Renal Tumors in Children
Suzanne Spijkers, Annemieke Littooij, Martine van Grotel and Erik Beek
Department of Radiology and Nuclear Medicine, University Medical Center Utrecht and Princess Máxima Center for Pediatric Oncology in Utrecht
Wilms tumor comprises the vast majority of renal neoplasms in young children and resection with neoadjuvant chemotherapy is the treatment of choice.
Most other renal tumors cannot be reliably distinguished from Wilms tumor at imaging, but some features may suggest an alternative diagnosis, which in some cases can lead to the decision to adjust the treatment or in some cases to perform a biopsy before start of pre-operative treatment.
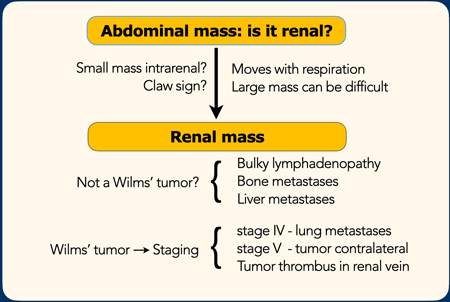
The role of imaging in children with a possible renal tumor is first to determine whether the mass originates in the kidney.
The next step is to look for signs that would make you consider an alternative diagnosis instead of a Wilms tumor.
The final step is staging.
In this article we will discuss common and some less common renal tumors and include some malignancies that can appear as a primary renal tumor, like lymphoma, neuroblastoma and leukemia.
Introduction
Role of Imaging
- Determine whether a mass is a renal mass.
In most cases ultrasound can determine whether a mass originates from the kidney. Especially look for the claw sign.
In large masses it can be difficult and MRI or CT can solve the problem.
A large neuroblastoma, that compresses or invades the kidney can look like a renal tumor.
- Is it a Wilms' tumor or could it be something else?
If it is a renal mass, then in most cases it will be a Wilms' tumor, especially in the age group 6 month to nine years. For the differential diagnosis, look for signs that are uncommon in a Wilms' tumor, like bulky lymphadenopathy (RCC or lymphoma) or liver and bone metastases (Clear cell sarcoma). - Staging
When a Wilms' tumor is the most likely diagnosis, but also in other tumors staging is the next step.
Especially look for tumor thrombus, lung metastases (stage IV) and tumor in the contralateral kidney (stage V)
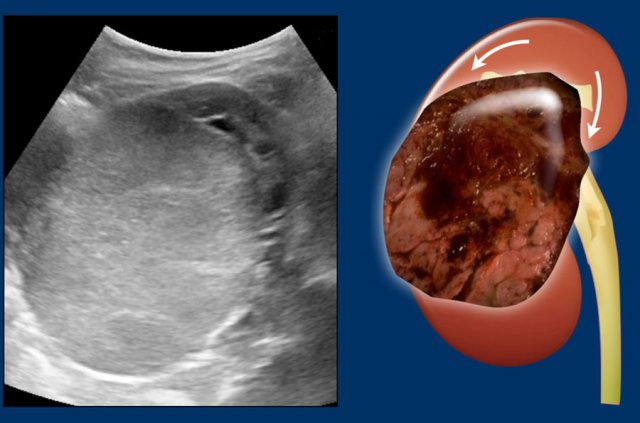 Claw sign
Claw sign
Claw sign
This sign in renal tumors is useful in determining that the tumor arises from the kidney rather than is located adjacent to the kidney and distorts the outline.
The claw sign refers to the sharp angles on either side of the mass, which the surrounding normal parenchyma forms when the mass has arisen from the kidney.
Images
Left sided Wilms' tumor in a one-year-old girl.
The remnant of the kidney is draped over the tumor, the “claw sign”.
Management
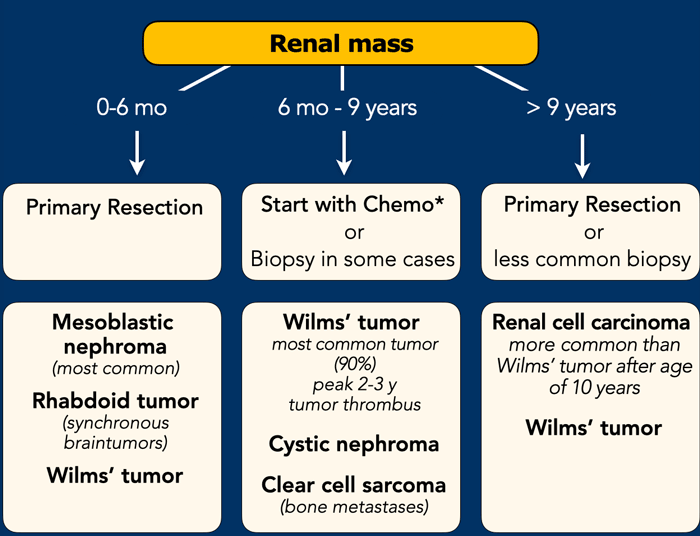
Imaging plays a limited role in determining the exact nature and management of a renal tumor in children, since almost all pediatric renal tumors will be resected and most tumors will be a Wilms tumor.
Age at presentation is a far more important predictor of tumor type.
0-6 months-old
Besides Wilms tumor, the differential diagnosis comprises two tumors that occur predominantly in infants: congenital mesoblastic nephroma and rhabdoid tumor of the kidney (MRTK). Both tumors are treated with primary resection. Therefore, renal tumors in infants below six months are primarily resected if possible.
6-months – 9 years
A renal tumor in children in this age group is considered a Wilms tumor without histological confirmation.
>9 years
In children above 9 years-old in most cases a primary nephrectomy is performed.
A renal cell carcinoma (RCC) is more common in this age group than a Wilms tumor.
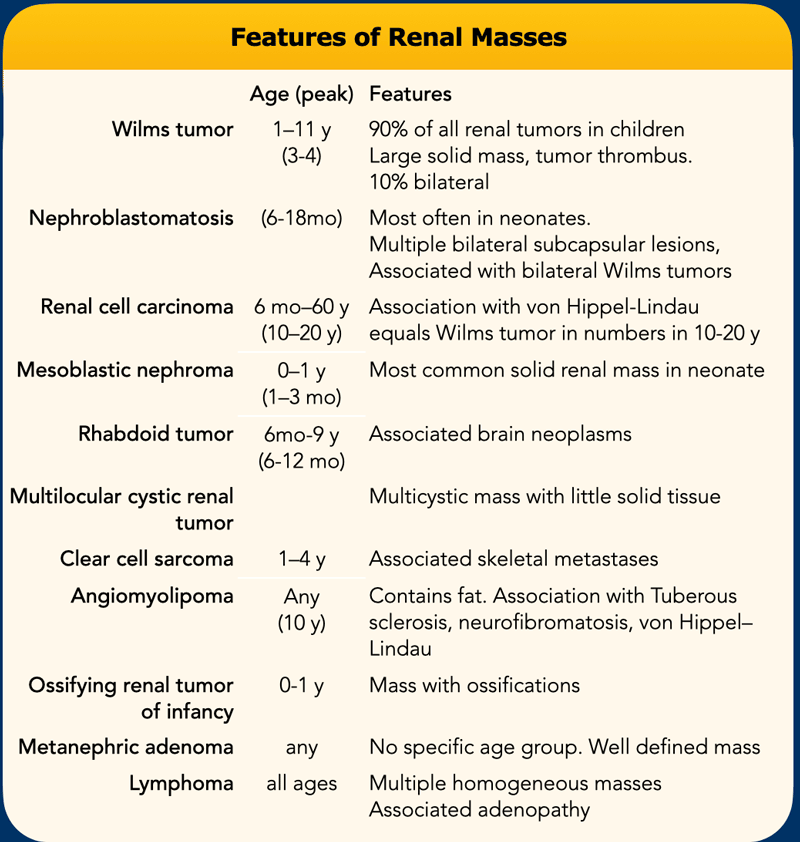
This table summarizes the features of pediatric renal tumors.
Some of these pediatric renal masses may be differentiated from a Wilms tumor on the basis of their clinical and imaging features.
- Wilms tumor is usually very large at presentation. It is the most likely diagnosis, especially when there are bilateral tumors, venous invasion, or pulmonary
metastases.
- Nephroblastomatosis occurs most often in neonates and is characterized by multiple bilateral subcapsular masses, often associated with Wilms tumors.
- Renal cell carcinoma is unusual in children except in association with von Hippel–Lindau syndrome and typically occurs in the 2nd decade.
- Congenital mesoblastic nephroma (CMN) is the most common renal tumor in the neonatal period and the most frequent benign renal tumor in childhood. A whirlpool aspect of the tumor on ultrasound
may suggest a congenital mesoblastic nephroma.
- Rhabdoid tumor is distinguished by its association with synchronous intracranial tumors.
- Multilocular cystic renal
tumors include cystic nephroma and cystic partially differentiated
nephroblastoma (CPDN). The diagnosis is suggested by a large mass constiting of
multiple cysts and no nodular solid tissue. The treatment is resection.
- Clear cell sarcoma of the kidney (CCSK) is known for its propensity to metastasize to bone, a rare location for Wilms tumor metastasis.
- Angiomyolipoma contains fat and is associated with tuberous sclerosis.
- Renal medullary carcinoma occurs in patients with sickle cell trait or hemoglobin SC disease and manifests as an infiltrative mass with metastases.
- Ossifying renal tumor of infancy (ORTI) is differentiated from mesoblastic nephroma by the presence of ossified elements. It herniates into the renal pelvis and mimics a staghorn calculus in appearance.
- Metanephric adenoma lacks specific features but is always well defined.
- Renal lymphoma is characterized by multiple homogeneous masses, often with associated lymph adenopathy.
Wilms tumor
 Nephroblastoma in a five-year-old boy.
Nephroblastoma in a five-year-old boy.
More than 90% of renal tumors in children are Wilms tumors, also called nephroblastomas. Wilms tumor presents mostly in children between 6 month and nine years of age with a peak incidence from 2 to 3 years.
Wilms tumors are generally very large at initial diagnosis and these children present with a distended abdomen.
Children with Wilms tumor are generally not ill.
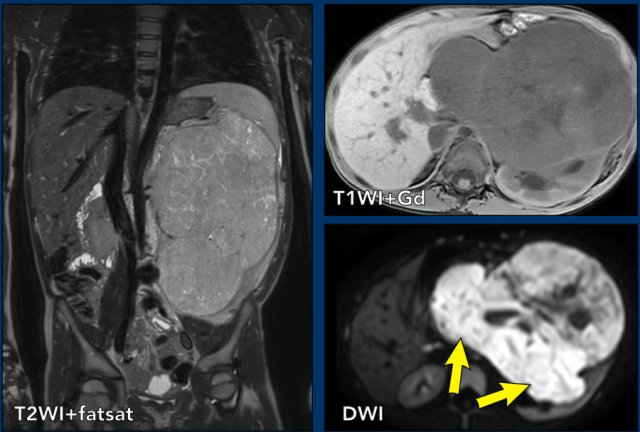
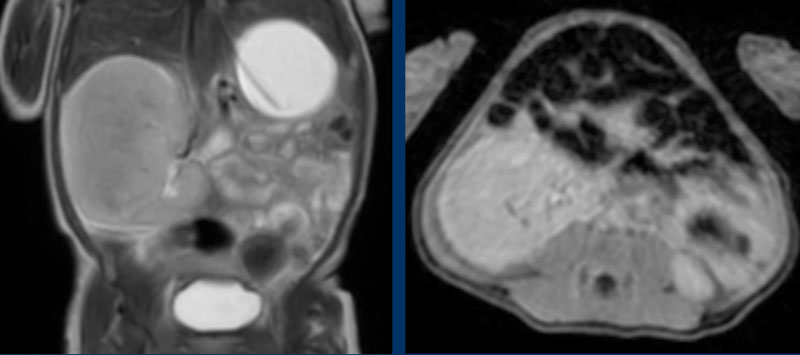
case 1
The coronal T2W-image shows an inhomogeneous tumor in the left kidney with small cystic
components.
The tumor enhances less than the peripheral remnant
of normal renal tissue.
The solid parts of the tumor show strong diffusion
restriction (arrows).
This was a Wilms tumor in a five-year-old boy. Pre-operative chemotherapy was given according to the Umbrella protocol of the SIOP-RTSG after which a nephrectomy
was performed.
Beckwith-Wiedemann syndrome
Smaller tumors can be detected when haematuria, abdominal pain, or hypertension with headache is the presenting symptom or during sonographic screening in children with syndromes which predispose to nephroblastoma, like Beckwith Wiedemann syndrome, WAGR, Perlman
syndrome, DICER 1 and Li-Fraumeni syndrome.
Bilateral nephroblastomas are often genetic or syndrome-related.
Small tumors are usually homogeneous echogenic.
Larger tumors are more inhomogeneous with cystic necrotic parts and hemorrhage.
10% of nephroblastomas have fine calcifications.
The lungs are the most frequent site of metastases.
Liver and bone metastasis are rare.
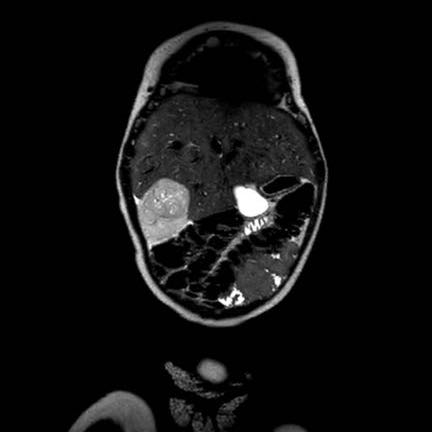
case 2
This is a two-year-old boy with Beckwith-Wiedemann syndrome.
A screening ultrasound showed a small homogeneous tumor in the left part of a horseshoe kidney.
MR findings
Wilms tumors are mostly inhomogeneous, with decreased signal intensity on T1 and increased signal intensity on T2.
Necrotic cystic parts are often present.
Enhancement after Gadolinium is inhomogeneous and less than the enhancement of normal renal parenchyma.
The solid parts of the tumor will show restricted diffusion.
Signs of hemorrhage are often present. Hemorrhagic areas will also show restricted diffusion, so look at the T1 for signs of bleeding.
MRI can nicely demonstrate tumor thrombus in the renal vein and inferior caval vein, as well as lymph node enlargement. It allows accurate and repeatable measurements of the tumor 3-dimensional, on the original and follow-up examinations.
case 3
This MRI is of a three-year-old
girl with a tumor of the right kidney.
Scroll through the coronal T2W-images.
There is a large tumor thrombus extending from the renal vein into the inferior
caval vein (arrows).
Continue with the ultrasound...
This is the initial ultrasound of the same patient showing the tumor and tumor thrombus.
case 4
This video is of a three-year-old
girl with a large mass in the right flank.
Ultrasound with a high frequency
transducer shows that the tumor originates from the right kidney.
The remnant
of the collecting system is dilated, as is often the case.
Continue with the MRI...
The MRi shows the extent of the tumor.
Notice the tumor thrombus in the inferior caval
vein.
Once you are sure of the renal origin of the tumor, scrutinize the other kidney for tumor or nephroblastomatosis (see below).
Search for enlarged para-aortal lymph nodes.
Search with color Doppler for patency of the renal vein and of the inferior caval vein, as a Wilms tumor tends to grow into the renal vein and inferior caval vein.
The finding of a liver metastasis should urge you to consider an alternative diagnosis.
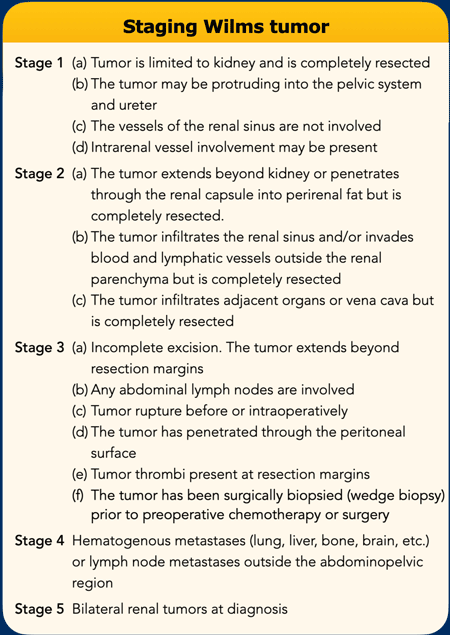
Staging and surgery
Surgery is the cornerstone for the treatment of WT.
The Children’s Oncology Group (COG) from North America recommends surgery before chemotherapy, whereas SIOP in Europe suggests preoperative chemotherapy.
As the SIOP group, the National Wilms Tumor Study Group (NWTSG) has concerns about performing a biopsy first because of the risk of tumor upstaging.
The SIOP recommends preoperative chemotherapy to decrease the risk of intraoperative rupture, downstage the tumor, and to reduce the need for irradiation.
The advantage of preoperative chemotherapy is the identification of chemoresistant high-risk blastemal predominant subtype that benefits from treatment intensification.
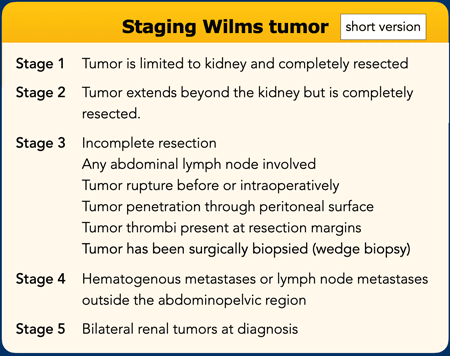
This is the short version of Wilms tumor staging.
Nephroblastomatosis
A
kidney can harbor a nephrogenic rest, which is persisting embryologic tissue.
If
multiple rests are present it is called nephroblastomatosis.
Most nephrogenic
rests resolve spontaneously, but they may transform into a Wilms tumor.
On ultrasound Wilms tumor is difficult to detect as these lesions tend to show similar echogenicity compared to the renal cortex.
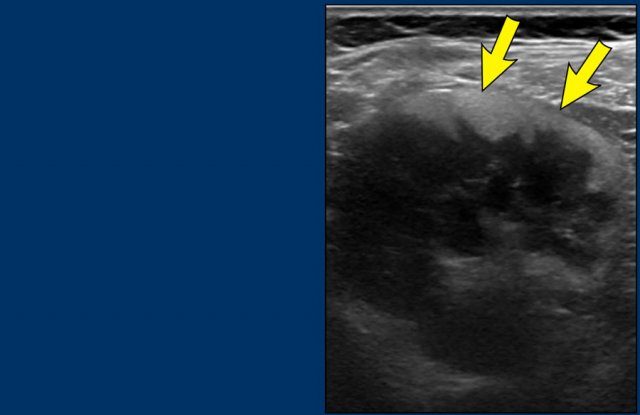
Image
Persistent
nephroblastomatosis in a seven-year-old boy who was treated five years ago for
a Wilms tumor. A peripheral rim of echogenic tissue is seen. These
residual lesions are followed up with regular ultrasound untill 5 years after
treatment.
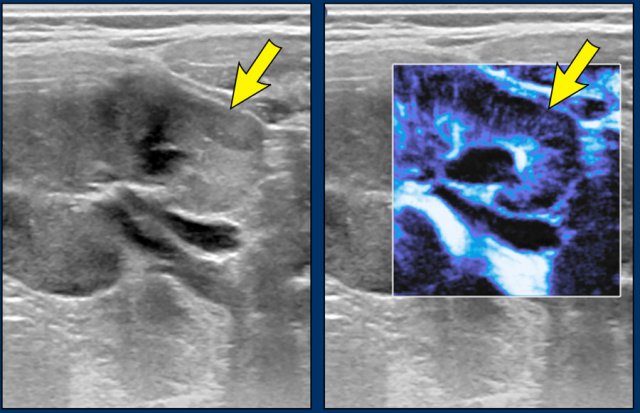
Microflow imaging can help to identify hypoperfused areas with nephroblastomatosis.
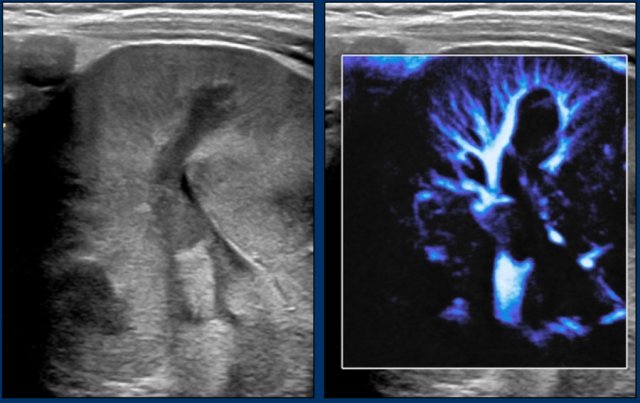
Images
A two-year-old
boy with a Wilms tumor in the left kidney and bilateral nephroblastomatosis.
With microflow color imaging it is less perfused than normal renal tissue.
Continue with the MR images...
On MRI nephroblastomatosis is best seen on the post contrast images and diffusion-weighted images.
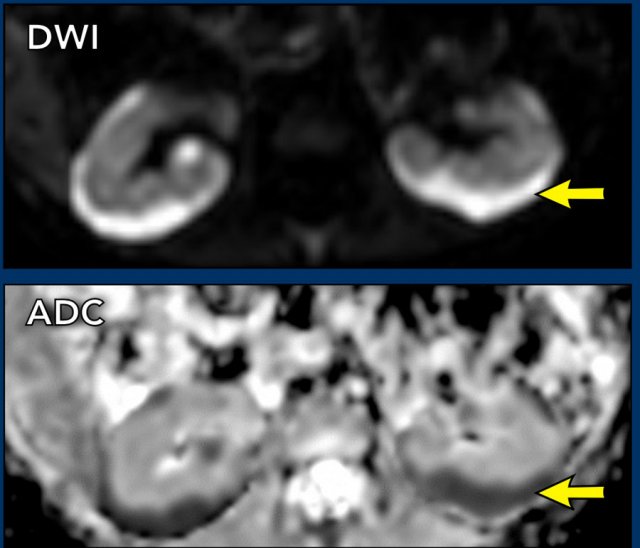
Images
MRI
images of the same patient show the hypoperfusion of the pathologic tissue and
the strong diffusion restriction with low ADC values.
Patient
was treated with pre-operative chemotherapy after which the tumor on the left
side was resected through partial nephrectomy. The diffuse
nephroblastomatosis was treated with monthly gift of AV (Actinmycin D and
Vincristin) chemotherapy for one year.
Congenital mesoblastic nephroma
Congenital mesoblastic nephroma is almost always a benign renal tumor that can be detected antenatally.
It is the most common neonatal renal tumor and most are detected before the age of one year.
The young age of the patient will strongly suggest this tumor.
On imaging there are no clear characteristics to distinguish it from a Wilms tumor, although a whirlpool aspect of the tumor on ultrasound may suggest a congenital mesoblastic nephroma.
The tumor is treated with nephrectomy.
video
In
a newborn boy the obstetrician palpated a tumor in the abdomen.
Ultrasound
showed a large mass in the upper pole of the right kidney. The video suggests a
whirled aspect of parts of the tumor.
Continue with the MRI.
MRI
The tumor has similar signal intensity as normal
renal tissue on all pulse sequences.
It enhances also equal to the remnant of the kidney.
The kidney was excised and contained a mesoblastic nephroma.
Multilocular cystic renal tumor
 Cystic nephroma
Cystic nephroma
A
multilocular cystic renal tumor is a confusing lesion.
It can be a benign cystic nephroma, or a malignant cystic partially differentiated
nephroblastoma.
Only the pathologist can make the difference.
The radiologist has to distinguish these multilocular cystic tumors which arise from the kidney with preservation of some normal renal tissue from a multicystic dysplastic kidney where no normal renal tissue is visible.
Images
Ultrasound and MRI of a four-year-old boy with a multilocular cystic lesion
in the interpolar region of the left kidney (arrow).
It was detected as an incidental
finding at the age of nine months. On follow-up no change was seen. The
lesion is consistent with a cystic nephroma, a benign condition.
The same lesion is seen on the T2 weighted transverse
image.
 Cystic nephroma
Cystic nephroma
These images are of a one-year-old girl.
On ultrasound a multicystic tumor was seen with some perfusion of
septa.
T2 weigthed image better shows the extent of the lesion. A remnant of the normal renal tissue of the lower pole is visible, distinguishing it from a multicystic dysplastic kidney.
This tumor was diagnosed as a cystic nephroma for which right nephrectomy was performed.
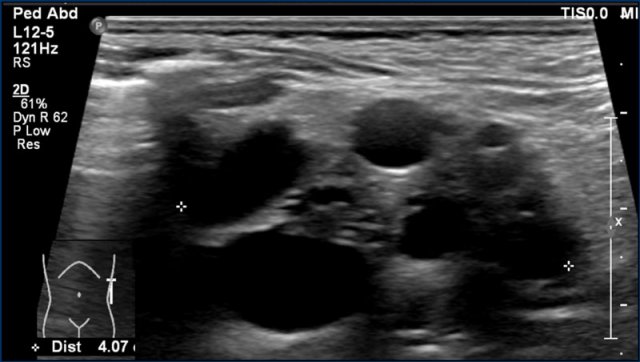
Multicystic dysplastic kidney
An 8-months-old boy with a multicystic dysplastic
kidney.
On ultrasound multiple cysts are present and no
normal renal tissue is seen.
No additional imaging is needed.
Often follow-up
ultrasound is performed to ascertain regression of the MCDK over time and to
diagnose contralateral abnormalities (in 30% of cases).
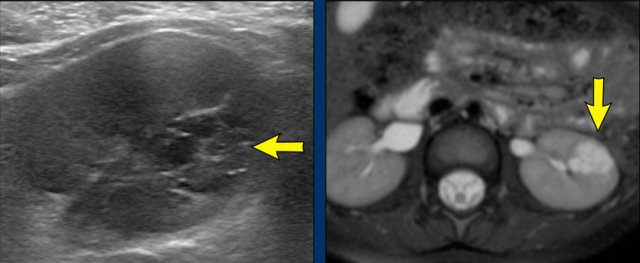
Malignant rhabdoid tumor of the kidney
 Malignant rhabdoid tumor of the kidney with brain (arrows) and bone metastases
Malignant rhabdoid tumor of the kidney with brain (arrows) and bone metastases
Malignant rhabdoid tumor of the kidney is a highly
malignant tumor with a poor
prognosis.
Distant metastases at the time of diagnosis of the tumor are
common, to the lungs, liver, brain, lymph nodes, and skeleton.
Rhabdoid renal tumors can occur in conjunction with a brain tumor, which can
be a primary atypical teratoid rhabdoid brain tumor (ATRT), but also other tumors
like medulloblastoma and ependymoma are described.
There are no distinguishing features from a Wilms tumor, but one should think of a rhabdoid tumor if the tumor is relatively small with an infiltrative growth pattern, low T2 signal and diffusion restriction.
Although rhabdoid tumors are reported to demonstrate a subcapsular fluid collection, this can occur also as an uncommon manifestation in Wilms tumor, but these collections occur in absolute numbers more in Wilms tumor than in rhabdoid tumors.
Images
Two-week-old girl presenting with a mass in the
left kidney.
A MRI of the brain at the time of initial diagnosis
showed tiny lesions, possibly metastases (arrows).
An MRI four weeks later
showed multiple brain and skull metastases.
The patient died two weeks later.
Clear cell sarcoma of the kidney
Clear
cell sarcoma of the kidney is rare, approximately 3% of pediatric renal tumors.
The 5-year survival rate is around 80% but it is worse in children below one
year of age.
The tumor has a propensity to metastasize to the bone.
The combination of a renal tumor and bone metastases should suggest to the diagnosis of a clear cell sarcoma.
The imaging findings are non-specific, but suggestive
features are that these tumors are generally homogeneous with limited diffusion
restriction.
video
A ten-month-old boy presented with an
abdominal mass. Ultrasound demonstrated a tumor in the right kidney. This is
better shown on MRI. The remnant of the kidney has a dilated collecting system.
On ADC images there is limited diffusion restriction.
Histopathology showed a clear cell sarcoma of the
kidney.
On ADC images there is limited diffusion restriction.
The tumor was thought to be a Wilms tumor, because of the limited diffusion restriction, but pathology showed a clear cell sarcoma of the kidney.
Renal cell carcinoma
Renal cell carcinoma (RCC)
is the second most common renal tumor in children.
RCC is rare in young
children and occurs mostly in children older than 10 years.
It can also occur in
patients with von Hippel-Lindau disease and Tuberous Sclerosis Complex, or
after treatment for previous malignancies (f.e Neuroblastoma or Leukemia)
Image
A nine-year-old boy presented with severe hematuria.
On palpation a left abdominal mass was found.
On ultrasound a predominantly solid mass was seen which seemed to invade the dilated collecting system.
On imaging renal cell carcinomas can present in many different ways.
They can appear more solid or have cystic elements and may be homogeneous, or rather heterogeneous.
Hemorrhage can occur and they may contain fat.
Relative small tumor size and prominent peripheral vessels suggests a RCC.
Imaging is essential for staging and a combination of ultrasound, CT and MRI is used.
video
MRI
nicely demonstrates the mass in the left kidney. Note the large collateral
veins.
Because
of heavy hematuria a left nephrectomy was performed.
Pathology showed a RCC which
was completely resected.
Lymphoma
There are two main types of lymphoma: Hodgkin lymphoma and non-Hodgkin lymphoma.
Hodgkin
lymphoma often manifests with cervical lymph node enlargement, and mediastinal
masses.
It is very rarely confined to the abdomen.
Non-Hodgkin lymphoma can be
located solely in the abdomen and generally originates from a bowel loop.
Non-Hodgkin
lymphoma presents more frequently with extra-nodal disease than Hodgkin
lymphoma.
Kidney involvement in lymphoma is rarely seen, but imaging features
to look for are multiple focal lesions that are homogeneous and hypoechoic on ultrasound and show strong diffusion restriction on MRI. 5,6
video
Ultrasound
of a three-year-old boy. Diffuse infiltration of both kidneys was seen.
Furthermore, multiple hypoechoic masses were detected
in pancreas, liver and bowel.
The combination of bowel
involvement and high LDH in de serum was highly suggestive for Burkitt
lymphoma. This diagnosis was confirmed by bone marrow biopsy and flow
cytometry.
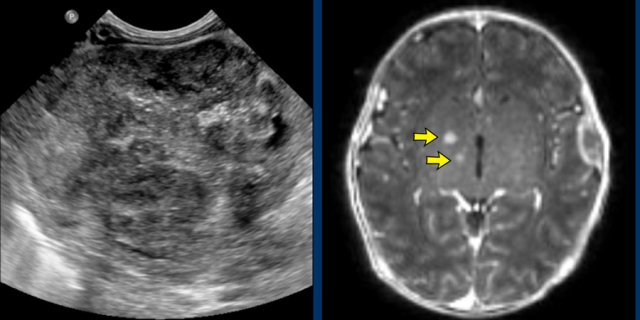
Leukemia
Leukemia is the most common malignancy in children.
It can affect all solid abdominal organs.
Organs can be diffusely infiltrated
or have a more nodular pattern.
The kidneys are affected in almost half of the
patients with acute lymphoblastic leukemia.
It can be uni- or bilateral, and
there can be focal lesions or diffuse infiltration with enlargement of the
kidneys.
The latter has a rather typical appearance with a striated pattern around the calices, similar to renal involvement of malignant lymphoma (figure).
Image
A
four-month-old boy presented with fever and anemia with thrombopenia. An
ultrasound examination shows enlarged kidneys with multiple hypo-echoic
lesions and linear abnormalities in both kidneys.
Retroperitoneal
lymphadenopathy was seen as well.
A hematological malignancy,
in particular leukemia was suspected due to the combination of imaging findings
and laboratory findings.
Continue with the video...
Distinguishing between malignant lymphoma and leukemia on imaging is difficult, when a lot of extramedullary disease is seen.
Often the final diagnosis is thus based on clinical presentation, laboratory findings (anemia and thrombocytopenia) and flow cytometry.
For this case the final diagnosis was leukemia.
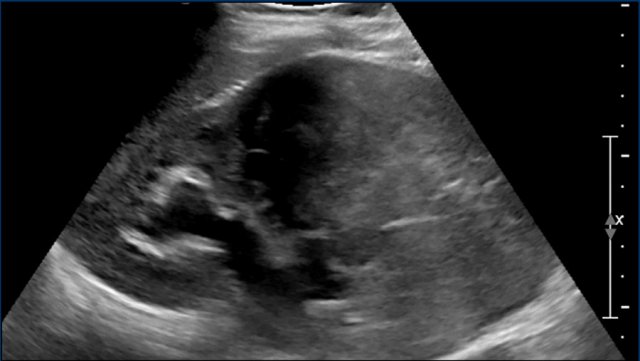
Neuroblastoma
The main differential diagnosis of nephroblastoma is neuroblastoma.
Typical
features that indicate neuroblastoma are calcifications - causing a specific
ultrasound pattern, shown in the video – and vessel encasement,
without invasion.
This vessel encasement causes the aorta and caval vein to
be lifted anteriorly.
On ultrasound the tumor is generally inhomogeneous and echogenic, with bright calcifications.
Children
with neuroblastoma are generally very ill, while children with a Wilms tumor are not.
The Vanillyl Mandelic Acid (VMA) and HomoVanillic Acid
(HVA) levels in the urine are in most cases elevated.
In our hospital these levels are checked in every child that presents with a tumor in the abdomen.
video
Three-years-old
girl referred from a peripheral hospital with a diagnosis of a tumor of the
left kidney. Ultrasound shows a mass originating from the left kidney. The mass
is very inhomogeneous with calcifications, and much more compatible with a
neuroblastoma than a nephroblastoma.