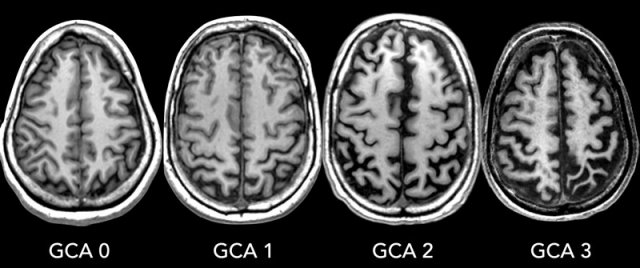
GCA-scale - Global Cortical Atrophy
GCA scale is the mean score for cortical atrophy throughout the complete cerebrum:
- 0: no cortical atrophy
- 1: mild atrophy: opening of sulci
- 2: moderate atrophy: volume loss of gyri
- 3: severe end-stage atrophy: 'knife blade'.
Cortical atrophy is most accurately assessed on FLAIR (Fluid-Attenuated Inversion Recovery) sequences.
In certain neurodegenerative conditions, atrophy may be asymmetric and localized to specific brain regions.
Radiological reports should explicitly document any regional atrophy or asymmetry.
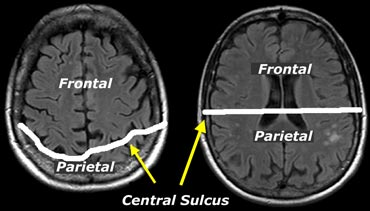
Images
Note that, cranially, the central sulcus is typically positioned more posteriorly than might be anticipated (see figure).
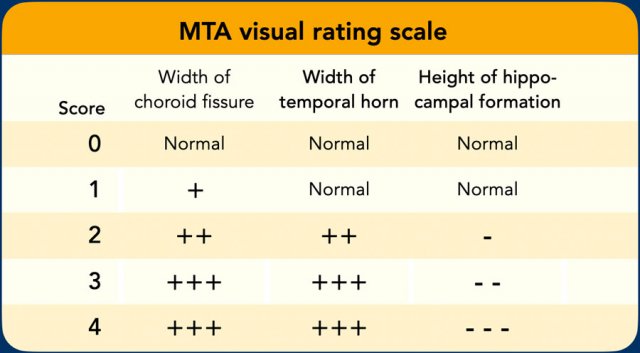
MTA score - Medial Temporal Atrophy
The MTA-score should be rated on coronal T1-weighted images at a consistent slice position.
Select a slice through the corpus of the hippocampus, at the level of the anterior pons.
Data from a study with 222 controls and patients with various forms of dementia in which this visual rating scale was used to assess temporal lobe atrophy suggest that sensitivities and specificities of 85% can be obtained for patients with AD.
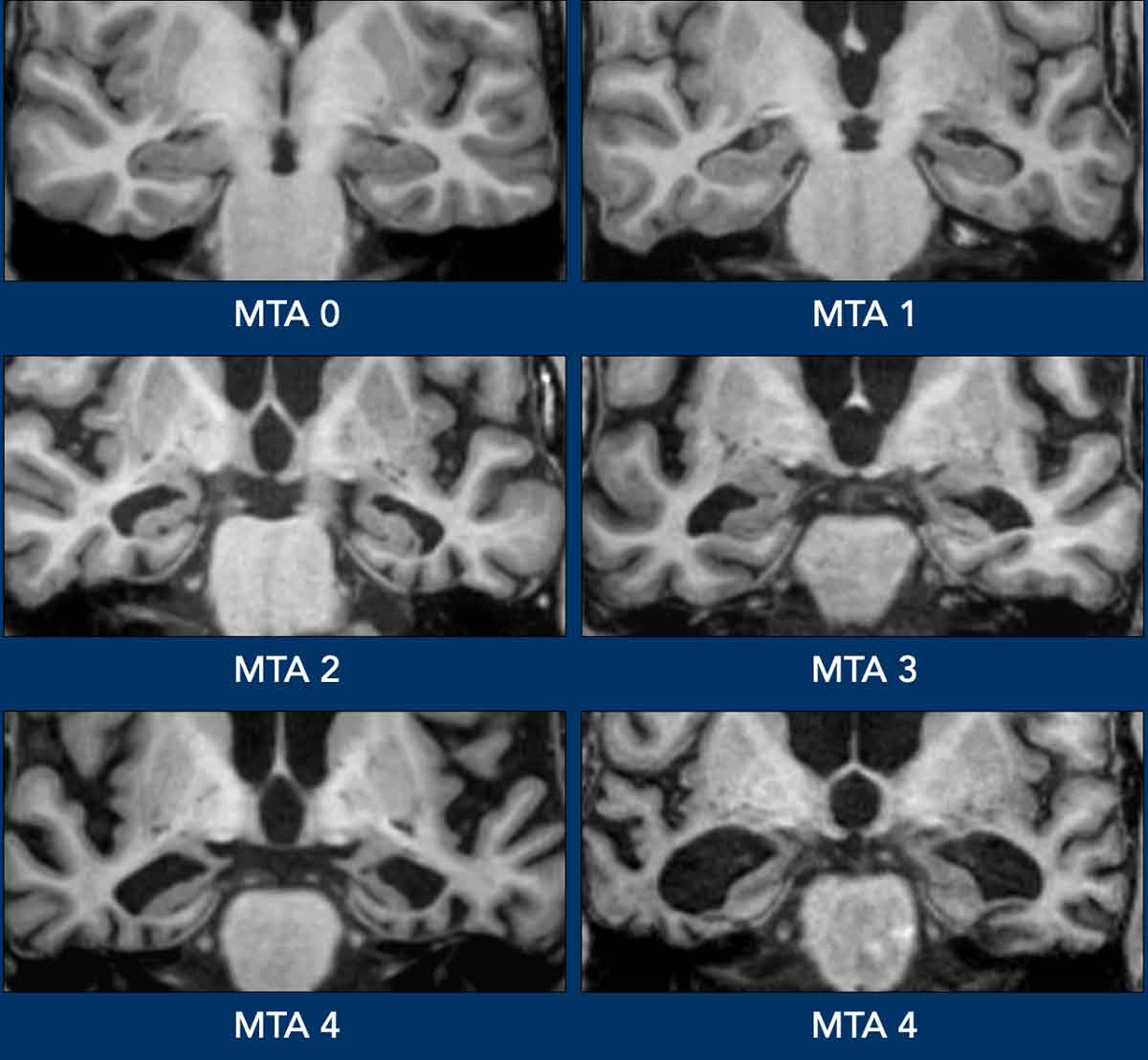
The MTA score is determined by a visual assessment of three parameters: the width of the choroid fissure, the width of the temporal horn, and the height of the hippocampal formation.
Scoring criteria:
- MTA 0: No atrophy
- MTA 1: Widening of the choroid fissure only
- MTA 2: Widening of the choroid fissure and the temporal horn of the lateral ventricle
- MTA 3: Moderate loss of hippocampal volume (reduced height)
- MTA 4: Severe volume loss of the hippocampus
Interpretation:
- < 75 years: A score ≥ 1.5 is considered abnormal.
- ≥ 75 years: A score ≥ 2.5 is considered abnormal.
A high Medial Temporal Atrophy (MTA) score is highly sensitive for Alzheimer’s disease (AD), present in most AD patients but rarely in controls, making it effective for distinguishing AD from healthy individuals. However, MTA is not specific to AD, as it can also occur in other dementias.
In MCI (a potential prodromal AD state), a negative MTA score strongly suggests a low likelihood of progression to AD (high negative predictive value), except in very young patients, where AD may present with a more posterior atrophy pattern.
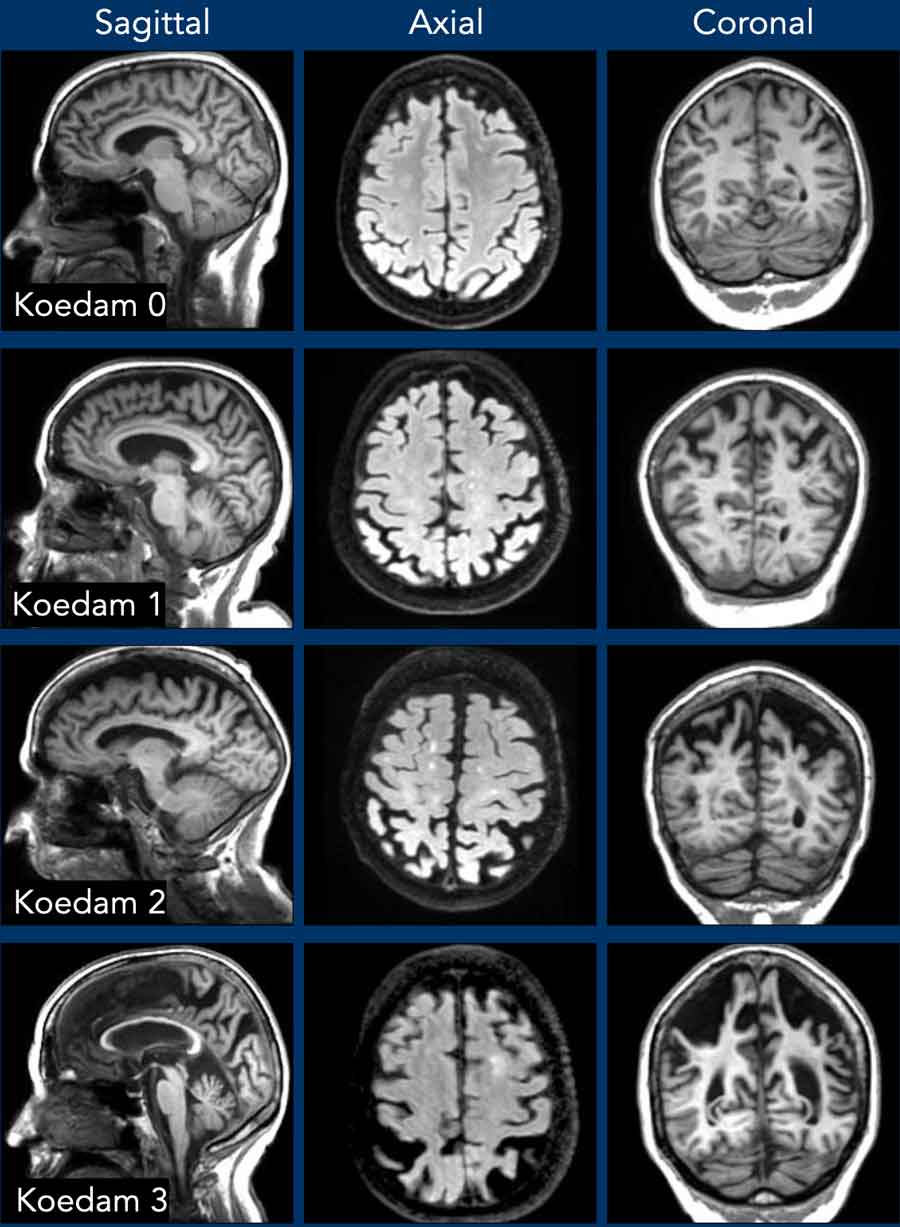
Koedam score - Parietal Atrophy
In addition to medial temporal lobe atrophy, parietal atrophy also has a positive predictive value in the diagnosis of AD.
Atrophy of the precuneus is particularly characteristic of AD.
This is particularly the case in young patients with AD (presenile AD), who may have normal MTA-scores.
The Koedam scale rates parietal atrophy - assessed in sagittal, coronal and axial planes.
In these planes, widening of the posterior cingulate and parieto-occipital sulci as well as parietal atrophy - including the precuneus - is rated (Table).
When different scores are obtained in different orientations, the highest score must be considered (16).
Koedam 0
- No cortical atrophy
- Closed sulci of the parietal lobes and cuneus
Koedam 1
- Mild parietal cortical atrophy
- Mild widening of posterior cingulate and parieto-occipital sulci
Koedam 2
- Substantial parietal atrophy
- Substantial widening of sulci
Koedam 3
- End-stage „knife-blade” atrophy
- Extreme widening of posterior cingulate and parieto-occipital sulci
Vascular Disease Assessment
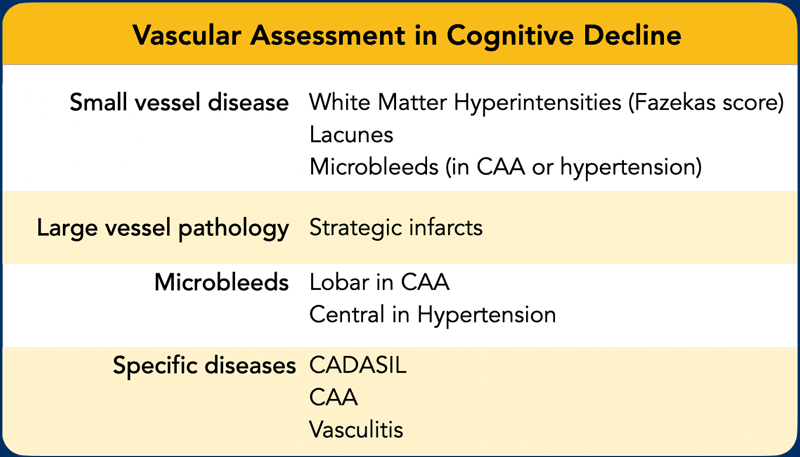
The combination of vascular disease and Alzheimer’s disease best predicts the development of dementia, as demonstrated by many studies.
This is consistent with the “double hit” concept, where vascular and neurodegenerative pathologies synergize.
White matter lesions may act as a steppingstone for the clinical manifestation of AD and subclinical vascular damage lowers the threshold for cognitive decline.
Amyloid deposits are observed in both cerebral amyloid angiopathy (CAA) and in Alzheimer’s disease.
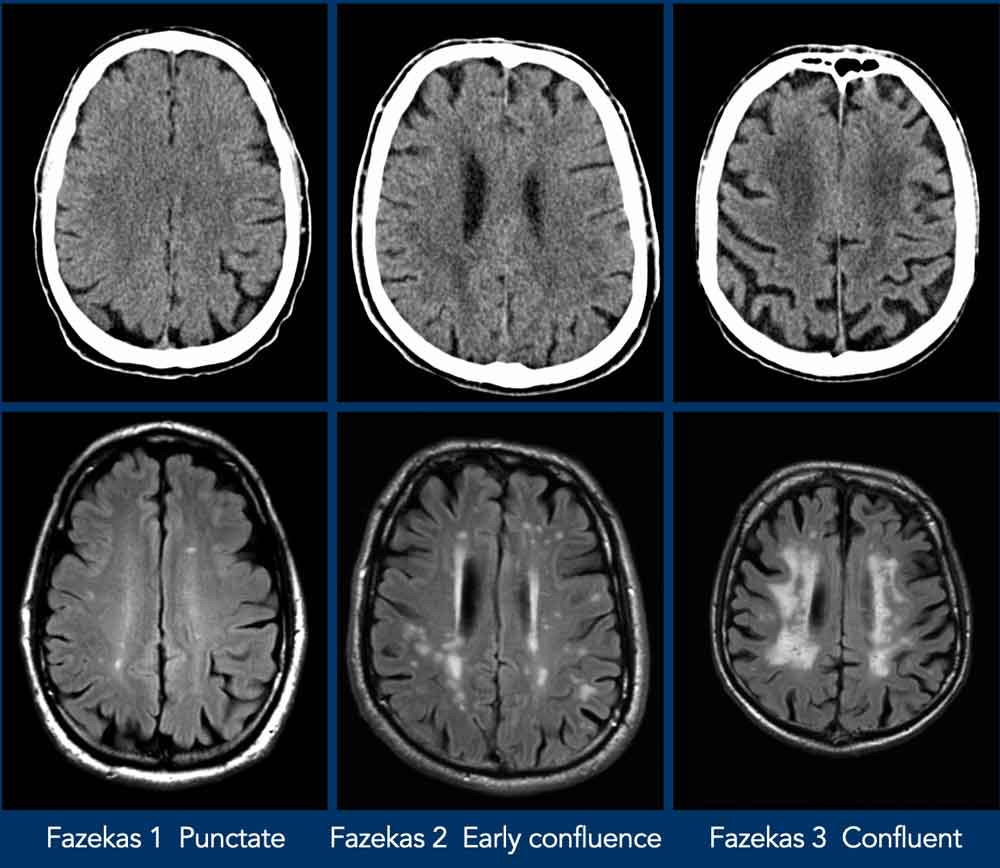
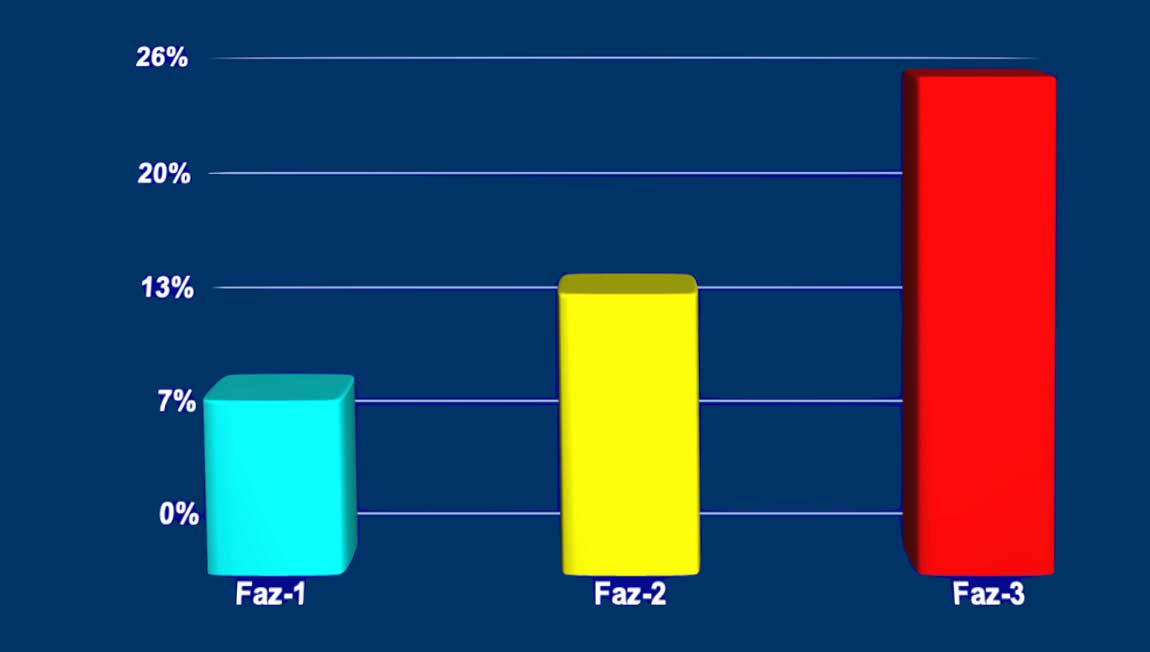
Fazekas scale for WM lesions
On MR, white matter hyperintensities (WMH) and lacunes - both of which are frequently observed in the elderly - are generally viewed as evidence of small vessel disease.
The Fazekas-scale provides an overall impression of the presence of WMH in the entire brain.
It is best scored on transverse FLAIR or T2-weighted images.
Score:
- Fazekas 0: None or a single punctate WMH lesion
- Fazekas 1: Multiple punctate lesions
- Fazekas 2: Beginning confluency of lesions (bridging)
- Fazekas 3: Large confluent lesions
The Fazekas scale for WM lesions predicts future disability in elderly
Fazekas 1 is considered normal in the elderly.
Fazekas 2 and 3 are pathologic and at high risk for disability, but may be seen in normally functioning individuals.
Table
In 600 normally functioning elderly people the Fazekas score predicted disability within one year.
In the Fazekas 3 group 25% was disabled within one year..
Three year follow-up shows that severe white matter changes independently and strongly predict rapid global functional decline.
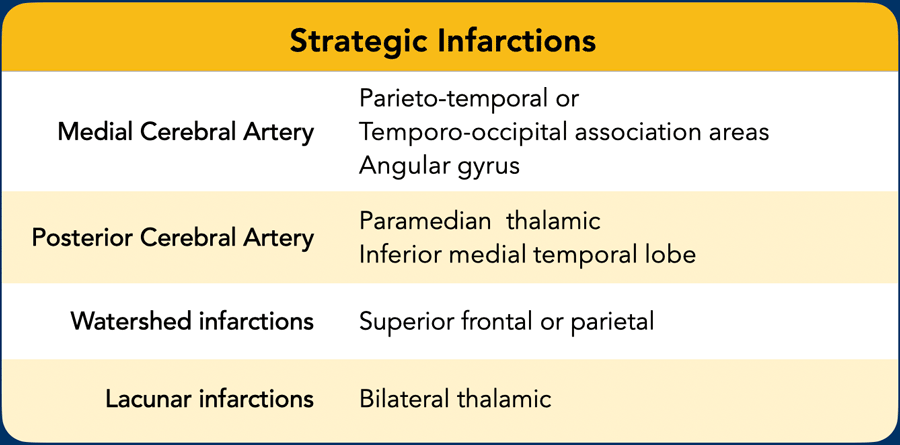
Strategic infarctions
Strategic infarctions are infarctions in areas that are crucial for normal cognitive functioning of the brain.
The areas are summarized in the table.
Cognitive dysfunction in VaD can be the result of:
- Large vessel infarctions:
- Bilateral in the anterior cerebral artery territory.
- Parietotemporal- and temporo-occipital association areas of the dominant hemisphere (angular gyrus included)
- Posterior cerebral artery territory infarction of the paramedian thalamic region and inferior medial temporal lobe of the dominant hemisphere
- Watershed infarctions in the dominant hemisphere (superior frontal and parietal)
- Small vessel disease:
- Multiple lacunar infactions in frontal white matter (>2) and basal ganglia (>2)
- WMLs (at least more than 25% of WM)
- Bilateral thalamic lesions
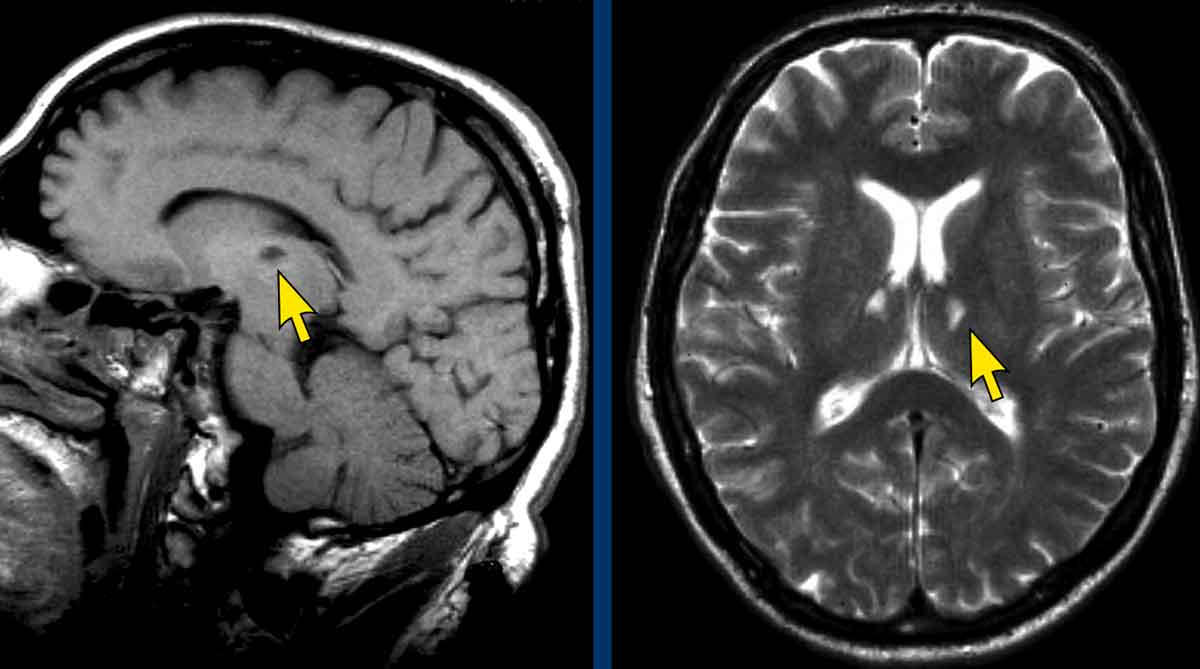
Strategic infarctions
Strategic infarctions are best seen on transverse FAIR and T2W sequences.
Images
Bilateral thalamic infarctions.
These lesions are often associated with cognitive dysfunction.
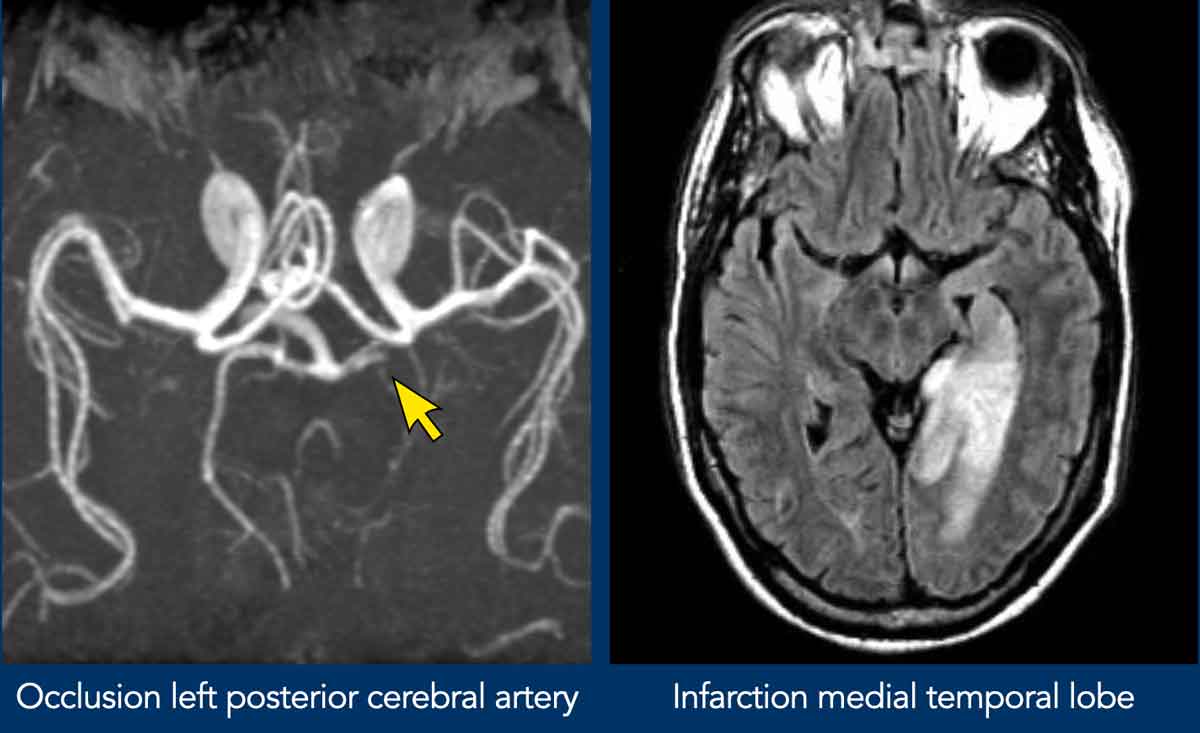
Strategic infarctions
Images
Large vessel infaction in the dominant hemisfere.
Microbleeds
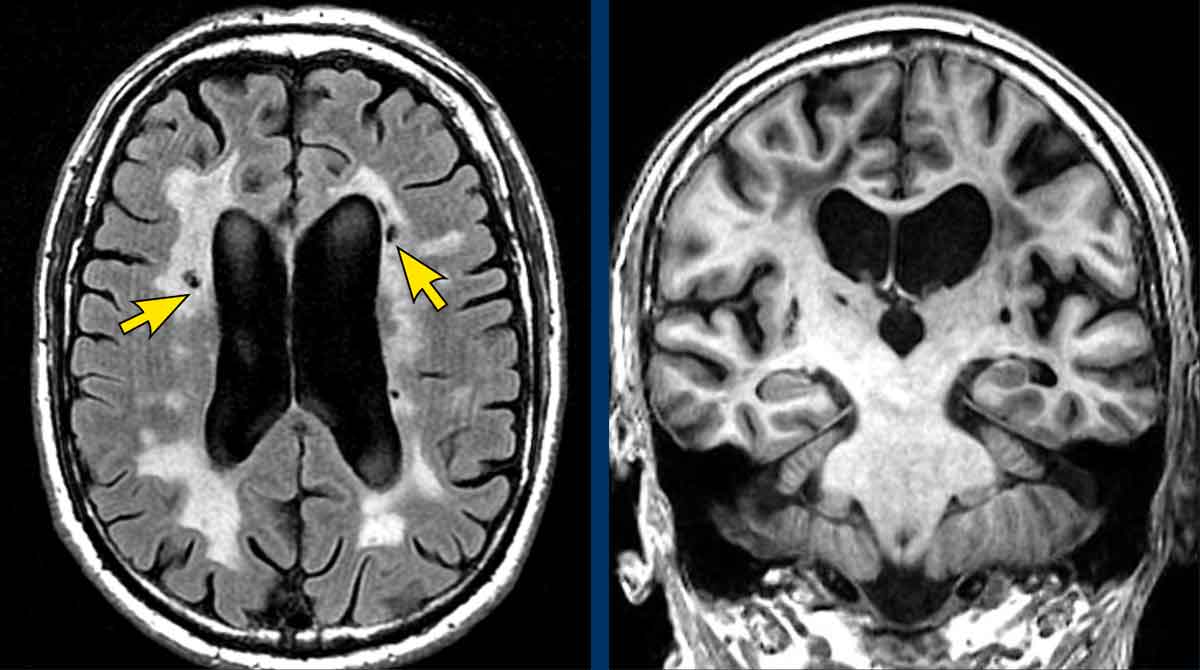
Vascular dementia
Pure vascular dementia is uncommon, but is occasionally seen.
Images
- Confluent white matter hyperintensities (Fazekas 3)
- Lacunes (arrows)
- No medial temporal lobe atrophy (MTA 1)
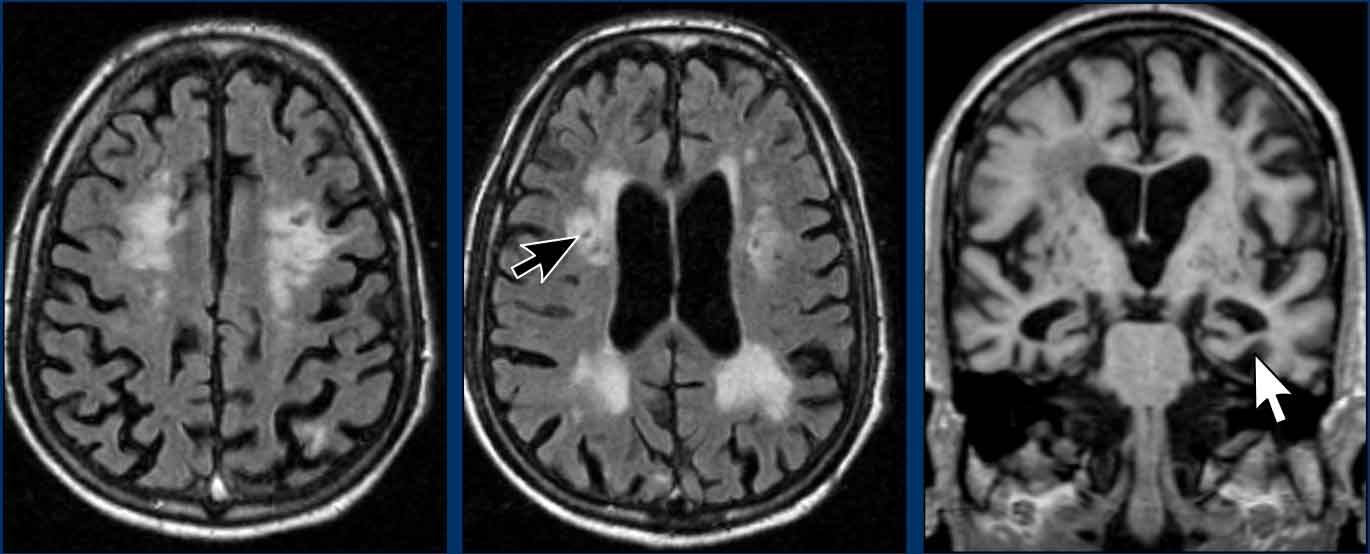
The combination of Alzheimer's disease and vascular disease is the most common presentation.
Images
- Confluent white matter intensities (Fazekeas 3)
- Lacunes (black arrow)
- Atrophy of the medial temporal lobe (white arrow))
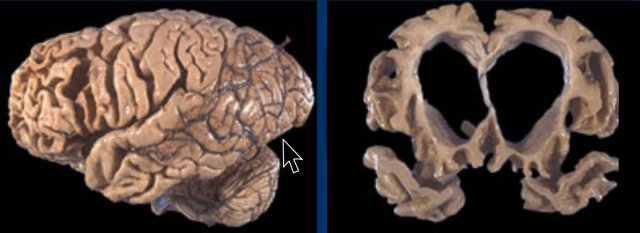
Normal Ageing
Brain findings in normal aging
1. Atrophy
- General: Mild to moderate white matter atrophy is common.
- Sulcal widening: Non-specific fronto-parietal sulcal widening (reflecting volume loss).
- Medial temporal lobe (MTL): Mild atrophy may occur; MTA score ≤2 in individuals >75 years can still be normal.
2. Perivascular Spaces
- Virchow-Robin spaces: Increased prominence, especially in the basal ganglia and white matter.
3. White Matter Hyperintensities (WMH)
- Fazekas grade 1: Limited, punctate WMH (e.g., in the deep white matter or periventricular regions) are acceptable in normal aging.
4. Iron Deposition
- Physiological: Progressive iron accumulation in:
- Basal ganglia (globus pallidus, putamen)
- Red nucleus
- Substantia nigra pars reticulata
- MRI appearance: Hypointensity on T2-weighted or SWI sequences*.
5. "Caps and Bands"
- Periventricular high signal: Thin T2/FLAIR hyperintense rims ("caps" around the frontal horns, "bands" along the lateral ventricles) may develop with age (arrow).
Pathological Findings (Not Typical of Normal Aging)
- Lacunes: Always pathological (indicative of small-vessel disease).
- Fazekas grade ≥2: Confluent or diffuse WMH (suggestive of small-vessel ischemia or vascular dementia).
- MTA score >2 in <75 years: Suggestive of early neurodegenerative disease (e.g., Alzheimer’s).
- Asymmetrical or focal atrophy: May indicate degenerative or vascular pathology.
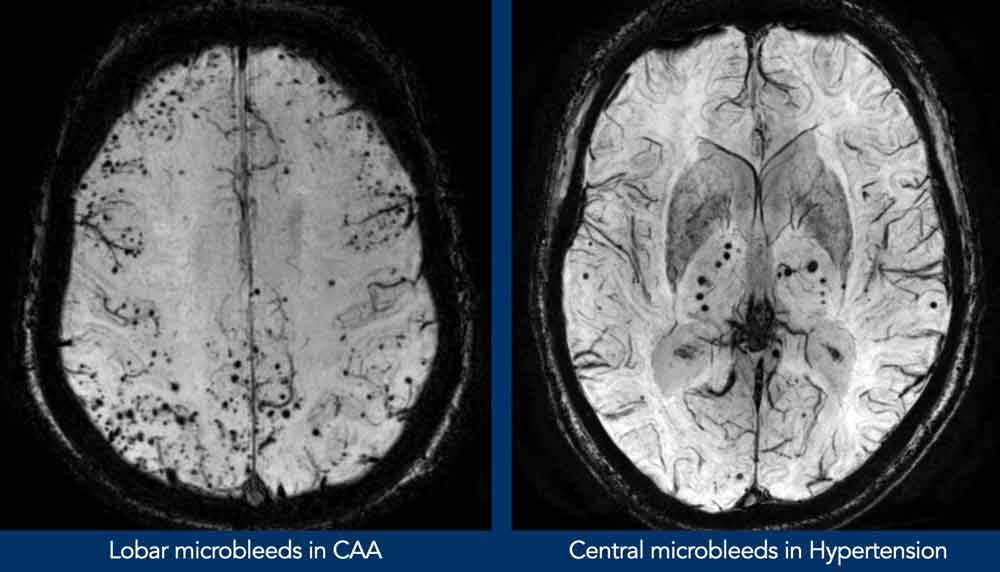
Cerebral Amyloid Angiopathy (CAA)
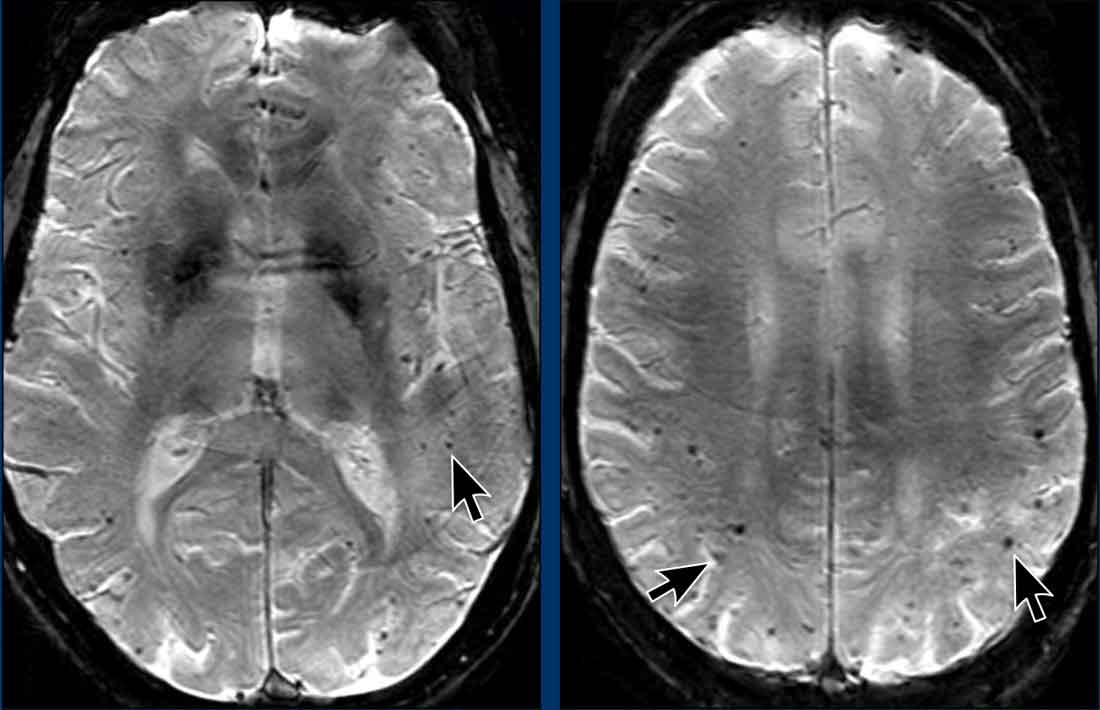
Dementia may be the clinical presentation in CAA, a condition in which β-amyloid is deposited in cortical and leptomeningeal vessel walls, leading to vascular fragility.
This results in hemorrhage, usually microbleeds, but less common subarachnoid hemorrhage or lobar hematomas.
There is an Increased risk of recurrent intracranial hematomas, especially with anticoagulation.
MRI Findings
- T2/SWI: Microbleeds presenting as multiple blooming artifacts (hypointense foci) in peripheral locations.
- FLAIR: Moderate-severe white matter hyperintensities (Fazekas 2–3), often posterior-dominant.
- Macrohemorrhages: Lobar hematomas (often recurrent), subarachnoid hemorrhage (convexity SAH).
Differential Diagnosis
- Hypertensive microbleeds: Typically deep (basal ganglia, thalamus, brainstem).
- Other microangiopathies: CADASIL, diabetic angiopathy (less peripheral).
Frontotemporal Lobar Degeneration (FTLD )
FTLD, previously known as Pick’s disease, is a progressive neurodegenerative dementia that accounts for 5–10% of all dementia cases. It occurs relatively more frequently in presenile individuals.
FTLD is clinically characterized by prominent behavioral and language disturbances, which may precede or overshadow memory deficits. Currently, there is no effective treatment for this condition.
Neuroimaging plays a crucial role in diagnosis, as the radiological findings are often distinctive.
Typical imaging features include pronounced atrophy of the frontal and/or temporal lobes.
In certain FTLD subtypes, such as semantic dementia, the atrophy may be strikingly asymmetric, with progressive aphasia and predominant degeneration of the left temporal lobe.
 FTLD: T2WI and FLAIR with 'knife blade' atrophy of left temporal lobe with normal right temporal lobe
FTLD: T2WI and FLAIR with 'knife blade' atrophy of left temporal lobe with normal right temporal lobe
FTLD example
These images are of a patient with progressive aphasia.
The most prominent finding is striking asymmetric atrophy of the left temporal lobe, involving not only the hippocampus but also the temporal poles.
The atrophy is so severe that the gyri appear sharply thinned, a feature often described as "knife-blade atrophy."
Additionally, there is increased signal intensity on the FLAIR sequence, likely due to underlying gliosis.
These imaging findings are pathognomonic for frontotemporal lobar degeneration (FTLD).
Clinically, patients with left-sided temporal atrophy typically present with obvious language deficits.
In contrast, right-sided temporal atrophy may be less readily recognized, as these patients often exhibit only subtle impairments, such as difficulty with facial recognition (prosopagnosia).
Dementia with Parkinsonism

This refers to a group of neurodegenerative disorders characterized by both cognitive impairment (dementia) and motor symptoms typical of parkinsonism (e.g., bradykinesia, rigidity, tremor, and postural instability).
Key Types of Dementia with Parkinsonism
- Dementia with Lewy Bodies (DLB)
- Core features: Fluctuating cognition, visual hallucinations, parkinsonism, and REM sleep behavior disorder.
- Pathology: Lewy bodies (alpha-synuclein aggregates) in cortical and subcortical regions.
- Imaging: Typically normal hippocampus on MRI; DaTSCAN shows reduced dopaminergic activity.
- Parkinson’s Disease Dementia (PDD)
- Definition: Dementia developing in patients with established Parkinson’s disease (PD) (diagnosed after motor symptoms).
- Symptoms: Similar to DLB but with a clearer history of parkinsonism preceding cognitive decline.
- Pathology: Lewy bodies + variable Alzheimer’s-type pathology (amyloid plaques, neurofibrillary tangles).
- Progressive Supranuclear Palsy (PSP)
- Motor symptoms: Early postural instability, vertical gaze palsy, axial rigidity, and falls.
- Cognitive symptoms: Frontal lobe dysfunction (apathy, executive dysfunction, behavioral changes).
- Pathology: Tau protein aggregates in subcortical structures (e.g., basal ganglia, brainstem).
- Multiple System Atrophy (MSA)
- Motor symptoms: Parkinsonism (MSA-P) or cerebellar ataxia (MSA-C).
- Autonomic symptoms: Severe dysautonomia (e.g., orthostatic hypotension, urinary incontinence).
- Cognitive symptoms: Mild to moderate executive dysfunction.
- Pathology: Alpha-synuclein aggregates in oligodendrocytes (glial cytoplasmic inclusions).
- Corticobasal Degeneration (CBD)
- Motor symptoms: Asymmetric rigidity, apraxia, dystonia, and alien limb phenomenon.
- Cognitive symptoms: Cortical dysfunction (e.g., aphasia, visuospatial deficits).
- Pathology: Tau pathology in cortical and basal ganglia regions.
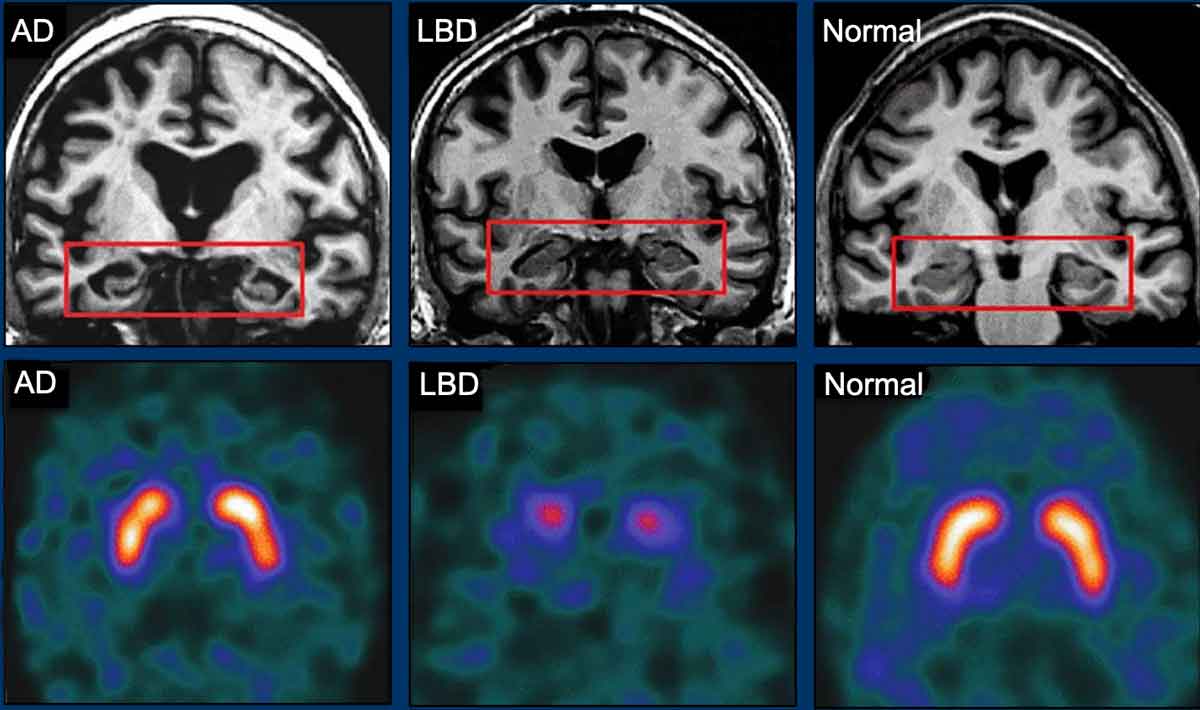
Dementia with Lewy bodies
Dementia with Lewy bodies (DLB) accounts for approximately 25% of all dementia cases and is classified among the atypical parkinsonian syndromes, alongside progressive supranuclear palsy (PSP) and multiple system atrophy (MSA).
Clinically, DLB may mimic Alzheimer’s disease or Parkinson’s disease dementia.
Patients typically present with one or more of the following core features: detailed visual hallucinations, parkinsonian symptoms, and fluctuations in cognition, alertness, or attention.
Role of Imaging
The role of structural neuroimaging in DLB is limited.
Brain MRI is typically normal, including the hippocampus—a key distinguishing feature from Alzheimer’s disease, the main differential diagnosis.
Functional nuclear imaging, such as DaTscan, can demonstrate abnormal dopaminergic neuronal loss, supporting the diagnosis (image).
Pathologically, DLB is defined by the presence of Lewy bodies in the hippocampal complex, subcortical nuclei, and neocortex, often accompanied by a variable number of diffuse amyloid plaques.
Cholinesterase inhibitors remain the primary pharmacological treatment for DLB.
Progressive supranuclear palsy (PSP)
PSP is also one of the atypical parkinsonian syndromes.
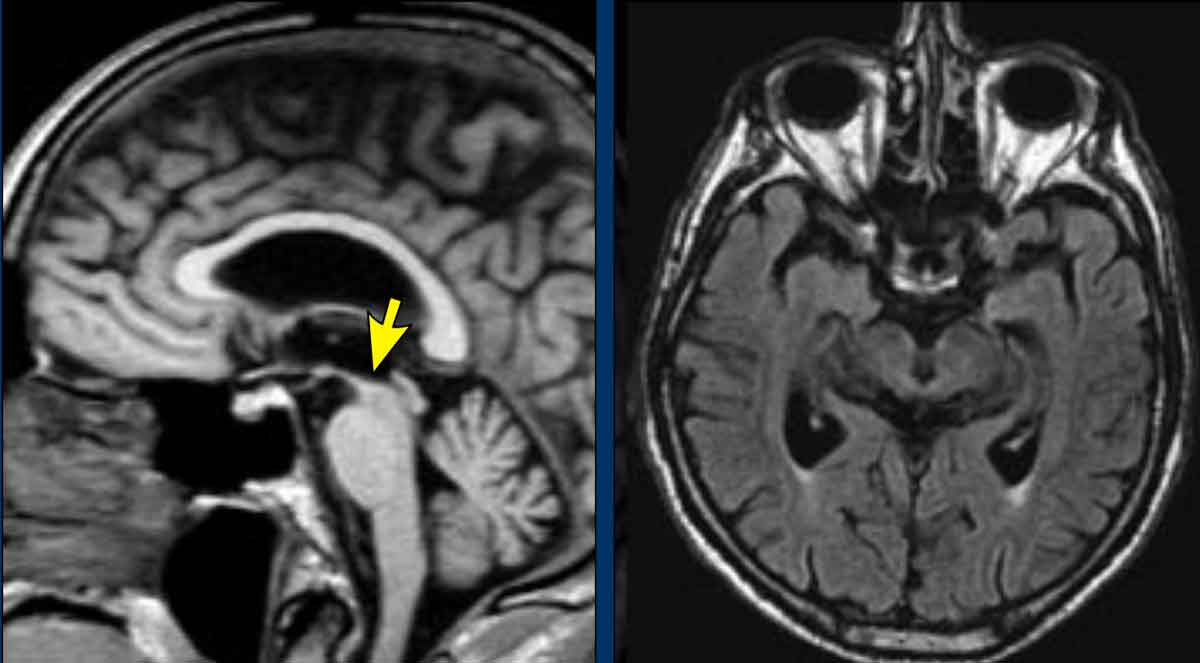
In PSP there is pronounced atrophy of the midbrain (mesencephalon), which accounts for the typical upward gaze paralysis.
Example
PSP with midbrain atrophy
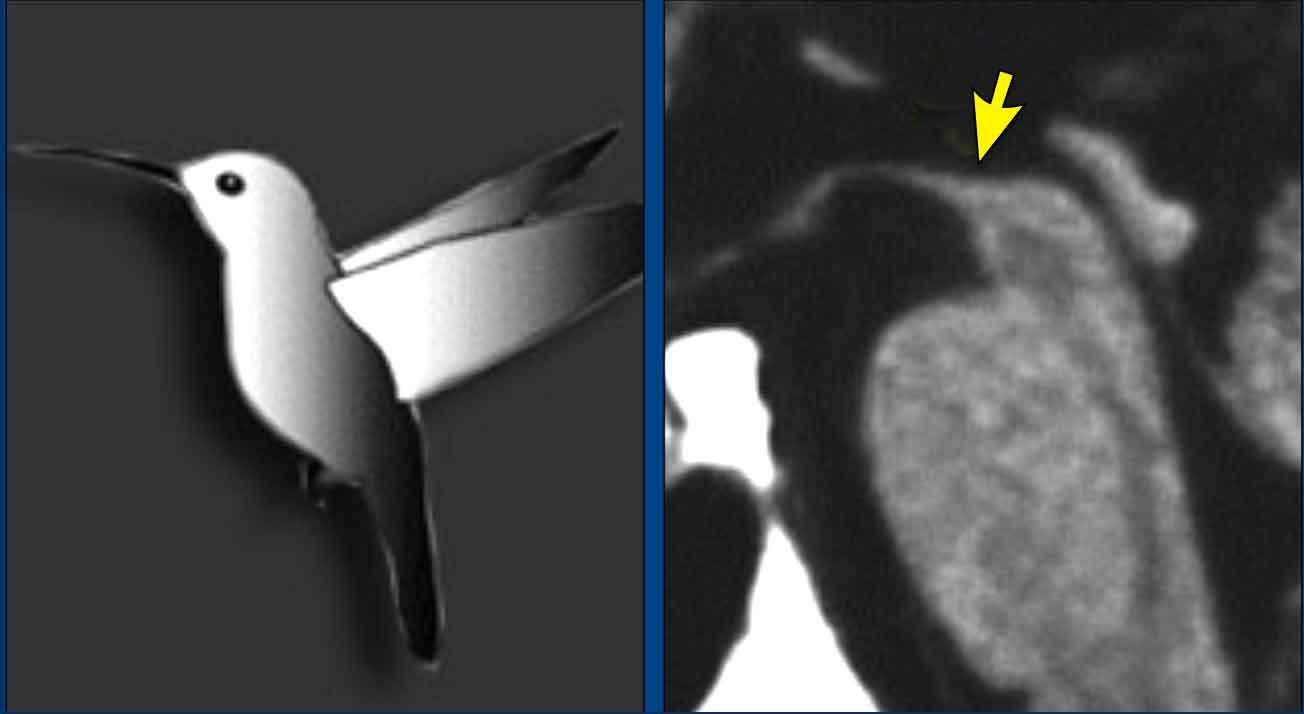
Normally the upper border of the midbrain is convex.
The atrophy of the midbrain in PSP results in a concave upper border of the midbrain with the typical 'humming bird sign' (figure).
Multi System Atrophy (MSA)
MSA is a rare, progressive neurodegenerative disorder characterized by a variable combination of parkinsonism, cerebellar ataxia, pyramidal signs, and autonomic dysfunction.
MSA is subclassified into MSA-C, MSA-P, and MSA-A based on the predominant clinical features:
- MSA-C (cerebellar variant, formerly sporadic olivopontocerebellar atrophy or sOPCA): Cerebellar symptoms (e.g., ataxia, dysarthria) predominate.
- MSA-P (parkinsonian variant, formerly striatonigral degeneration): Parkinsonian features (e.g., bradykinesia, rigidity) dominate.
- MSA-A (autonomic variant, formerly Shy-Drager syndrome): Autonomic dysfunction (e.g., orthostatic hypotension, urinary incontinence) is the primary manifestation.
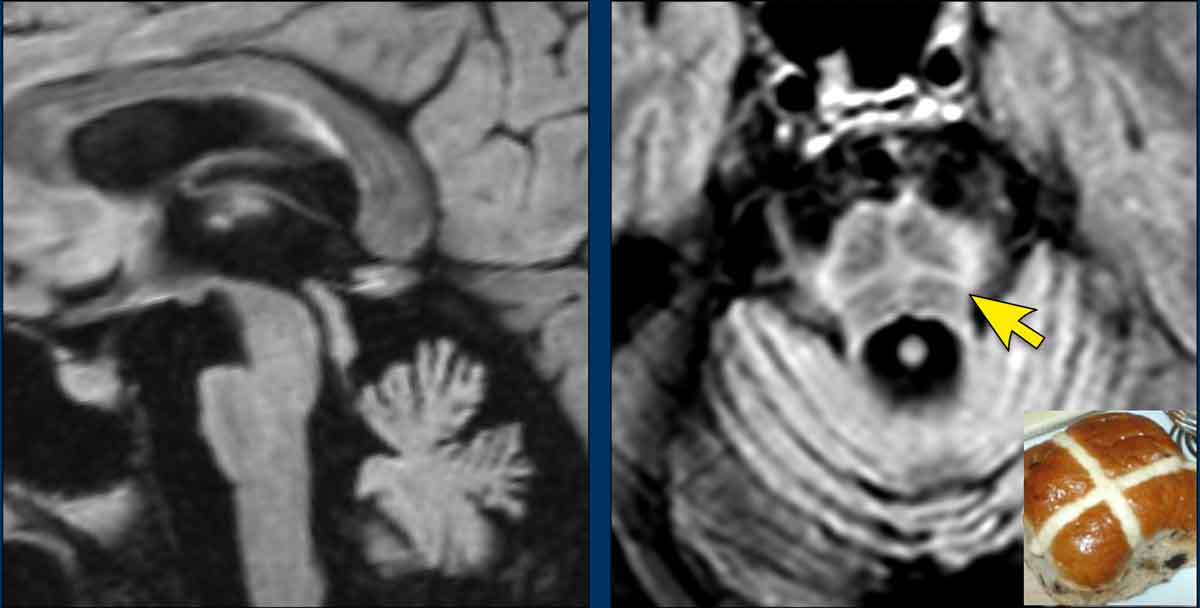
In MSA, there is pronounced cerebellar atrophy and severe pontine atrophy.
- In MSA-P, MRI typically reveals hypointensity in the dorsolateral putamen on T2-weighted images, with a characteristic "slit-like hyperintensity" lateral to the putamen.
- Unlike Progressive Supranuclear Palsy (PSP), the "hummingbird sign" is absent in MSA, as the midbrain retains a normal convex upper border.
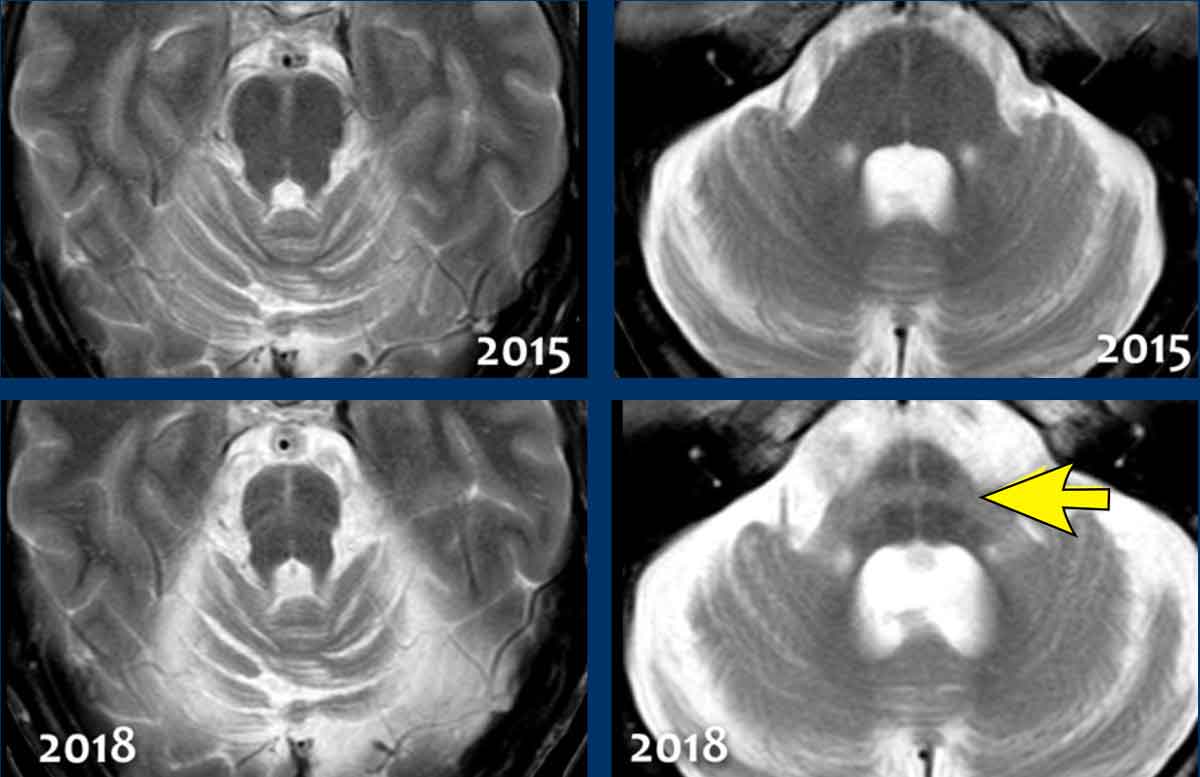
The "hot cross bun sign", resulting from pontine hyperintensity on T2-weighted images, is highly suggestive of MSA-C.
Images
Notably, in this patient, comparison of imaging from 2015 to 2018 demonstrates progressive, extreme atrophy of the pons and cerebellum.
Creutzfeldt-Jakob disease
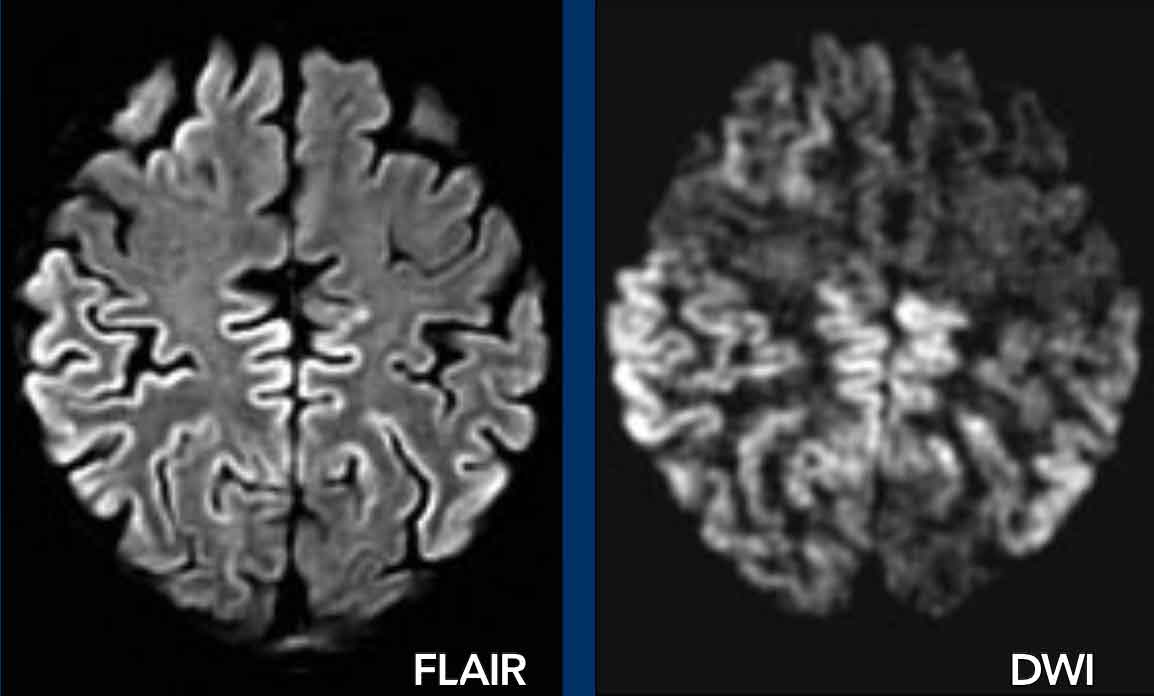
Creutzfeldt-Jakob disease is a rare, rapidly progressive, and invariably fatal neurodegenerative disorder caused by an abnormal infectious protein known as a prion.
The initial clinical manifestation is typically rapidly progressive dementia, characterized by memory impairment, personality alterations, and hallucinations.
Pathologically, Creutzfeldt-Jakob disease
is defined by spongiform changes in the cortical and subcortical gray matter, accompanied by neuronal loss and gliosis.
Neuroimaging may reveal these abnormalities, which are sometimes detectable on FLAIR sequences but are most conspicuous on DWI, involving the striatum, neocortex, or both.
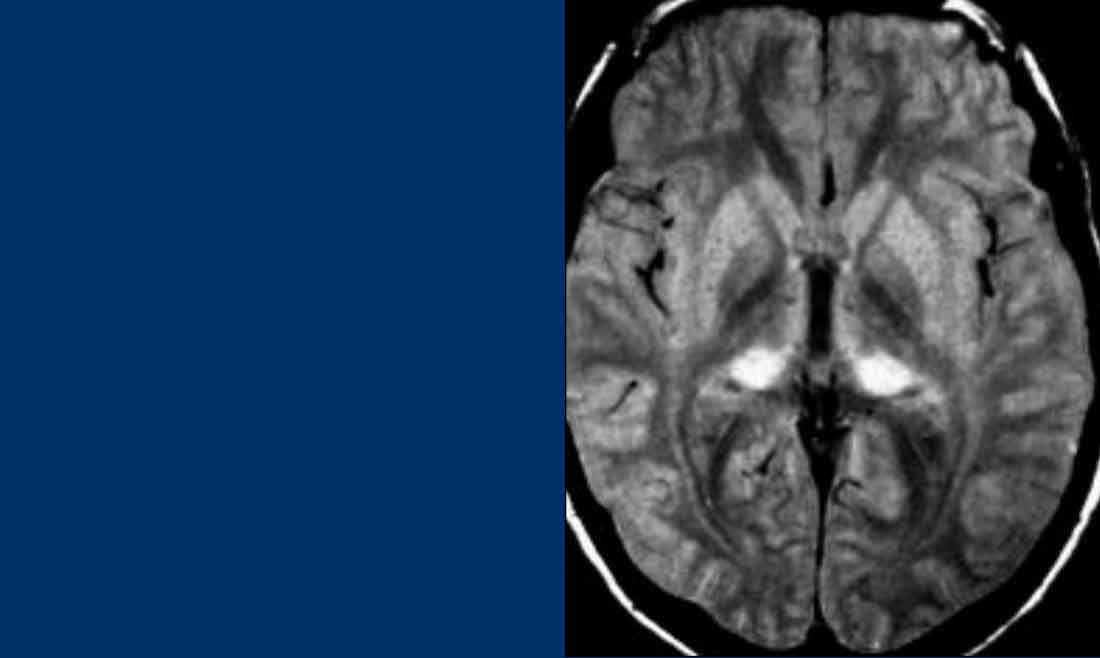
New variant CJD
New variant of CJD is also known as the 'mad cow disease' (12).
It is a disease fortunately hardly encountered anymore.
In this variant the changes are seen in the posterior part of the thalamus, called the pulvinar.
Huntington’s disease
Huntington’s disease is an inherited neurodegenerative disorder with an autosomal dominant pattern of inheritance, though de novo mutations may also occur.
Clinically, it can manifest with early-onset dementia, choreoathetosis, and psychotic symptoms.
Neuroimaging typically demonstrates:
- Characteristic atrophy of the caudate nucleus
- Secondary enlargement of the frontal horns of the lateral ventricles
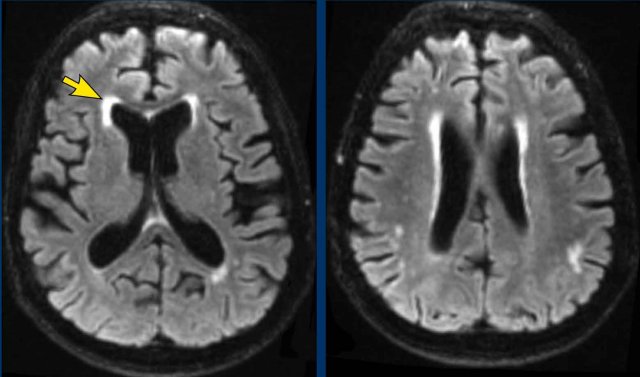
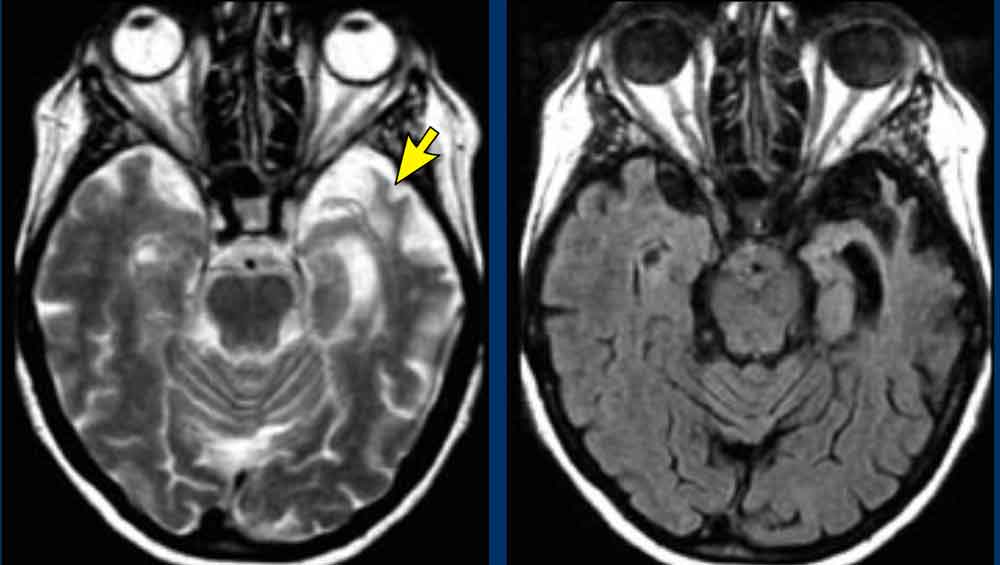
CADASIL
CADASIL is another hereditary disease which may present with a progressive cognitive dysfunction.
Other presenting symptoms include migraines, stroke-like episodes and behavioral disturbances.
It affects the small vessels of the brain.
Confluent white matter hyperintesities in the frontal and especially anterior temporal lobes in combination with lacunar infarcts and microbleeds are seen on imaging.
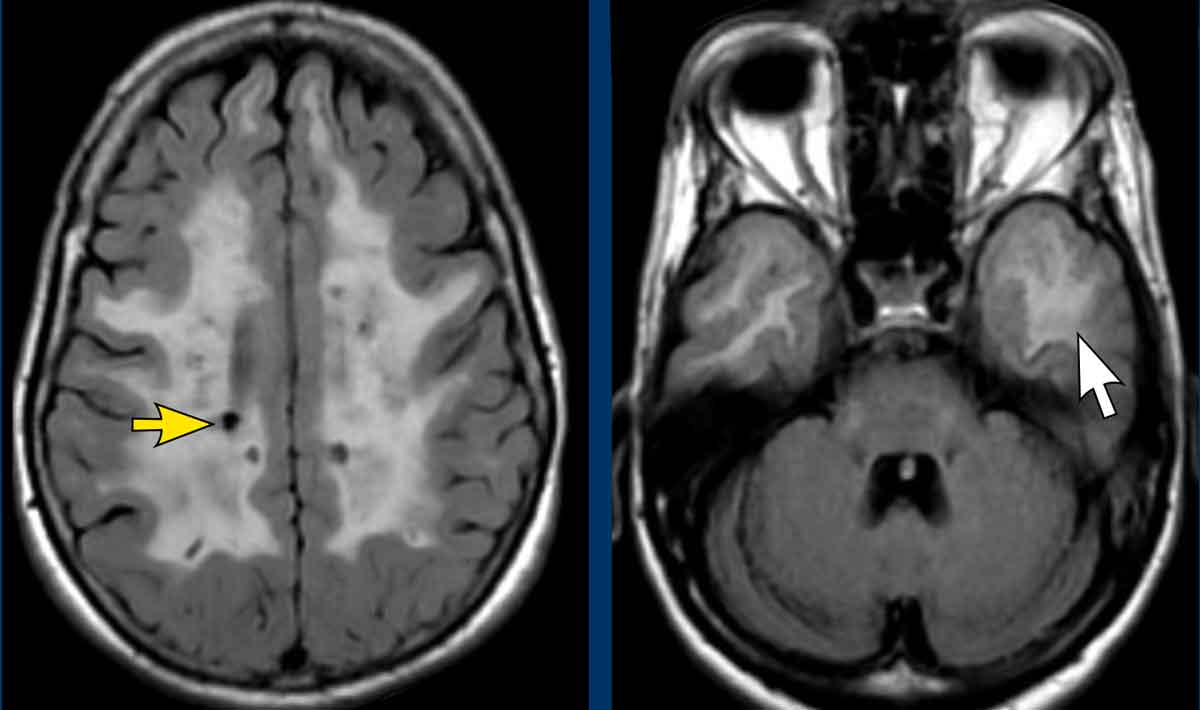
Images
Classic findings in CADASIL
- confluent white matter hyperintensities with lacunar infarcts (yellow arrow)
- Involvement of the anterior temporal lobes (white arrow)
Traumatic Brain Injury
Long-term sequelae of traumatic brain injury, such as cerebral contusions and diffuse axonal injury (DAI), may include cognitive impairment.
Therefore, when evaluating MRI scans for dementia, frontobasal or temporal parenchymal loss or *T2-weighted "black dots"**—characteristic of DAI—in a patient with a history of trauma must be carefully considered.
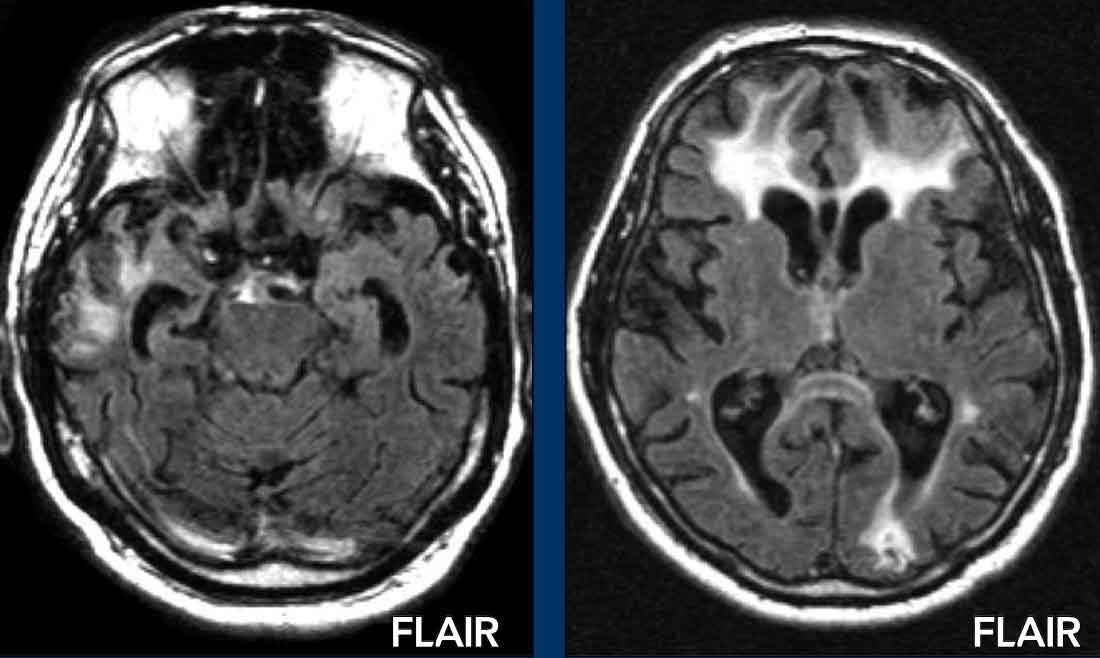
Example
FLAIR imaging reveals classic post-traumatic tissue loss with gliosis in the bilateral frontal lobes, left occipital lobe, and right temporal lobe.
ARIA
ARIA (Amyloid-Related Imaging Abnormalities) is a side effect of amyloid-β–targeting monoclonal antibodies used in Alzheimer’s disease treatment.
These drugs clear amyloid plaques, which can temporarily increase blood-brain barrier permeability, leading to MRI-detectable changes.
ARIA has two forms, which may occur separately or together.:
- ARIA-E (edema/effusion)
- ARIA-H (hemosiderin deposits)
Adult-onset leukoencephalopathy (ALSP)
ALSP (CSF1R-related leukoencephalopathy) is a rare, autosomal dominant white matter disorder caused by CSF1R gene mutations, leading to microglial dysfunction and progressive cognitive, psychiatric, and motor decline.
Onset typically occurs in adults aged 40–60 years.
Other Imaging Techniques
PET imaging
Role of PET Imaging in Alzheimer’s Disease Diagnosis
In addition to clinical findings, CSF analysis, and MRI, PET imaging plays a valuable role in diagnosing Alzheimer’s disease (AD).
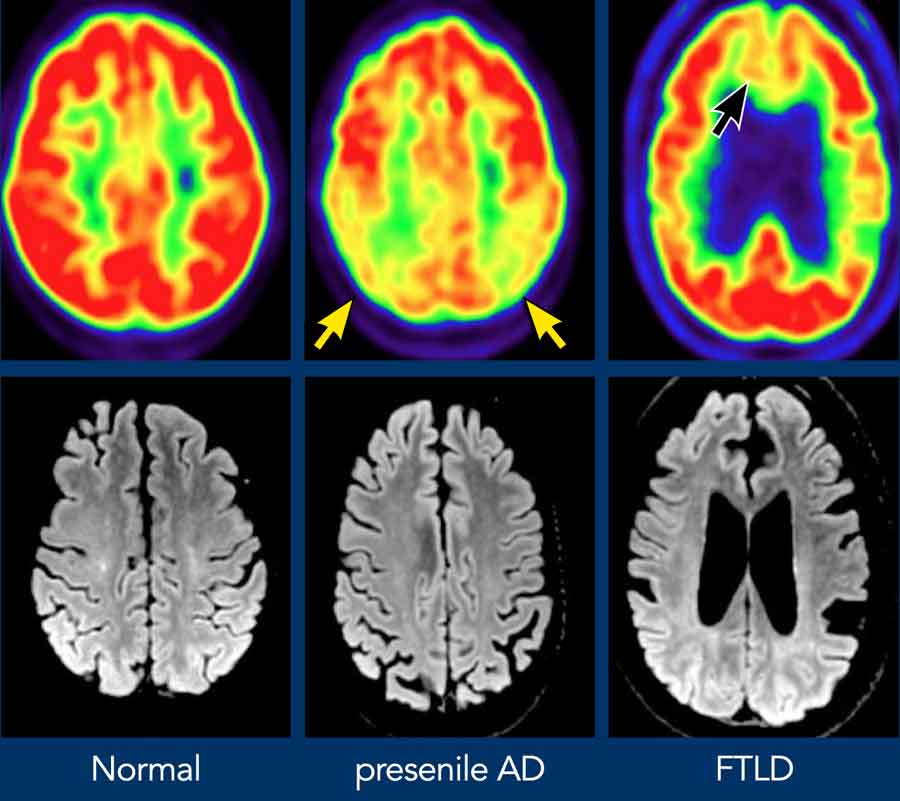
- FDG-PET Findings in AD:
- Demonstrates hypometabolism in the temporoparietal regions and/or the posterior cingulate cortex.
- Helps differentiate AD from frontotemporal dementia (FTD), which typically exhibits frontal hypometabolism on FDG-PET.
Image Description
The provided images include FDG-PET (top row) and axial FLAIR images of:
- A normal subject
- A patient with Alzheimer’s disease (AD)
- A patient with frontotemporal dementia (FTD)
Key Observations:
- In AD, there is decreased metabolism in the parietal lobes (indicated by yellow arrows).
- In FTD, there is frontal hypometabolism (indicated by red arrows).
Amyloid PET Tracers in Alzheimer’s Disease (AD):
- Early detection: Amyloid-PET abnormalities may appear >10 years before clinical onset.
- Diagnostic value:
- High negative predictive value: A normal amyloid-PET scan effectively rules out AD.
- CSF amyloid offers comparable diagnostic accuracy.
- Plasma markers: Currently not available for clinical use.
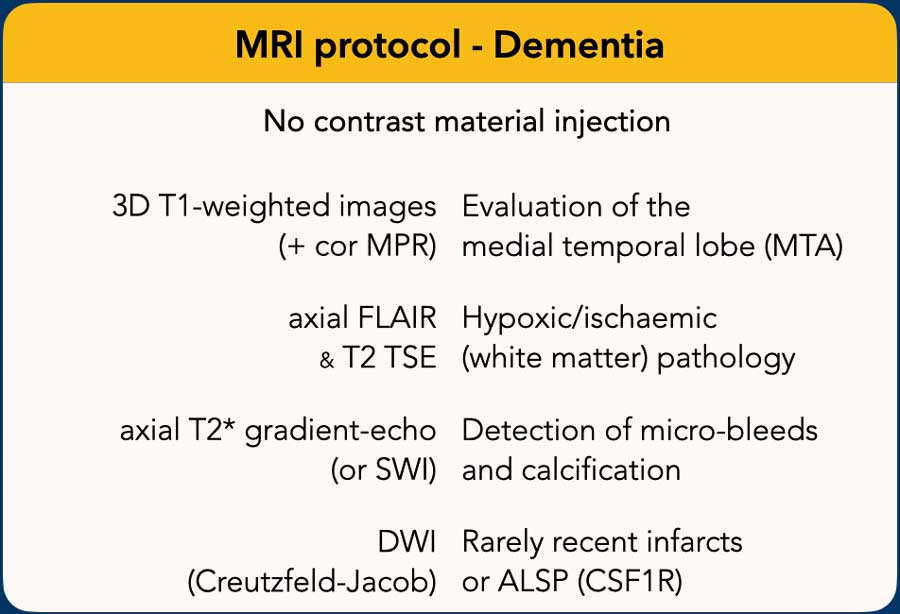
MRI Protocol for Neurodegenerative and Vascular Assessment
1. Coronal-Oblique T1-Weighted Images
- Purpose: Assessment of medial temporal lobe and hippocampal atrophy.
- Plane: Orthogonal to the long axis of the hippocampus, oriented parallel to the brainstem.
- Technique: Thin-section images, ideally reformatted from a sagittal 3D T1-weighted sequence covering the entire brain.
- Additional Use: Sagittal reconstructions allow evaluation of midline structures and parietal atrophy, relevant in certain neurodegenerative disorders.
2. FLAIR Images
- Purpose: Evaluation of global cortical atrophy (GCA), vascular white matter hyperintensities, and infarctions.
3. T2-Weighted Images
- Purpose: Detection of infarctions, particularly lacunar infarctions in the thalamus and basal ganglia, which may be subtle or missed on FLAIR.
4. T2-Weighted Images*
- Purpose: Identification of microbleeds (e.g., in cerebral amyloid angiopathy), as well as calcifications and iron deposition.
5. Diffusion-Weighted Imaging (DWI)
- Purpose: Supplemental sequence for young patients or cases of rapidly progressive neurodegenerative disorders.
- Differential Considerations: Useful in distinguishing vasculitis and Creutzfeldt-Jakob disease (CJD).
CT imaging
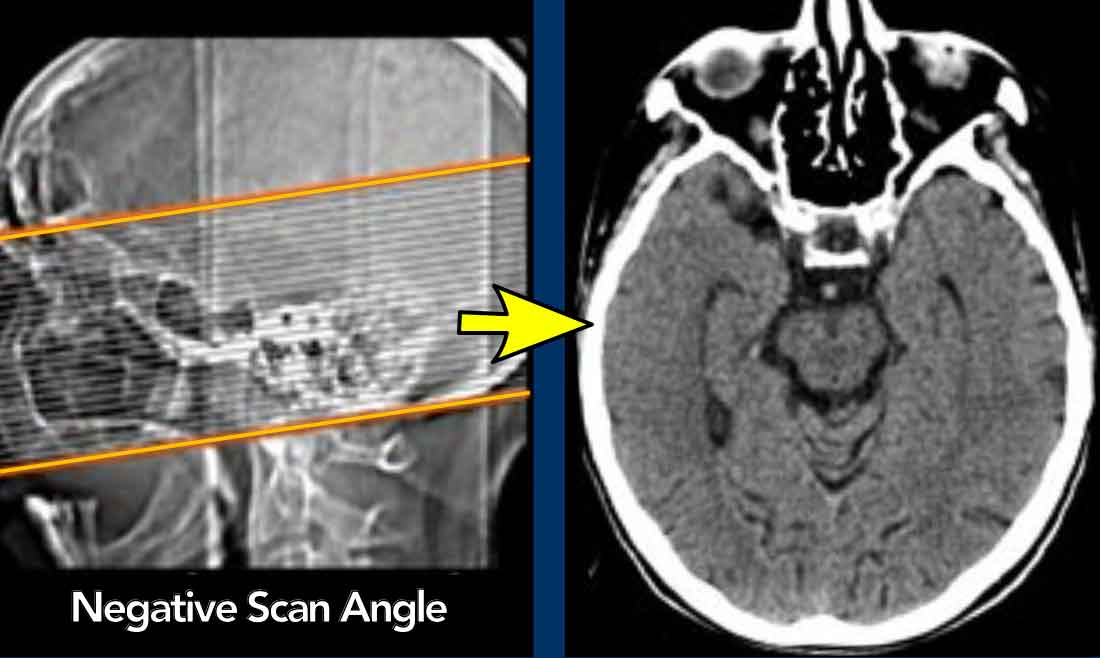
CT Protocol for Cognitive Decline Assessment
CT imaging may be utilized when MRI is contraindicated or when the primary objective is to exclude surgically treatable causes of cognitive decline.
- Scan Plane: In the transverse plane, the scan angle should be parallel to the long axis of the temporal lobe.
Images
CT with negative scan angle for optimal vizualisation of the hippocampus in the transverse plane
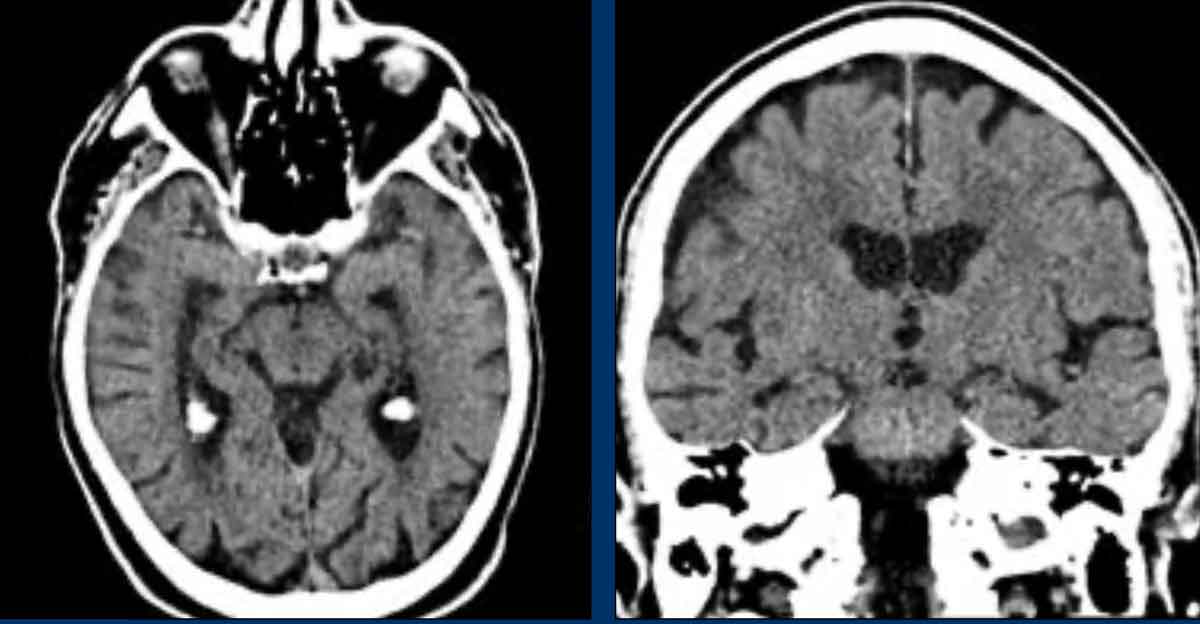
- Multi-detector CT allows for coronal reformations to be reconstructed perpendicular to the long axis of the temporal lobe, optimizing visualization of the hippocampus.