Shoulder Ultrasound
Mohamed Salah Ayyad¹, Alrawy Ali Mohammad¹, Khaled Taha¹ and Robin Smithuis²
¹Radiology department of the faculty of Medicine - Mansoura University, Egypt and ²Alrijne hospital in Leiden, the Netherlands
Publicationdate
This article is currently in preparation. Once it is finalized, we will provide an announcement on the homepage.
This article serves as an introduction to shoulder ultrasound. Ultrasound is a non-invasive, easily accessible imaging technique that allows for thorough evaluation of the shoulder, including dynamic assessment in patients with impingement.
We will review the sonographic anatomy of the shoulder, outline the examination protocol—including proper patient positioning—and discuss common pathologies encountered during shoulder ultrasound.
Anatomy
Glenohumeral Joint Stabilization
A key stabilizer of the glenohumeral joint is the rotator cuff, which is composed of the subscapularis tendon anteriorly, the supraspinatus tendon superiorly, and the infraspinatus and teres minor tendons posteriorly.
Of these posterior tendons, only the infraspinatus tendon is partially visible in this illustration.
The normal anatomy is also discussed here.
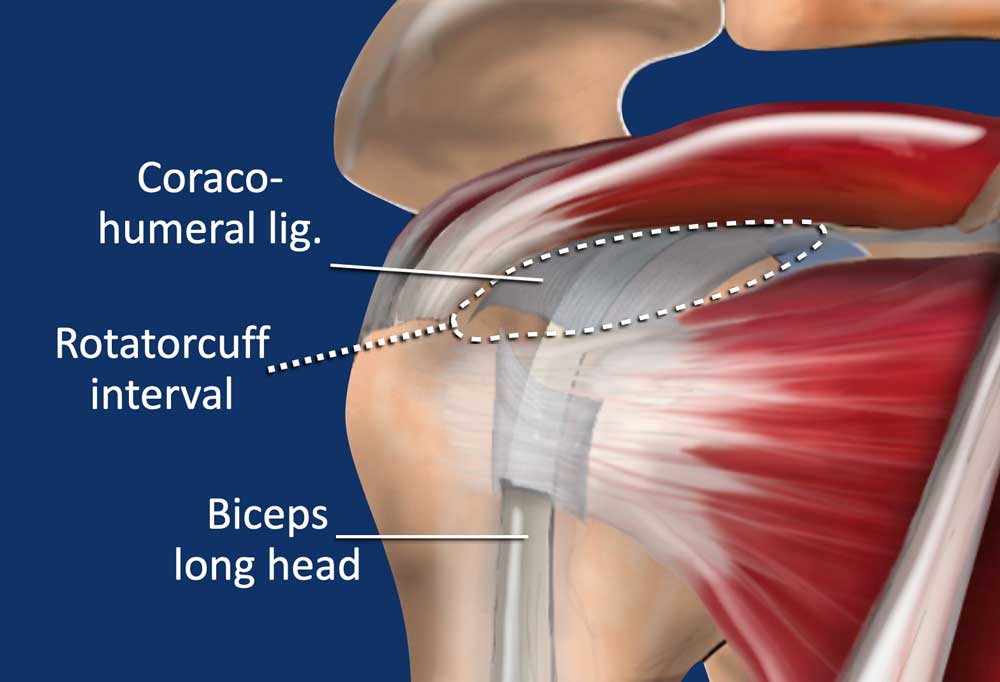
Rotator cuff interval
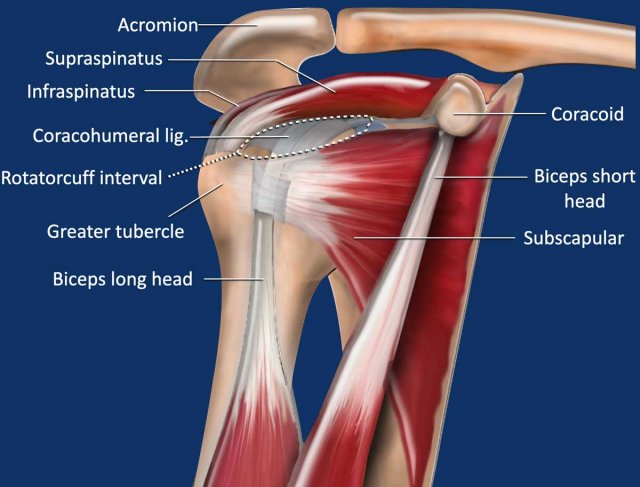
The rotator cuff interval is a distinct gap in the rotator cuff located between the superior edge of the subscapularis tendon and the anterior edge of the supraspinatus tendon.
In this interval, the humeral head is not covered by the rotator cuff but is instead covered by the intra-articular portion of the long head of the biceps tendon, which is stabilized by the coracohumeral ligament.
When assessing for supraspinatus tendon tears, it is crucial to examine its attachment to the greater tuberosity, particularly along the posterior border of the rotator cuff interval.
This anterior region of the supraspinatus tendon is a common site for partial-thickness tears, known as "rim-rent tears."
The biceps tendon is stabilized by the capsuloligamentous complex, referred to as the biceps pulley, which consists of the superior glenohumeral ligament, the coracohumeral ligament, and the distal insertion of the subscapularis tendon.
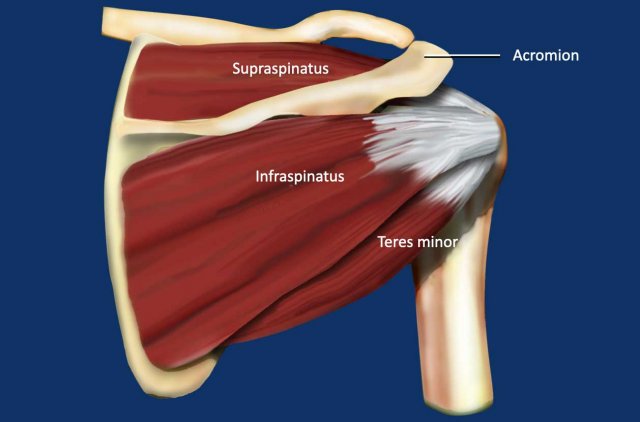
This posterior view of the shoulder highlights the supraspinatus, infraspinatus, and teres minor muscles and their associated tendons.
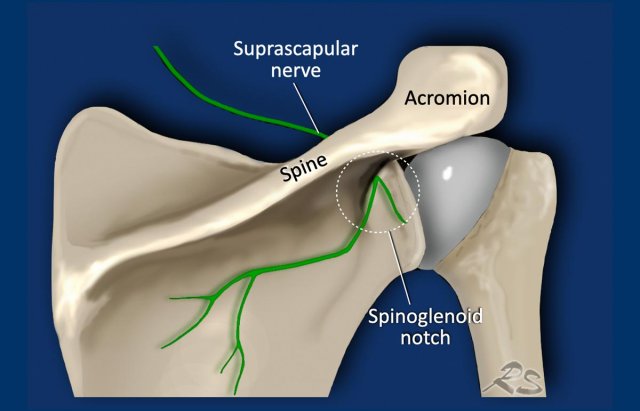
Spinoglenoid notch
The spinoglenoid notch is the anatomical region located between the lateral base of the scapular spine and the glenoid process.
It serves as a connection between the supraspinatus and infraspinatus fossae and allows passage for the suprascapular nerve and artery.
Ganglion cysts can develop in this area, potentially compressing the suprascapular nerve and leading to shoulder pain and atrophy of the infraspinatus muscle.
These cysts are often secondary to tears in the posterosuperior glenoid labrum.
Standard Ultrasound Examination
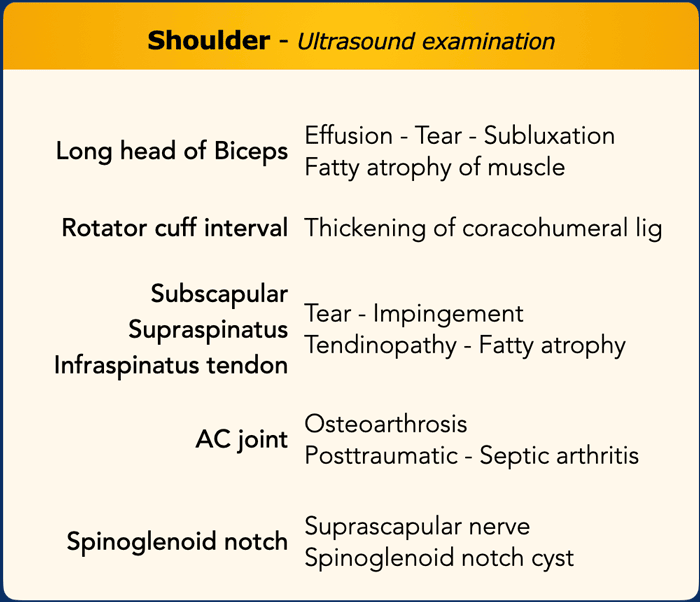
Ultrasound Examination of the Shoulder
A high-resolution linear probe (≥10 MHz) is typically used for shoulder ultrasound. Occasionally, a curvilinear probe (3.5 MHz) is employed to provide a broader view of the glenohumeral joint.
The examination generally begins with the long head of the biceps (LHB) tendon, assessing for effusion, tears, or subluxation.
Fatty atrophy may also be observed, either within the muscle belly or at the myotendinous junction.
Next, the tendons of the subscapularis, supraspinatus, and infraspinatus muscles are evaluated, with particular attention to identifying tears.
The examination can be expanded to include the acromioclavicular (AC) joint, spinoglenoid notch, posterior labrum, and the glenohumeral joint.
A checklist (see Table) is recommended to ensure all structures have been thoroughly examined.

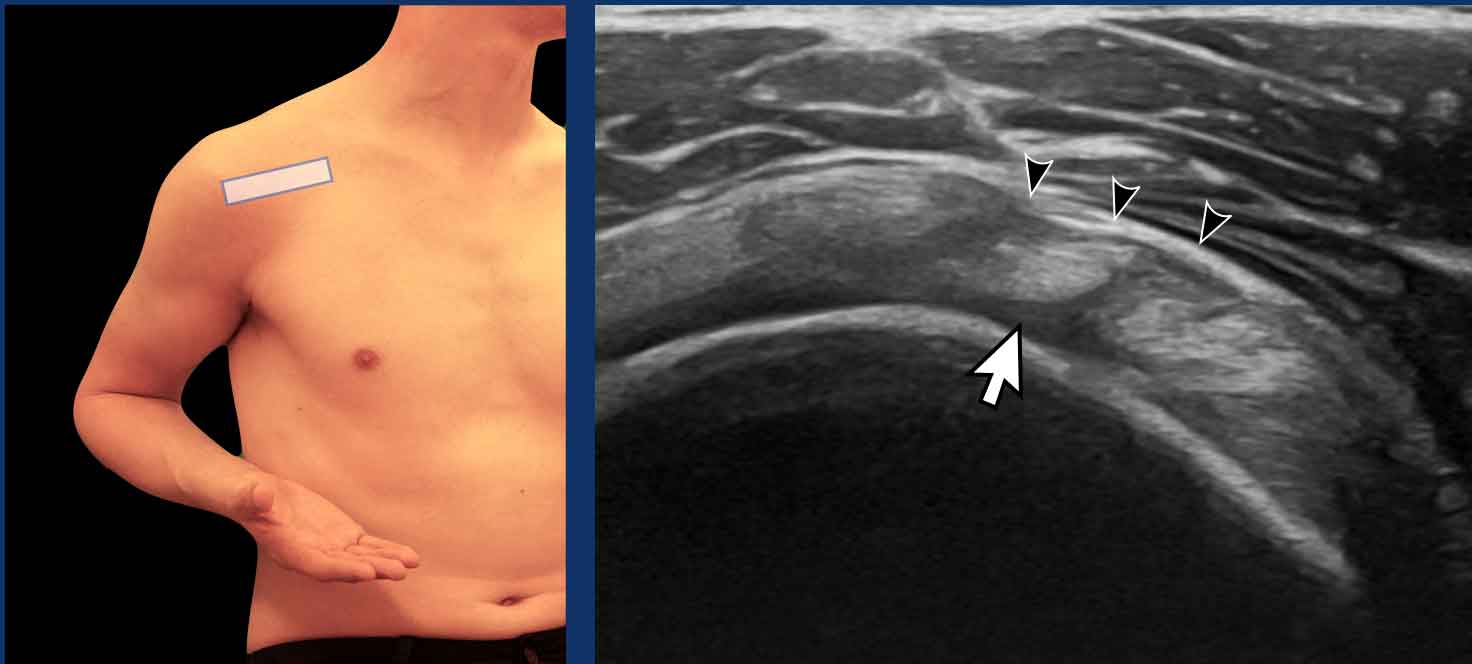
Long head of the biceps tendon
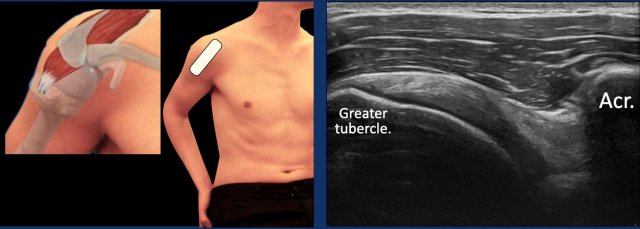
The LHB tendon is best visualized by positioning the probe over the muscle belly of the biceps brachii in the upper arm and moving proximally to the myotendinous junction and the tendon.
The patient’s forearm should be supinated and slightly internally rotated toward the contralateral knee.
In this position, the LHB appears as a rounded structure with a fibrillary echotexture (black arrow) situated within the intertubercular groove (white arrowheads).
Video of the examination of the long head of the biceps in the transverse plane.
Click in the left upper corner for a full screen view.
 Anisotropy of the LHB
Anisotropy of the LHB
Anisotropy
Anisotropy is an artifact that occurs when the ultrasound beam is not perpendicular to the LHB tendon. This misalignment leads to reduced sound wave reflection, resulting in a loss of resolution and a darkened, hypoechoic appearance of the structure (black arrow). In some cases, this may give the impression that the LHB tendon is dislocated from the intertubercular groove.
To correct for anisotropy, reposition the transducer so that the ultrasound beam is perpendicular to the tendon. The LHB will then regain its typical echogenic, fibrillary appearance (white arrow).
It is important to note that anisotropy can also affect other structures, such as the subscapularis tendon in this image, which similarly appears anechoic due to this artifact.
Rotator cuff interval
When the patient moves the elbow slightly backward while maintaining forearm supination, the intra-articular portion of the biceps tendon within the rotator cuff interval becomes more clearly visualized. This positioning is referred to as the Jugger’s position (see figure).
Image
Transverse view of the rotator cuff interval.
The LHB (arrow) is located between the subscapularis tendon anteriorly and the supraspinatus tendon posteriorly.
The LHB is covered by the coracohumeral ligament (arrowheads).
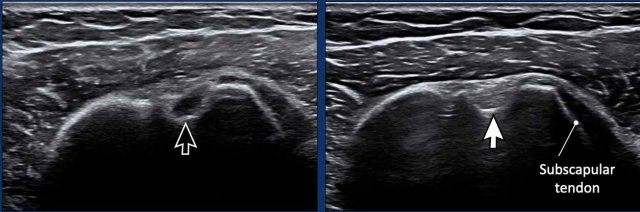
Subscapular tendon
The arm is positioned alongside the trunk, with the elbow flexed at a 90º angle between the arm and forearm.
The forearm is placed in supination and external rotation.
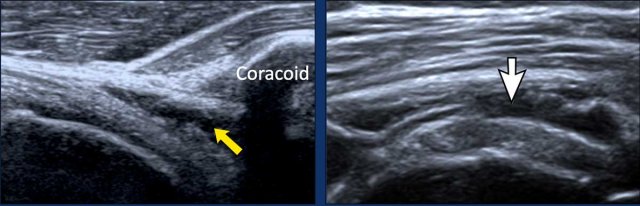
The ultrasound probe is positioned medially to visualize the subscapularis (SSC) tendon as it passes beneath the coracoid process.
Video of normal subscapular movement
During internal and external rotation of the forearm, the whole tendon should be seen sliding under the coracoid (see video).
Impingement is noted when there is incomplete or delayed passage of the tendon (see chapter on impingement).
Double click on the video for a full screen view.
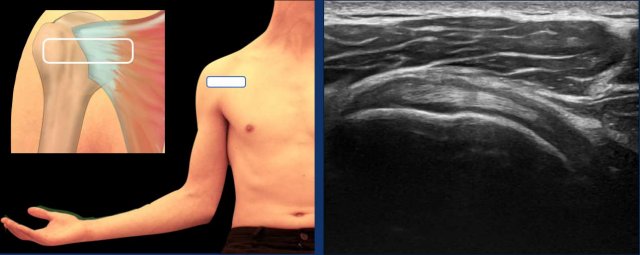
Supraspinatus tendon
The optimal position for examining the supraspinatus tendon is the modified Crass position. In this position, the patient is instructed to place their hand on the ipsilateral hip or toward their back pocket (see figure).
An alternative is the Crass position, in which the patient places their arm in internal rotation behind the back.

Infraspinatus tendon
Examining the infraspinatus tendon can be challenging due to the difficulty in distinguishing it from the supraspinatus tendon. The optimal position for visualizing the infraspinatus tendon is to have the patient place their hand on the contralateral shoulder.
Position the probe in the same orientation as for examining the supraspinatus tendon. Once the supraspinatus is in view, gradually move the probe inferiorly. A subtle gap will become evident, followed by the smaller, distinct outline of the infraspinatus tendon.
Video of the infraspinatus tendon.
Double click on the video for a full screen view.
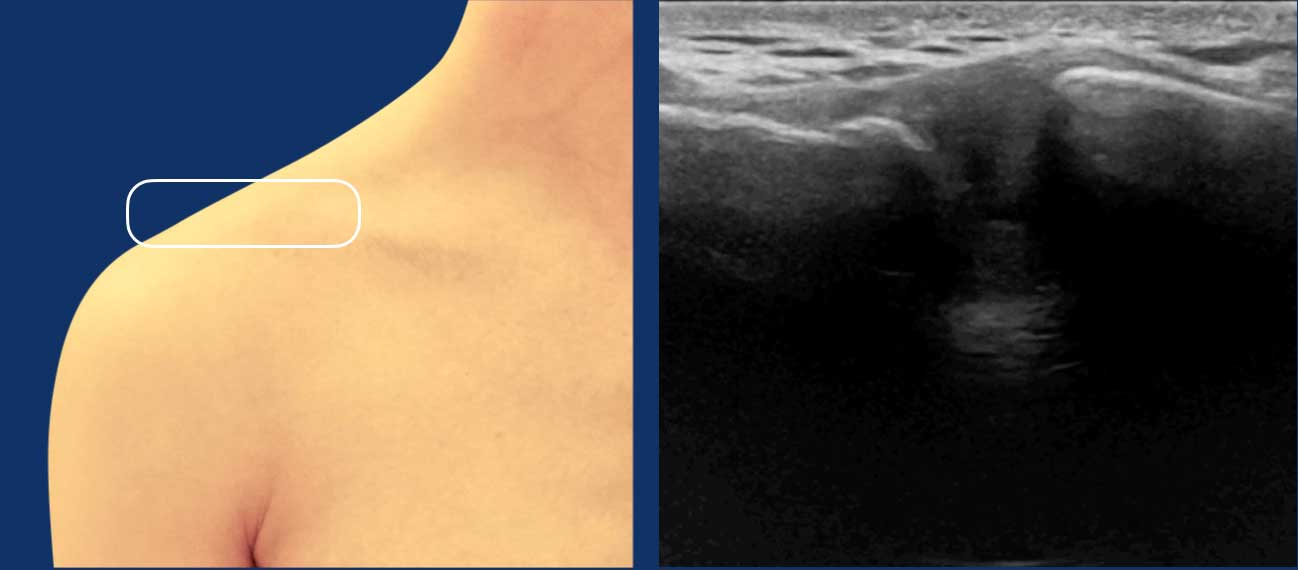
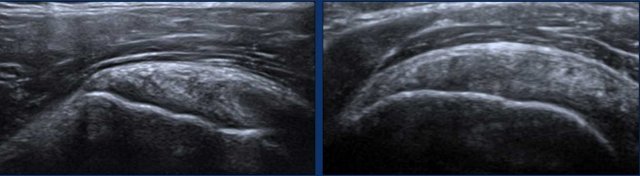
Acromioclavicular joint
The acromioclavicular joint is easily appreciated by palpating the bony projection and then placing the probe over it.
A normal acromioclavicular joint shows a smooth
contour of the bony articular surfaces.
Spinoglenoid notch
Identify the scapular spine as a hyperechoic bony landmark.
Move the probe laterally until you locate the spinoglenoid notch, which is situated between the lateral scapular spine and the glenoid process.
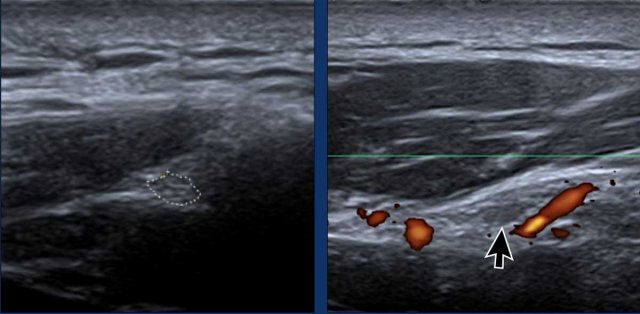
The
suprascapular nerve appears as a hypoechoic tubular structure with a fascicular pattern (arrow).
Power Doppler can be beneficial to trace the suprascapular vessels in order to find the nerve.
Examine for ganglion cysts, which may appear as hypoechoic, fluid-filled structures compressing the suprascapular nerve.
These cysts are often associated with tears of the posterosuperior glenoid labrum.
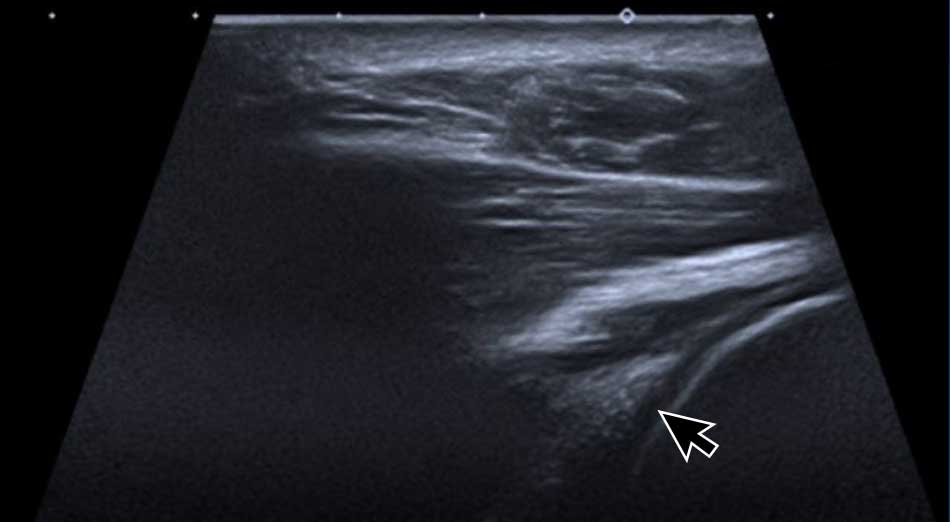
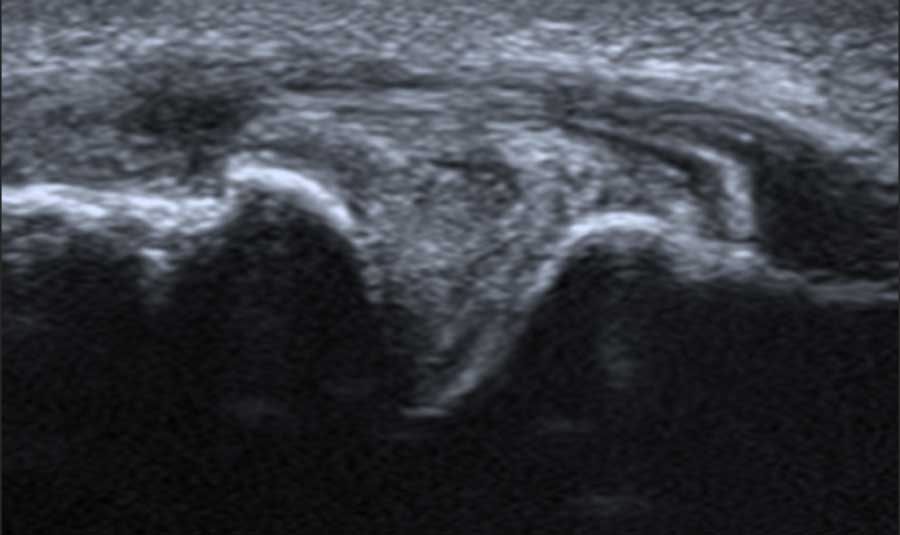
Posterior labrum and glenohumeral joint
The posterior labrum can be examined by placing the probe
at the posterior aspect of the glenohumeral articulation.
The
labrum is seen as a triangular echogenic structure, which is more echogenic than the
adjacent cartilage (arrow).
Pathology
Biceps tendinopathy
Images
Two examples of a thickened long head of the biceps tendon.
Notice the irregular echo-pattern especially on the image on the right.
There is hypervascularity and some surrounding fluid (arrows).
Tear of the long head of the biceps (LHB)
The most common site of injury to the LHB is at the myotendinous junction and the adjacent portion of the tendon.
LHB tears are readily identified on ultrasound as anechoic fluid disrupting the continuity of the muscle fibers.
The echogenicity of the fluid varies depending on the chronicity of the injury:
- Acute tears typically appear as anechoic fluid.
- Chronic tears may demonstrate echogenic debris or reflective echoes within the fluid.
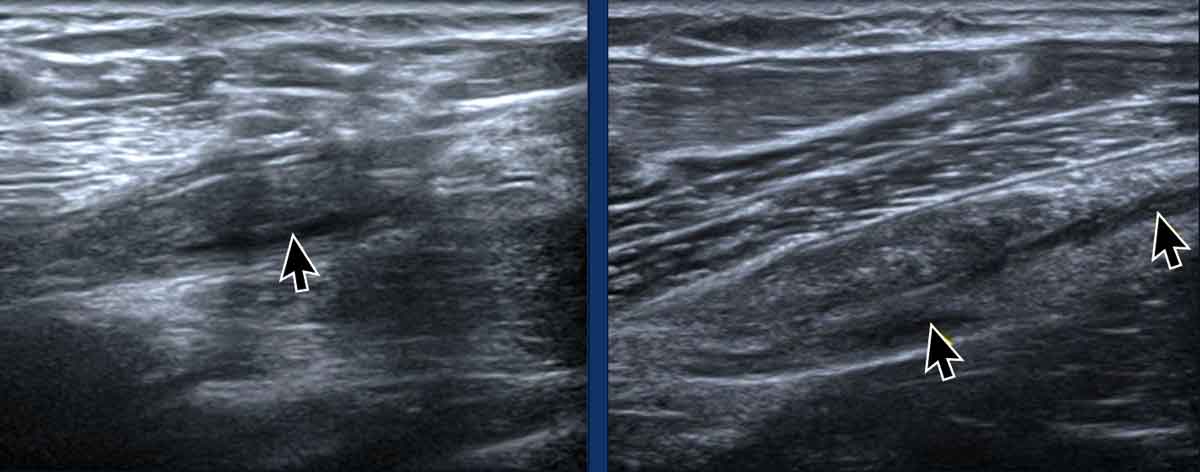
Images
The accompanying examples illustrate tears at the myotendinous junction of the LHB. The tears appear completely anechoic, consistent with acute injuries.
Biceps tendon dislocation
The long head of the biceps (LHB) tendon is normally located centrally within the bicipital groove. An abnormal, eccentric, or displaced positioning of the tendon may indicate laxity or rupture of the biceps pulley.
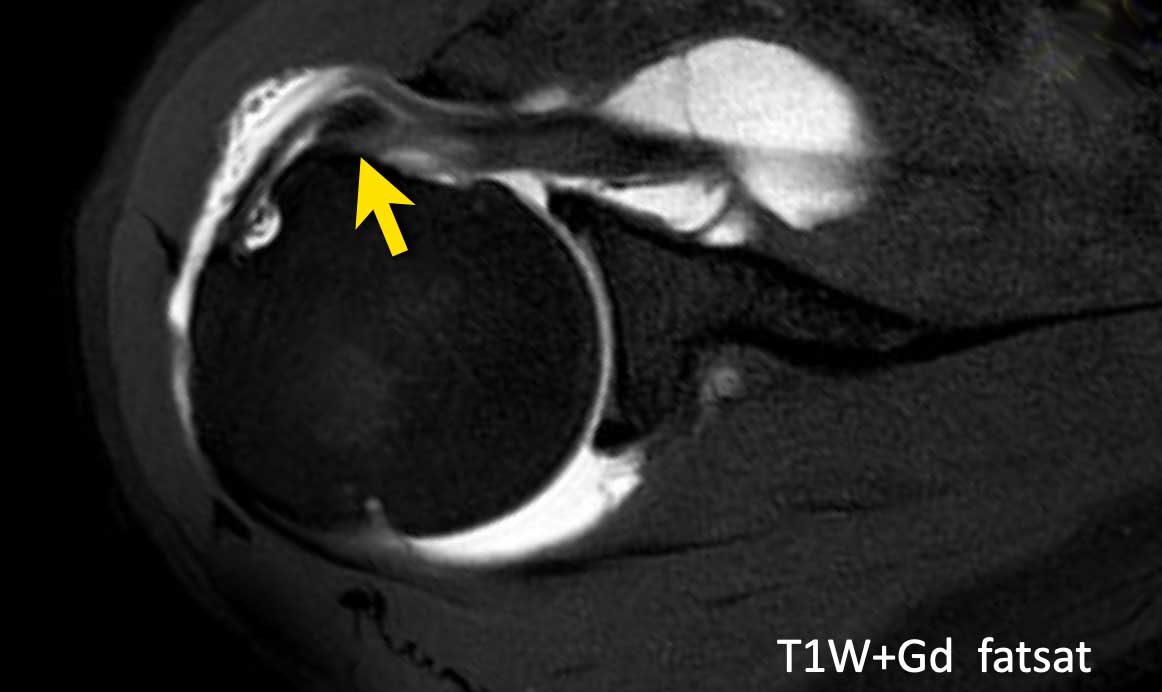
Imaging Findings
MR Arthrography with Axial T1-Weighted Fat-Suppressed Image: The biceps tendon is medially displaced within the subscapularis tendon, as indicated by the arrow.
Continue with ultrasound images...
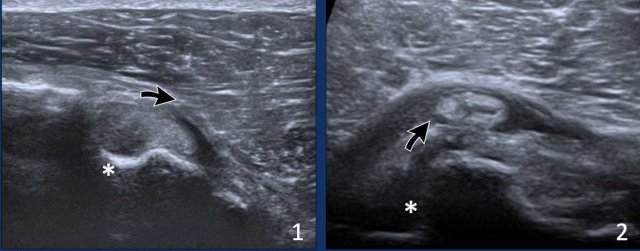
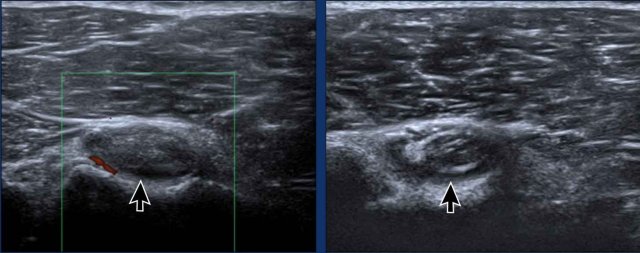
Images
- Eccentric position of the long head of the biceps tendon due to laxity of the biceps pulley.
- Dislocation of the biceps tendon. Notice the empty bicipital groove (asterix)
Rotator cuff tears
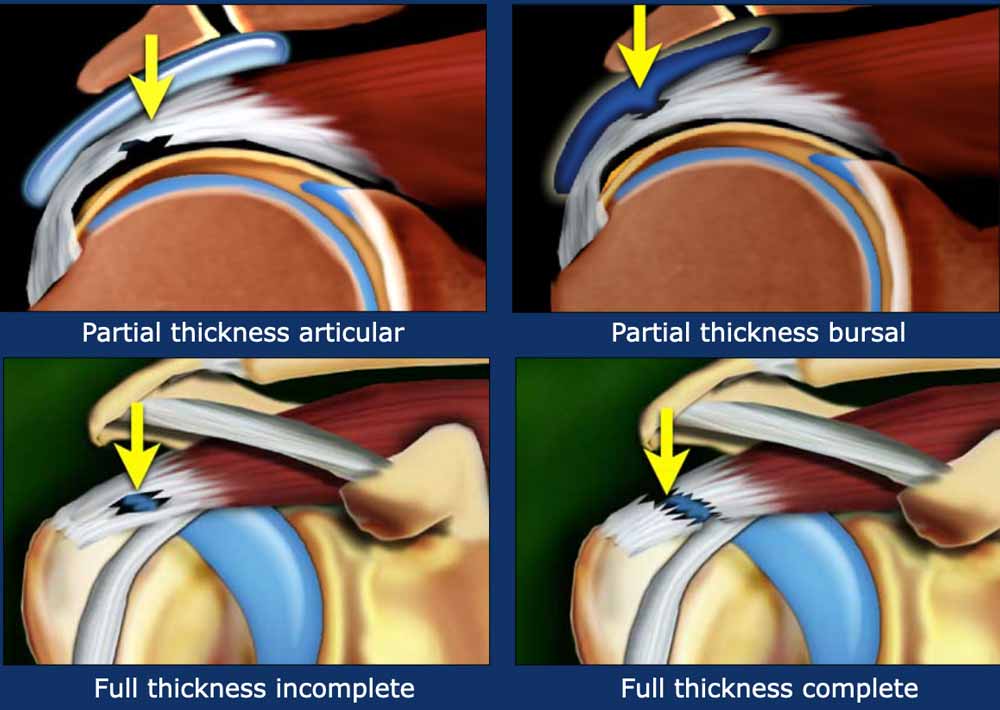
Partial thickness tears
Partial thickness tears involve only a part of the tendon and do not involve the full thickness.
It can be located on the articular or on the bursal side (figure).
An intrasubstance tear is also a partial thickness tear.
Full thickness tears
Full thickness tears can be complete or may involve only a part of a tendon.
This is called an incomplete full-thickness tear and is just like a hole in a tendon (figure).
Full thickness tears
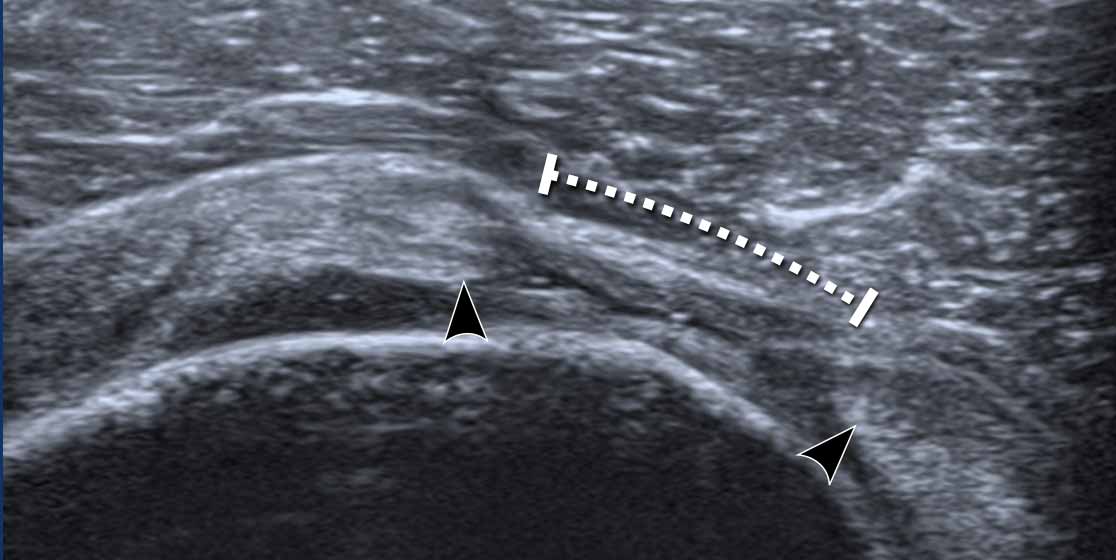
This image shows a complete full thickness tear of the supraspinatus tendon.
There is a small hypoechoic fluid collection.
Both tendon edges are blunt and retracted (arrowheads).

Here another example of a ful thickness tears of the supraspinatus tendon.
The gap is filled with some fluid from the glenohumeral joint (arrow)
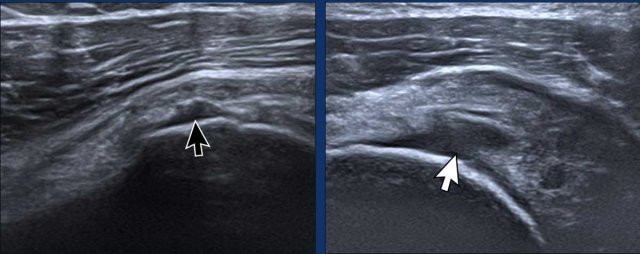
Partial thickness tears
Here two examples of a partial tear on the articular side.
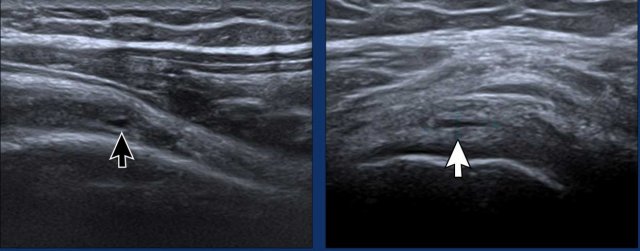
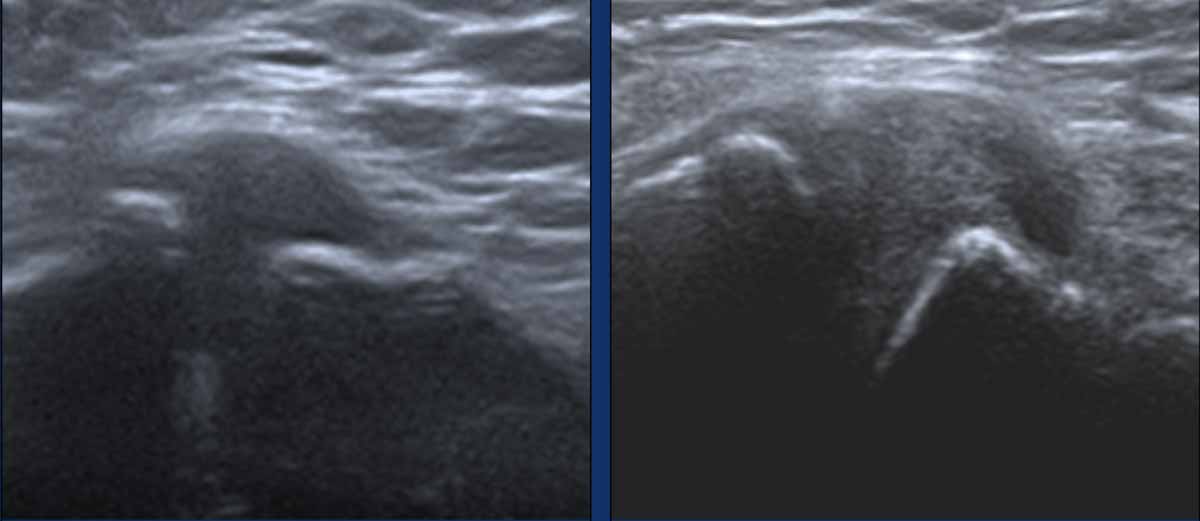
Intrasubstance tears
Intrasubstance tears are partial-thickness tears that do not extend to either the articular or bursal surfaces of the tendon.
Images
The images demonstrate two examples of small intrasubstance tears.
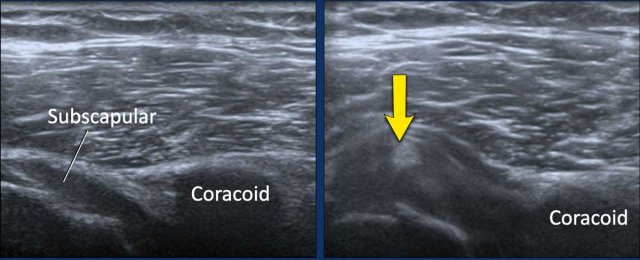 Image during exoratation (left) and endorotation (right)
Image during exoratation (left) and endorotation (right)
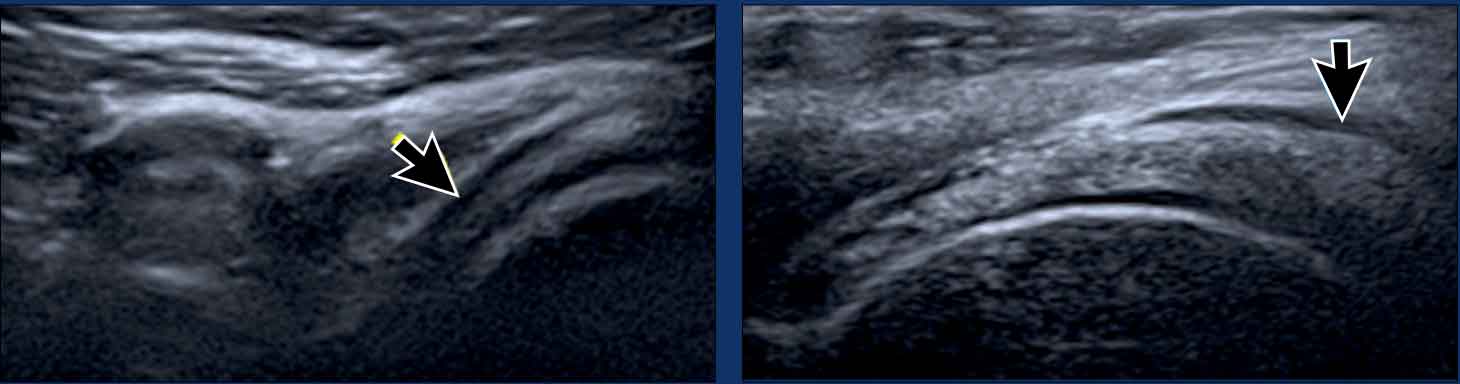
Impingement
During endorotation a normal subscapular tendon should show almost complete passage underneath the coracoid process.
Impingement is suspected when a residual portion of the tendon is still visible during maximum endorotation.
Images
During endorotation there is incomplete passage under the coracoid and buckling of the subscapular tendon.
Video of subscapular impingement.
Double click on the video for a full screen view.
Notice the limited range of motion.
This video is of a 58-year-old female experiencing severe pain and limited movement in her shoulder.
In full external rotation, a large subcoracoid bursa bulges over the subscapular tendon.
Double click on the video for a full screen view.
Notice the limited range of motion.
Tendinopathy
The term tendinopathy is used rather than tendinitis because there is no active inflammation, but instead it is a degenerative process with mucoid degeneration.
The tendon is frequently thickened and may show hypoechoic striated areas.
Images
Thickened supraspinatus tendon with an inhomogeneous echo pattern.
Calcific tendinopathy
Calcific tendinopathy occurs when calcium deposits accumulate within the tendons. While this condition can affect tendons throughout the body, it most frequently involves the rotator cuff tendons of the shoulder. These calcium deposits may become inflamed, leading to pain.
Imaging Findings:
- Significant thickening of the supraspinatus tendon with large calcifications producing an extensive posterior acoustic shadow.
- A small calcification observed within the supraspinatus tendon.
Bursitis
The normal bursal space is collapsed and barely distinguishable by ultrasound (arrows).
Acute bursitis appears sonographically as
distension of the bursa (yellow arrow).
Chronic bursitis may
show a thick wall (white arrow).
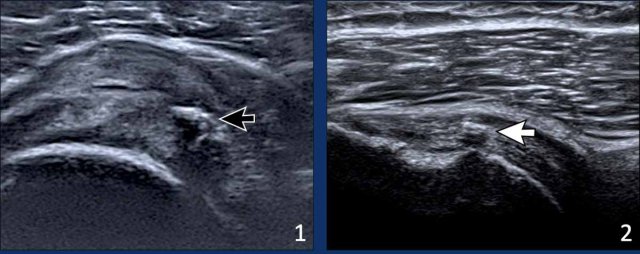
AC pathology
Osteoarthritis
Diagnosing symptomatic osteoarthritis of the acromioclavicular joint can be difficult, as radiographic and ultrasound findings of joint degeneration are commonly seen in adults and have a poor correlation with clinical symptoms.
Images
Osteoarthritis of the AC joint with cortical irregularity and bulging of the capsule.
AC-arthritis
This image is of a 19-year-old male athlete who sustained an injury during a wrestling match.
There were no signs of septic arthritis and he was diagnosed with post-traumatic arthritis.
He improved with anti-inflammatory medication and rest.