Normal Values in Pediatric Ultrasound
Simon Robben, Rick van Rijn and Robin Smithuis
Radiology Departement of the Maastricht University Hospital, Academical Medical Centre in Amsterdam and the Alrijne hospital in Leiden, the Netherlands
Publicationdate
This document provides an overview of normal reference values for ultrasound examinations in neonates and children.
The items are in an alphabethic order.
Select one of the items listed on the left for details.
Adrenal
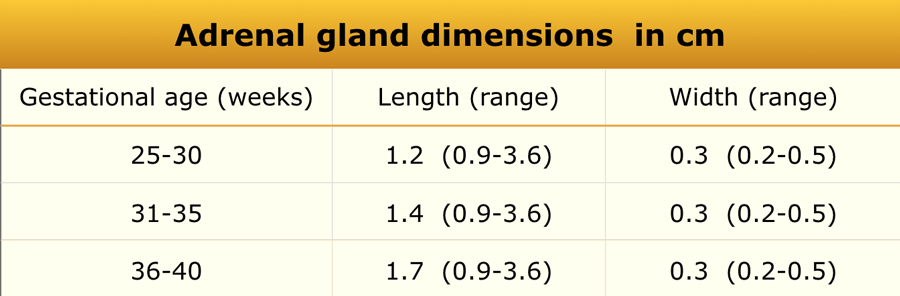 Adapted from reference 21
Adapted from reference 21
Materials and Methods
An ultrasonographic study was performed in 92 infants.
Measurements
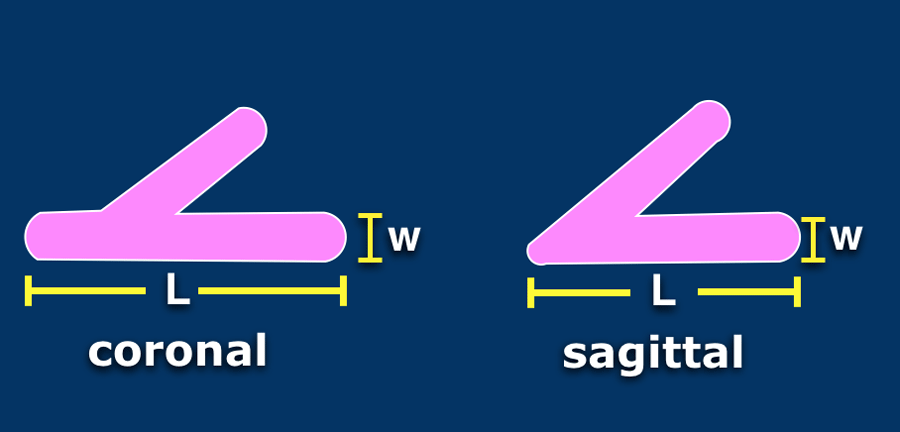
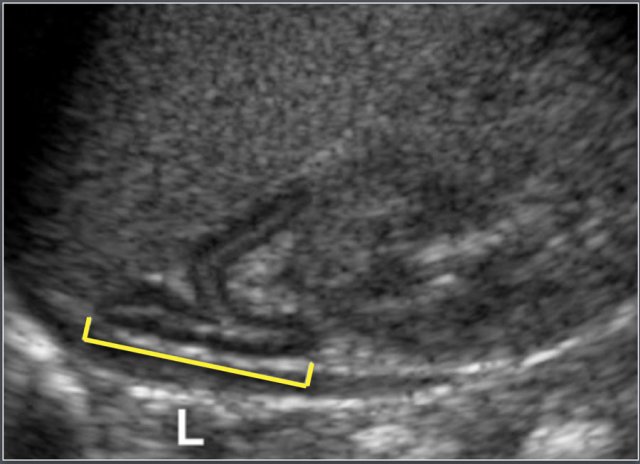
- Length (L): Defined as the maximum cephalocaudal dimension of the adrenal gland, measured in either the coronal or sagittal plane.
- Width (w): Defined as the maximum thickness of one of the limbs.
Causes of Adrenal Enlargement
- Congenital adrenal hyperplasia
- Adrenal hemorrhage
- Adrenal neuroblastoma
Appendix
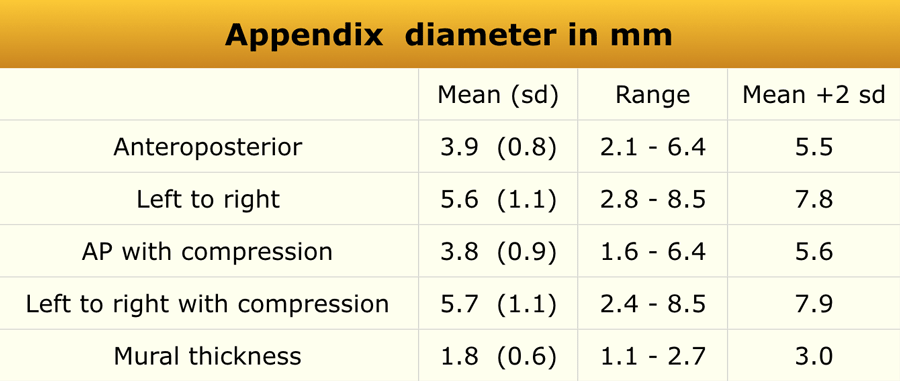 Adapted from reference 14
Adapted from reference 14
Materials and Methods
An ultrasonographic study was conducted in 146 consecutive patients (62 boys and 84 girls; mean age, 7 years; age range, 2–15 years).
Exclusion criteria
- Cystic fibrosis
- Acute abdominal pain
- Previous appendectomy
- Age <2 years (due to difficulty in performing the examination)
The appendix was successfully visualized in 120 children.
Causes of Appendiceal Enlargement
- Acute appendicitis
- Cystic fibrosis
- Lymphoid hypertrophy (due to immune deficiency or viral enteritis)
- Intraluminal gas, mucus, or fecal material
- Mucocele
Bladder
 Adapted from reference 17
Adapted from reference 17
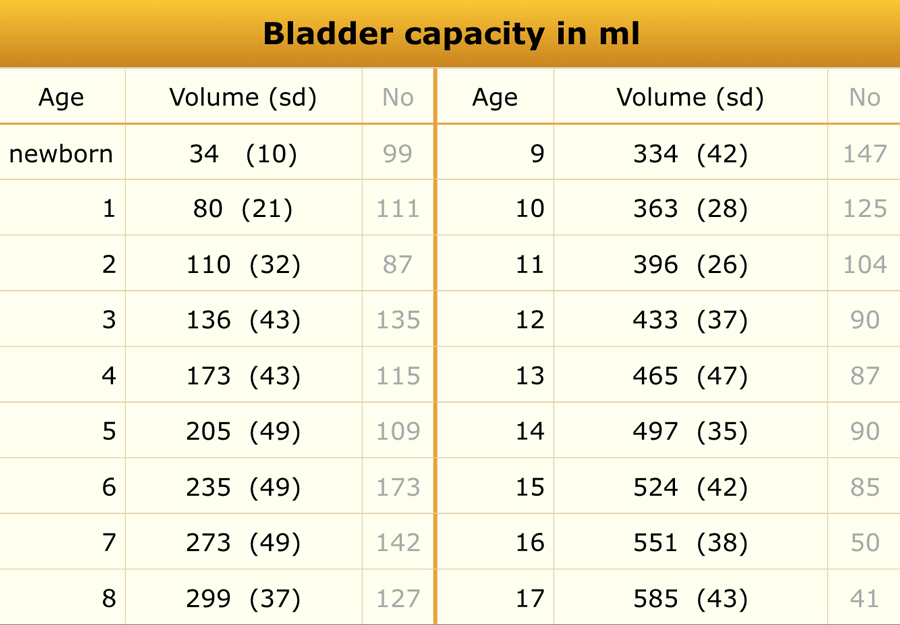
Bladder volume
Materials and Methods
A total of 3,376 children were included in this ultrasonographic study.
Note: The total number of patients listed in the results tables may differ, as not all age subgroups were represented.
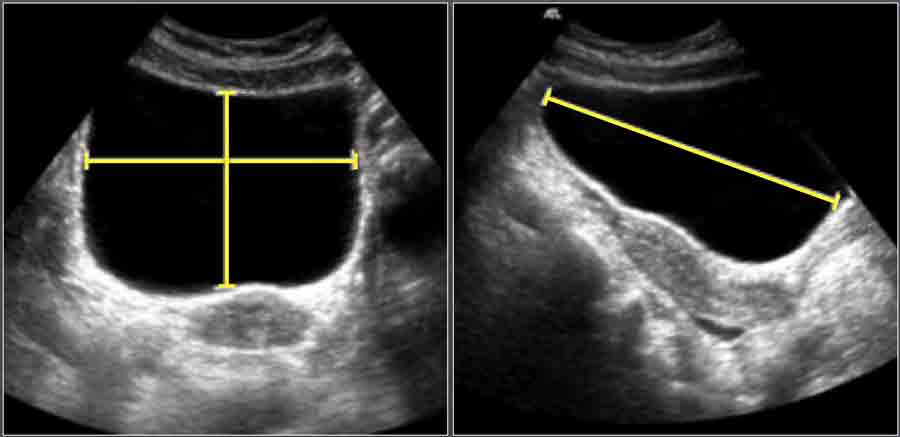
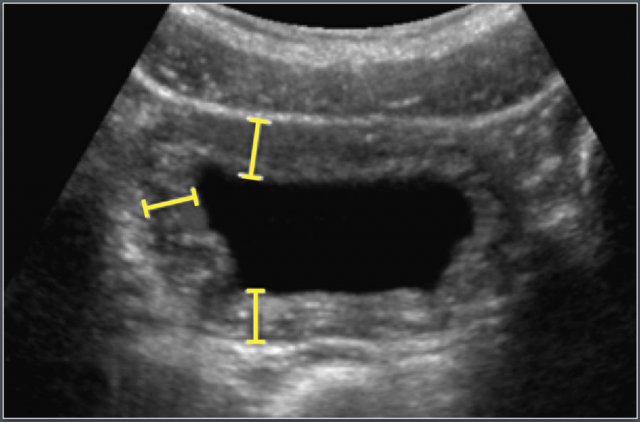
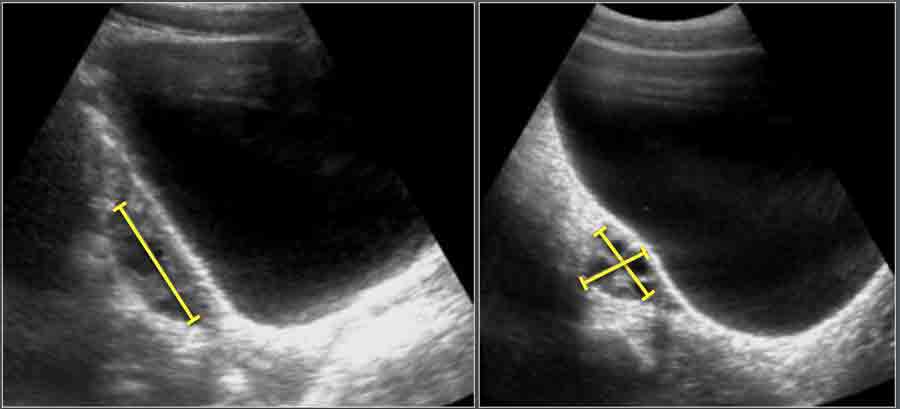
Measurement Technique
- Length (L): Measured on a longitudinal scan from the bladder neck to the fundus.
- Depth (D): Measured perpendicular to the longitudinal plane at the level of maximum cross-sectional area, from the anterior to posterior mucosal surface in the midline.
- Width (W): Measured perpendicular to D at its midpoint.
Bladder Volume Calculation
Bladder volume was calculated using the ellipsoid formula:
Volume (cm³)=L×D×W×0.523Volume (cm³)=L×D×W×0.523
 Adapted from reference 17
Adapted from reference 17
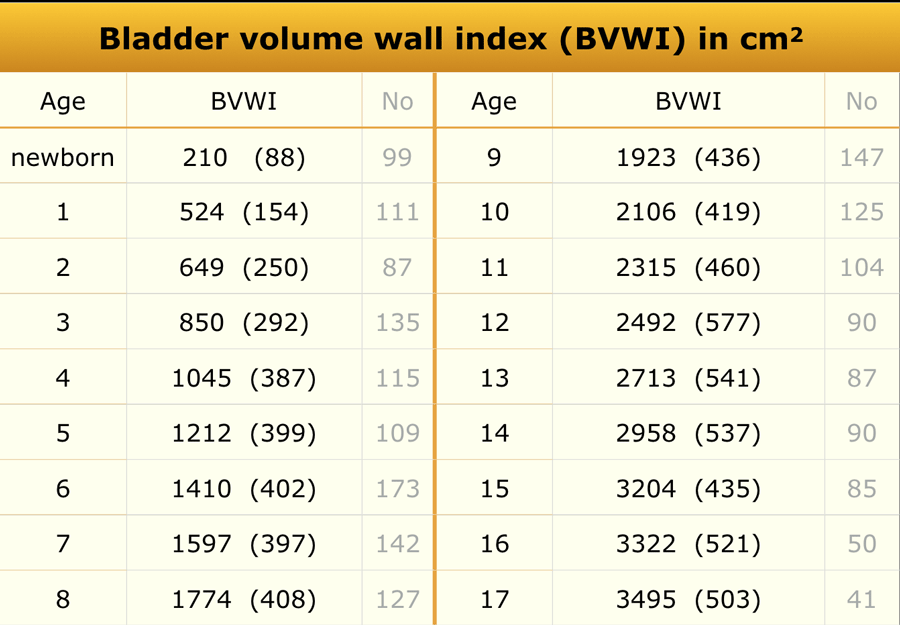
Bladder wall thickness
Materials and Methods
A total of 3,376 children were included.
Bladder wall thickness was measured only when the residual bladder volume was <10% of the pre-voided volume.
Measurement Technique
The bladder wall was evaluated on a zoomed transverse image of the emptied bladder.
Measurements were taken at three sites:
- Anterolateral
- Lateral
- Posterolateral
The mean of these three measurements was used for analysis.
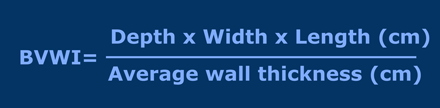
Bladder Volume Wall Thickness Index (BVWTI)
Bladder wall thickness depends on the degree of bladder filling and bladder capacity.
Therefore, it is expressed as the Bladder Volume Wall Thickness Index (BVWI).
It helps normalize bladder wall measurements across different degrees of bladder distension and improves diagnostic accuracy for lower urinary tract abnormalities, especially in children.
Causes of Bladder Wall Thickening
- Cystitis
- Dysfunctional voiding
- Posterior urethral valves
Bowel
 Adapted from reference 13
Adapted from reference 13
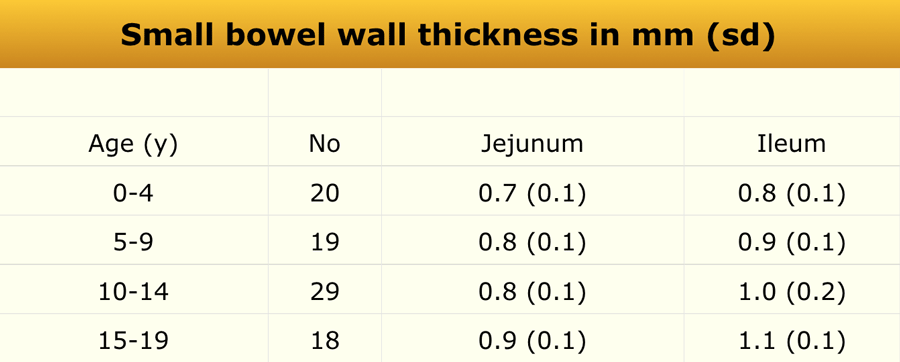
Materials and Methods
The study population consisted of 128 patients (57 males and 71 females). Of these, 86 individuals were aged between 1 and 19 years (only data pertaining to this subgroup are presented).
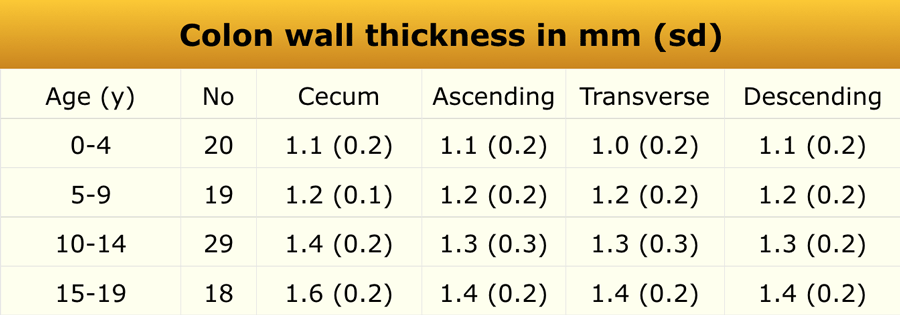
Bowel wall thickness was measured on transverse ultrasound sections and included the following histologic layers: mucosa, lamina propria, muscularis mucosae, submucosa, and muscularis propria.
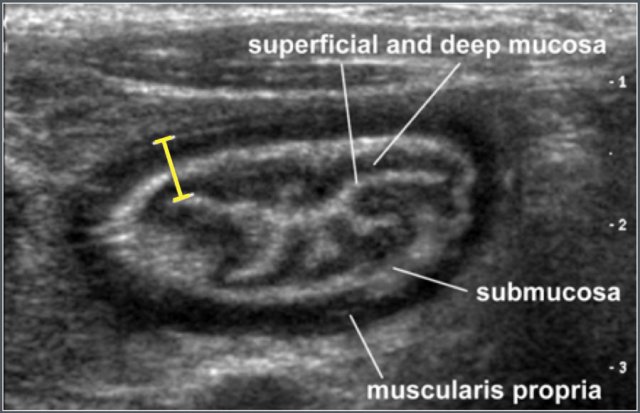
Ultrasonographic example
Measurement of the terminal ileum wall thickness in a 12-year-old male patient with cystic fibrosis.
Common causes of small bowel wall thickening include:
- Henoch–Schönlein purpura
- Crohn’s disease
- Lymphoma
 Adapted from reference 13
Adapted from reference 13
In the same study, colonic wall thickness was also measured.
Common causes of colonic wall thickening include:
- Inflammatory bowel disease (IBD)
- Hemolytic–uremic syndrome (HUS)
- Pseudomembranous colitis
Common Bile Duct
 Adapted from reference 8
Adapted from reference 8
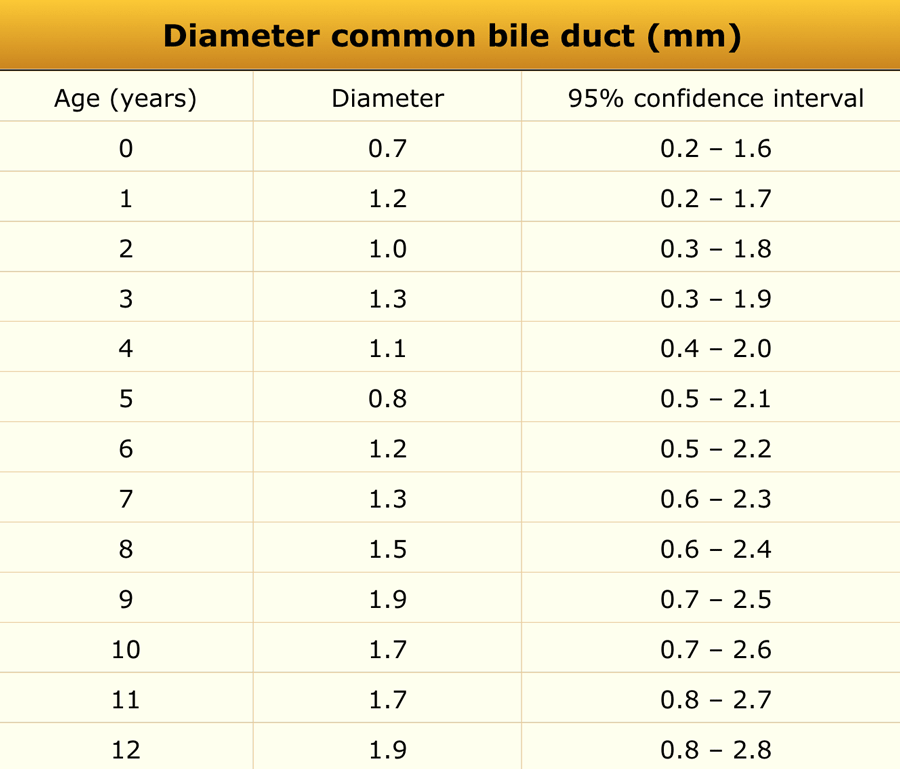
Materials and Methods
A total of 173 consecutive pediatric patients (100 boys and 73 girls) referred for abdominal ultrasonography unrelated to hepatobiliary pathology were included. The age range was 1 day to 13 years (median 5.0 years).
In all subjects, the diameter of the common bile duct measured ≤ 3.3 mm.
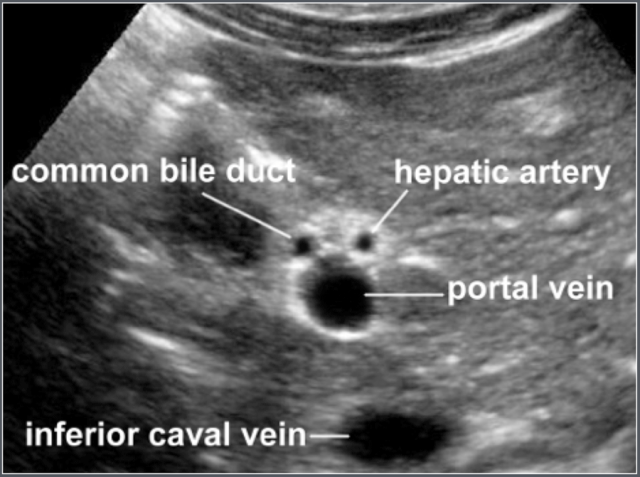
Image
Transverse ultrasonographic image of the common bile duct and surrounding anatomy.
Galbladder
 Adapted from reference 10
Adapted from reference 10
Materials and Methods
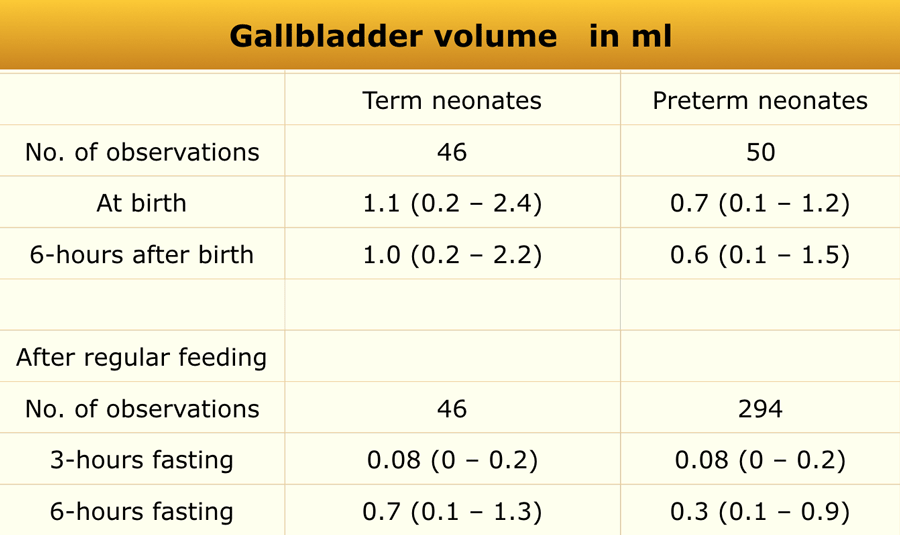
Ultrasonographic gallbladder volume was calculated using the ellipsoid formula:
Volume = length × width × height × 0.52
The study included 50 preterm infants (mean gestational age 31.7 ± 2.5 weeks, mean birth weight 1556 ± 441 g) and 46 term infants (mean gestational age 38.3 ± 1.2 weeks, mean birth weight 3253 ± 440 g).
Measurements were obtained shortly after birth, following 6 hours of fasting, and again at 5–7 days of age after 3-hour and 6-hour fasting intervals following regular milk feeding.
Common causes of a small gallbladder include:
- Biliary atresia
- Postprandial (after fatty meal) contraction
Hip
 Adapted from reference 22
Adapted from reference 22
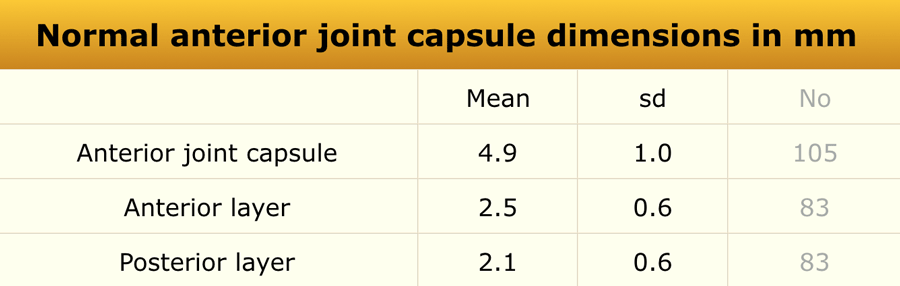
Anterior recess
Materials and Methods
An ultrasonographic study was performed in 58 healthy children and 105 children with unilateral transient synovitis, aged 1.7–12.8 years.
 Adapted from reference 22
Adapted from reference 22
All examinations were performed with the patient in the supine position and the hips in a neutral position.
The anterior joint capsule was measured, including both its anterior and posterior layers. The anterior contour of the joint capsule was also evaluated.
No statistically significant correlation was found between age and anterior joint capsule thickness.
A difference greater than 2 mm between sides or an effusion >2 mm was considered abnormal.
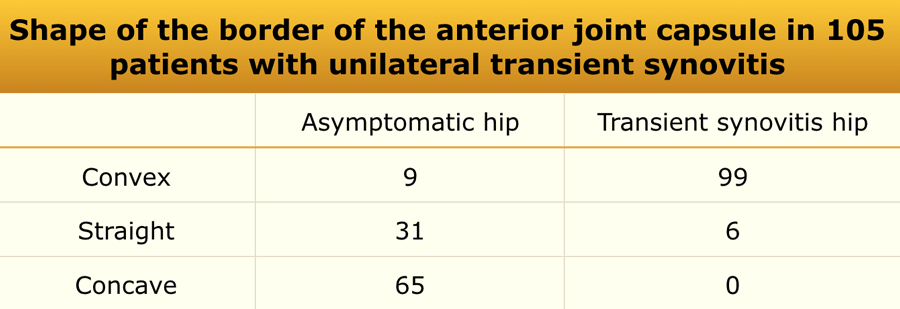
Shape of the border of the anterior joint capsule
The anterior contour of the joint capsule can be evaluated.
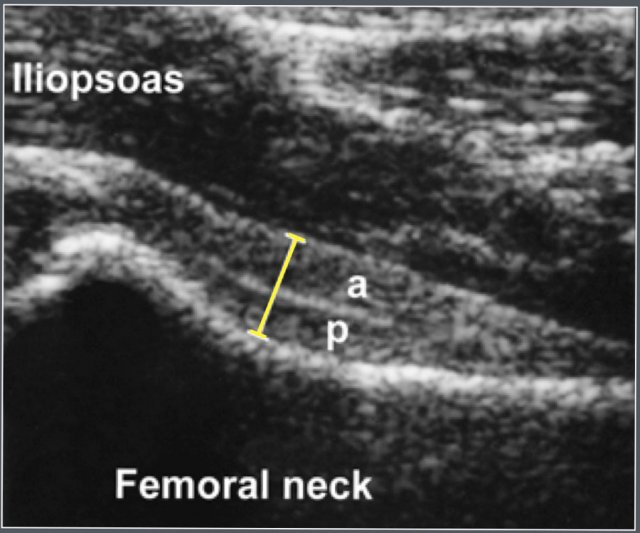
Ultrasonographic measurement of the anterior joint capsule.
Both anterior (a) and posterior (p) layer can be identified.
Common causes of hip joint effusion include:
- Transient synovitis
- Septic arthritis
- Juvenile idiopathic arthritis (JIA)
 Adapted from reference 23
Adapted from reference 23
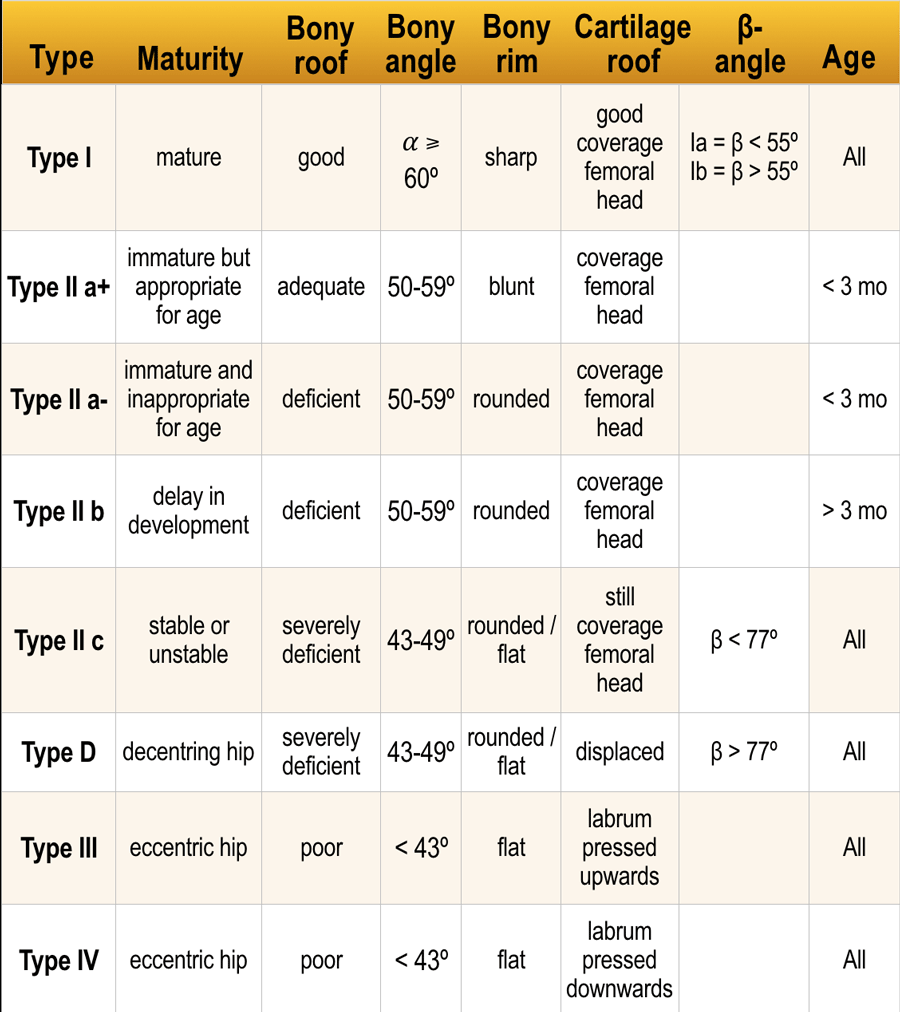
Developmental Dysplasia of the Hip (Graf’s Classification)
- Type I: Mature, centered hip joint with a well-developed acetabular roof and an angular or slightly blunt bony rim.
- Type II: Centered hip joint with a deficiently developed acetabular roof and a rounded bony rim.
- Type III: Decentered hip joint with a poorly developed acetabular roof and a flattened bony rim.
Click here for article on Developmental Dysplasia of the Hip.
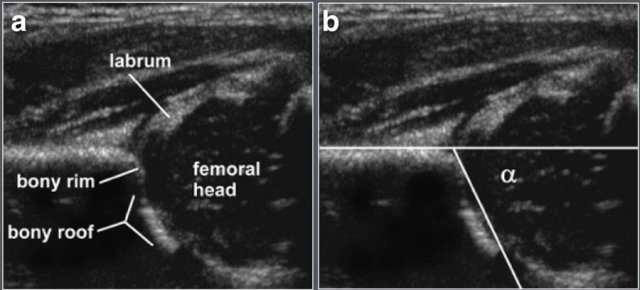
Ultrasonographic parameters:
- Coronal plane view of the hip joint
- Measurement of the α (alpha) angle
Kidney
 Adapted from reference 6
Adapted from reference 6
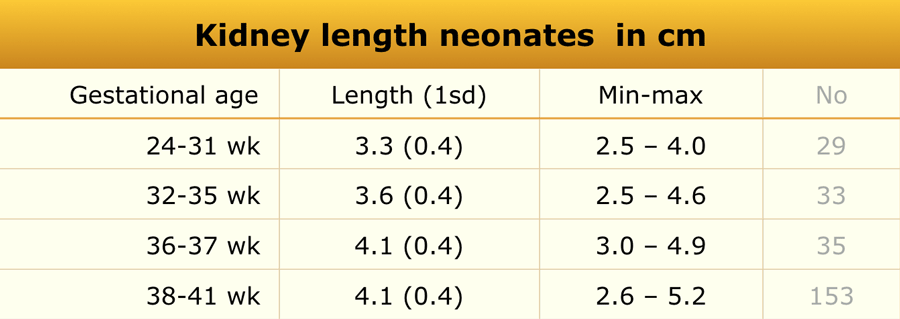
Preterm and Term Babies
Materials and Methods
Ultrasonographic evaluation was performed in 261 healthy newborn infants.
The craniocaudal dimension of each kidney was measured using standard ultrasonography.
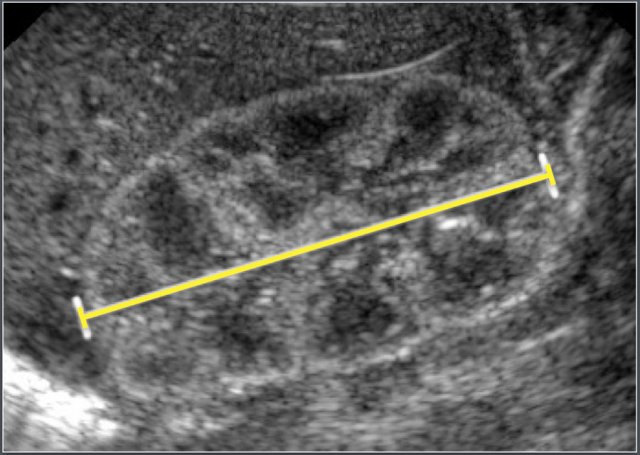
Ultrasonographic measurement of the length of a neonatal kidney.
In neonates, the renal parenchyma is typically more echogenic than the liver parenchyma, which is a normal finding at this age.
 Adapted from reference 16
Adapted from reference 16
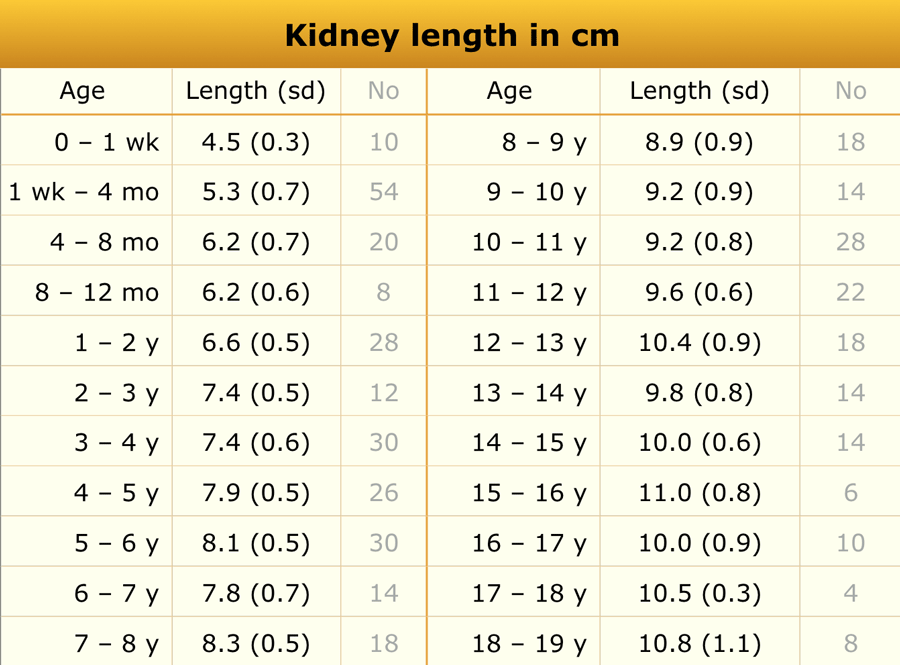
Children
Materials and Methods
The study included 203 pediatric patients. Exclusion criteria included a history of malignancy, steroid use, upper urinary tract abnormalities, vesicoureteral reflux (VUR) greater than grade I, urologic surgery, or abnormal renal sonographic findings.
On average, the left kidney measured 1.9 mm longer than the right.
Common causes of renal enlargement include:
- Duplicated collecting system
- Nephritis (infectious and non-infectious)
- Leukemia or lymphoma
- Autosomal recessive polycystic kidney disease (ARPKD)
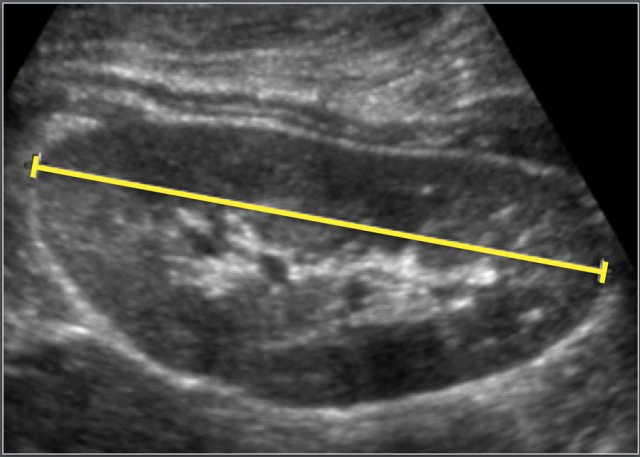
Ultrasonographic measurement of the length of a kidney.
 Adapted from reference 17
Adapted from reference 17
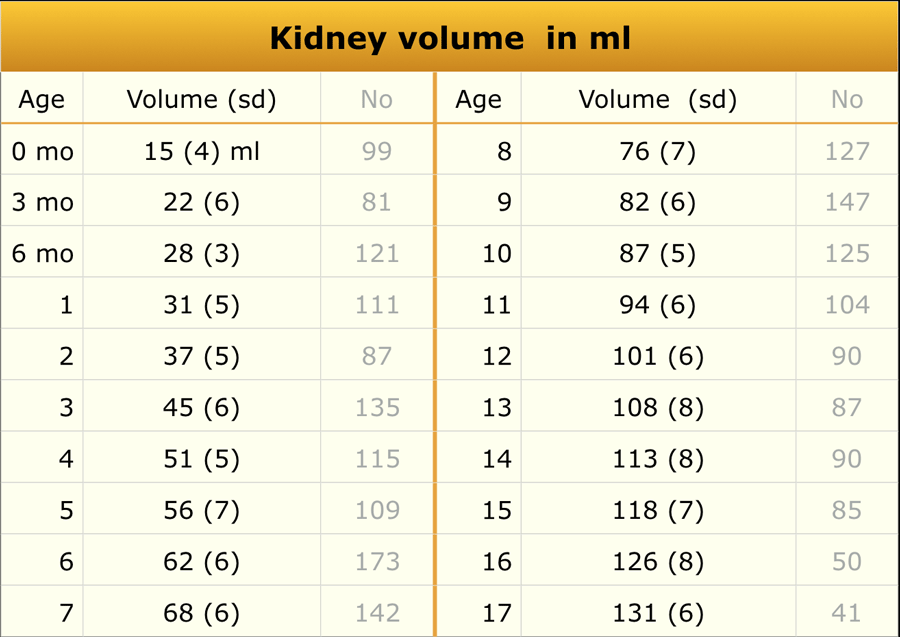
Renal volume
Materials and Methods
A total of 3,376 children were included in this ultrasonographic study.
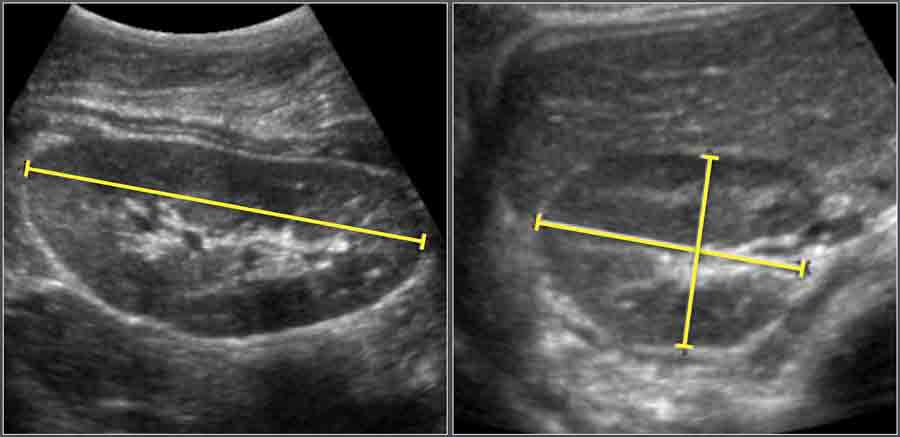
Renal volume was calculated using the ellipsoid formula:
Volume = Length × Width × Depth × 0.523
The total renal volume was determined by summing the right and left kidney volumes.
The reported values represent the average of both kidneys.
 Adapted from reference 18
Adapted from reference 18
Thickness of the wall of the collecting system
Materials and Methods
Ultrasonographic examination of 48 renal collecting systems in 24 healthy children (aged 3 days–12.6 years) was performed.
The wall of the collecting system was identifiable in all kidneys, ranging from 0 (not visible) to 0.8 mm in thickness.
A wall thickness ≥ 1 mm was considered abnormal.
Common causes of collecting system wall thickening include:
- Urinary tract infection (UTI)
- Intermittent dilatation (e.g., vesicoureteral reflux)
- Recent or resolved dilatation
Liver
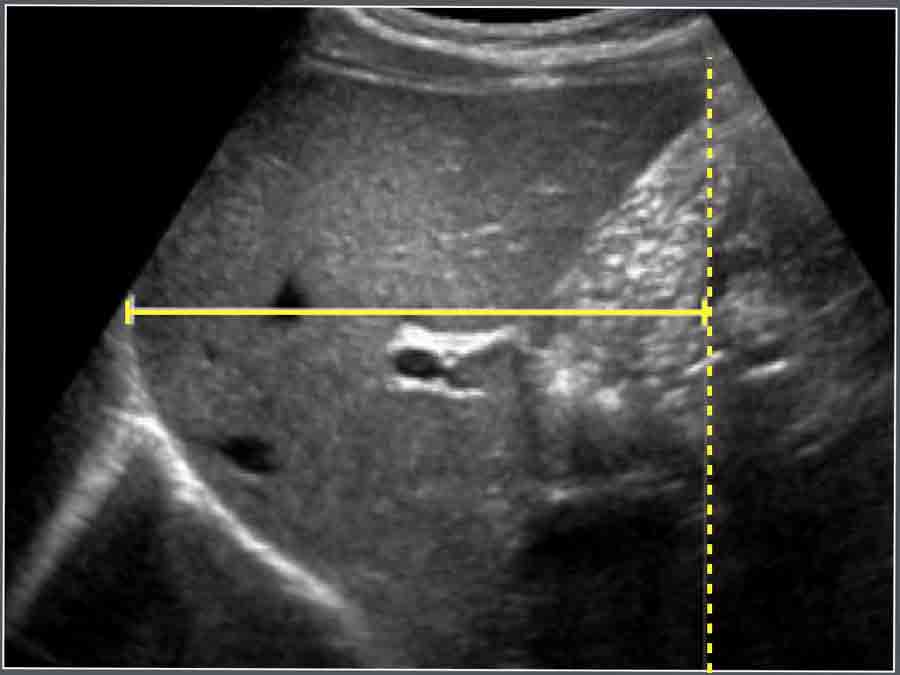
The craniocaudal dimension of the liver is measured along the midclavicular line using ultrasonography.
Causes of hepatomegaly include:
- Leukemia
- Storage diseases (e.g., glycogen storage disorders)
- Neonatal hepatitis
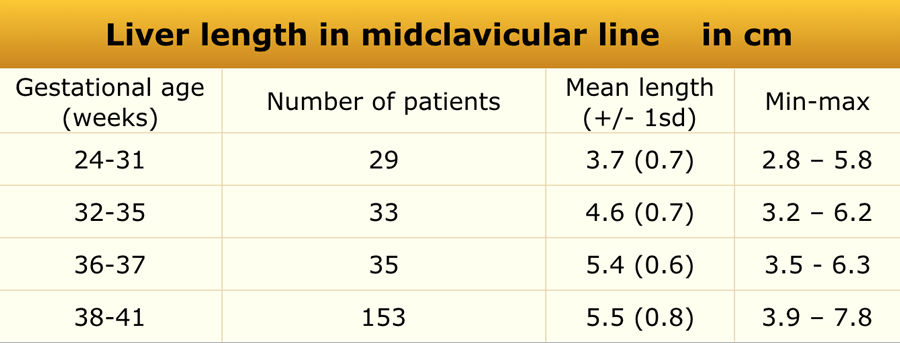 Adapted from reference 6
Adapted from reference 6
Newborns
Materials and Methods
In newborns (n = 261), the craniocaudal dimension of the liver was measured along the midclavicular line using ultrasonography.
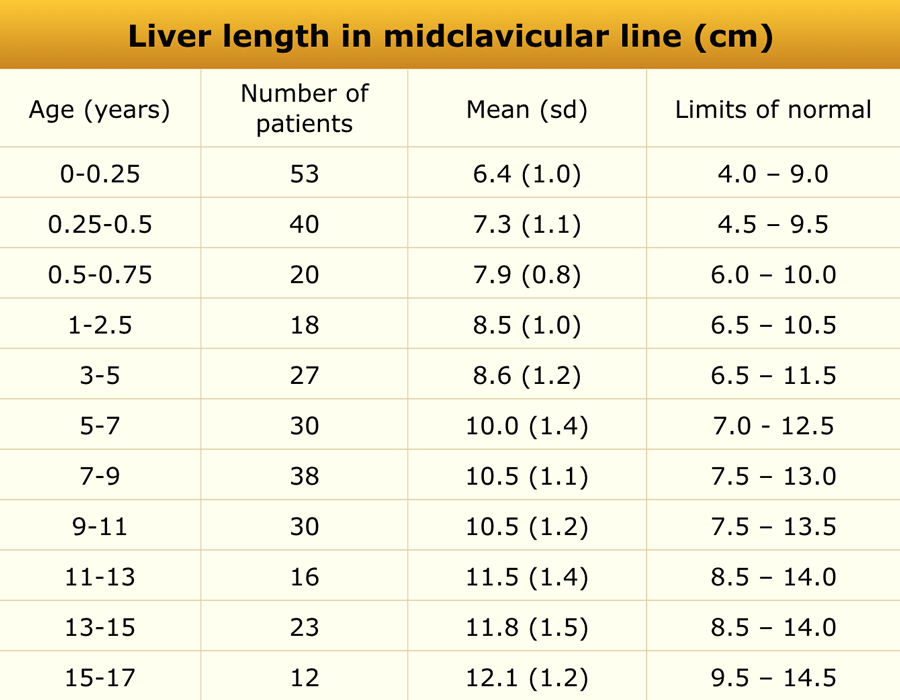 Adapted from reference 7
Adapted from reference 7
Children
Material and methods
US study in 307 healthy children.
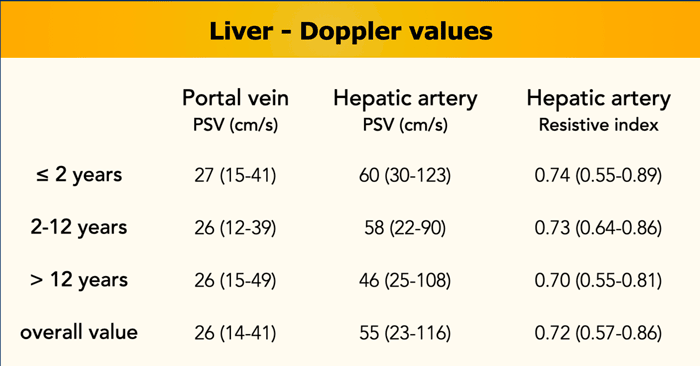
Doppler parameters
Materials and Method
An additional study of 100 healthy children (age range 0–17.9 years, median 7.8 years) established reference values for:
- Portal vein peak systolic velocity
- Hepatic artery peak systolic velocity
- Hepatic artery resistive index (RI)
(reference).
Findings:
- Portal vein velocity was not age-independent
- Hepatic artery velocity and RI decreased with increasing age
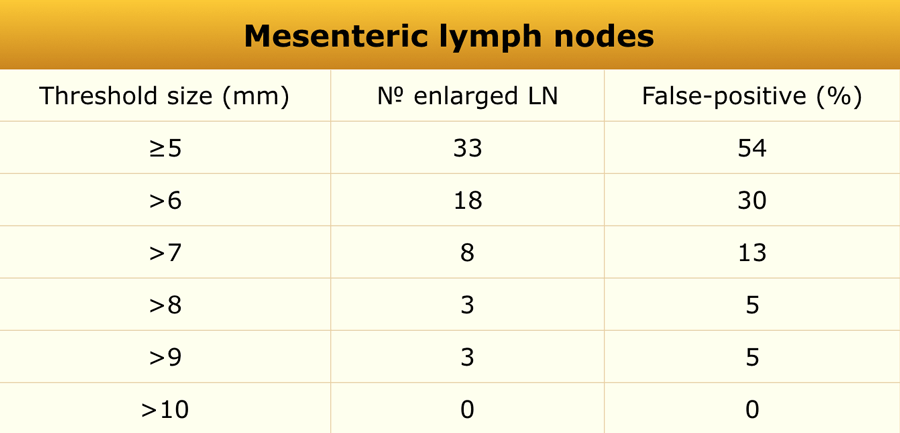
Mesenteric lymph nodes
 Adapted from reference 15
Adapted from reference 15
Materials and Methods
This retrospective study included 61 children (36 boys, 25 girls; mean age 10.7 years, range 1.1–17.3 years) who underwent non-contrast abdominal CT for evaluation of suspected or confirmed renal stones. Lymph node size was evaluated on these images, and findings were extrapolated to ultrasonographic reference values.
Findings:
Enlarged mesenteric lymph nodes (short-axis diameter > 5 mm) were observed in 33 of 61 children (54%), predominantly in the right lower quadrant (88%).
Based on these results, a short-axis diameter > 8 mm may represent a more accurate threshold for pediatric mesenteric lymphadenopathy.
False-positive rate for enlarged mesenteric lymph nodes with varying lymph node threshold size is seen in the table.
Common pathological causes of enlarged mesenteric lymph nodes include
- Intestinal lymphoma
- Lymphogenic metastasis
- Specific infectious enteritis (e.g., tuberculosis)
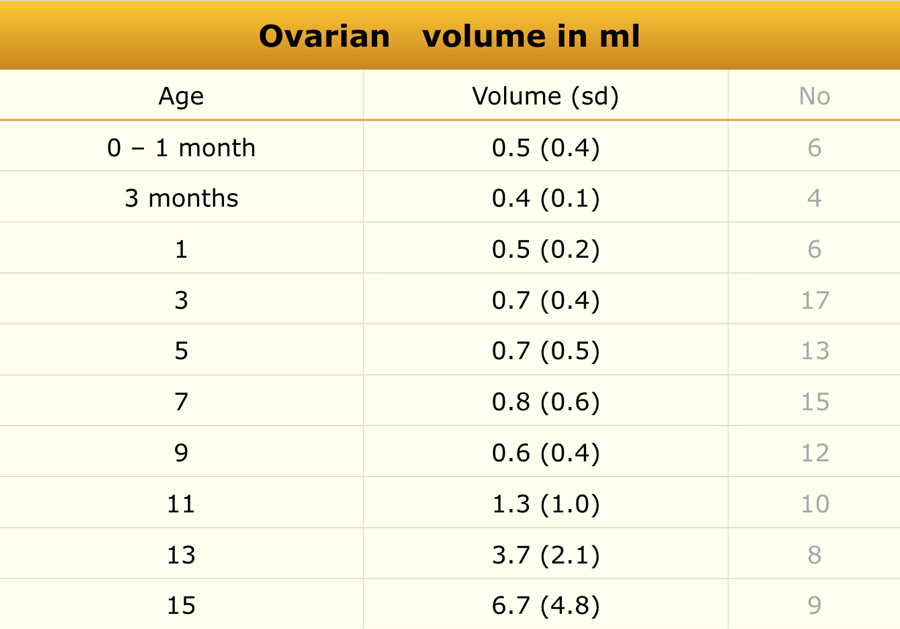
Ovary
 Adapted from reference 20
Adapted from reference 20
Materials and Methods
Ultrasonographic measurements of uterine and ovarian volumes were performed in 178 healthy girls.
Common causes of ovarian enlargement include:
- Precocious puberty
- Ovarian torsion
- Polycystic ovarian disease
- Teratoma or dermoid cyst
Ovarian volume is calculated using the formula:
- Length x Width x Height x 0.523.
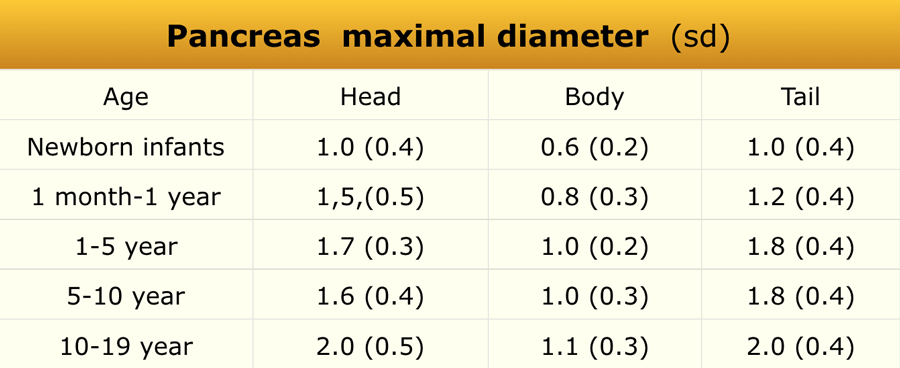
Pancreas
 Adapted from reference 12
Adapted from reference 12
Materials and Methods
This retrospective ultrasonographic study included 273 pediatric patients (sex distribution not specified).
Echogenicity findings:
- Low echogenicity in 27 cases (10%)
- Isoechoic in 145 cases (53%)
- Increased echogenicity in 101 cases (37%)
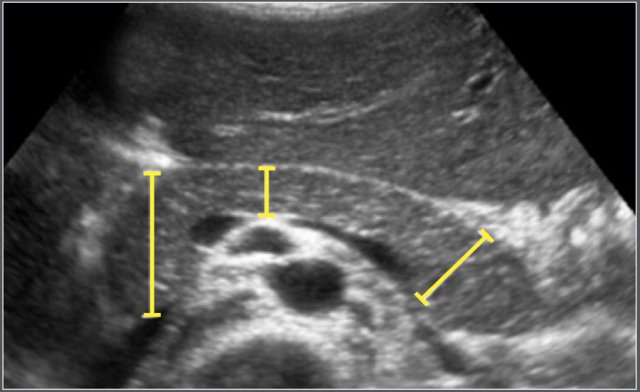
The maximum anteroposterior (AP) diameters of the head, body, and tail of the pancreas were measured on transverse or oblique ultrasound images.
Common causes of pancreatic enlargement include:
- Traumatic pancreatitis
- Viral pancreatitis
- Drug-induced pancreatitis
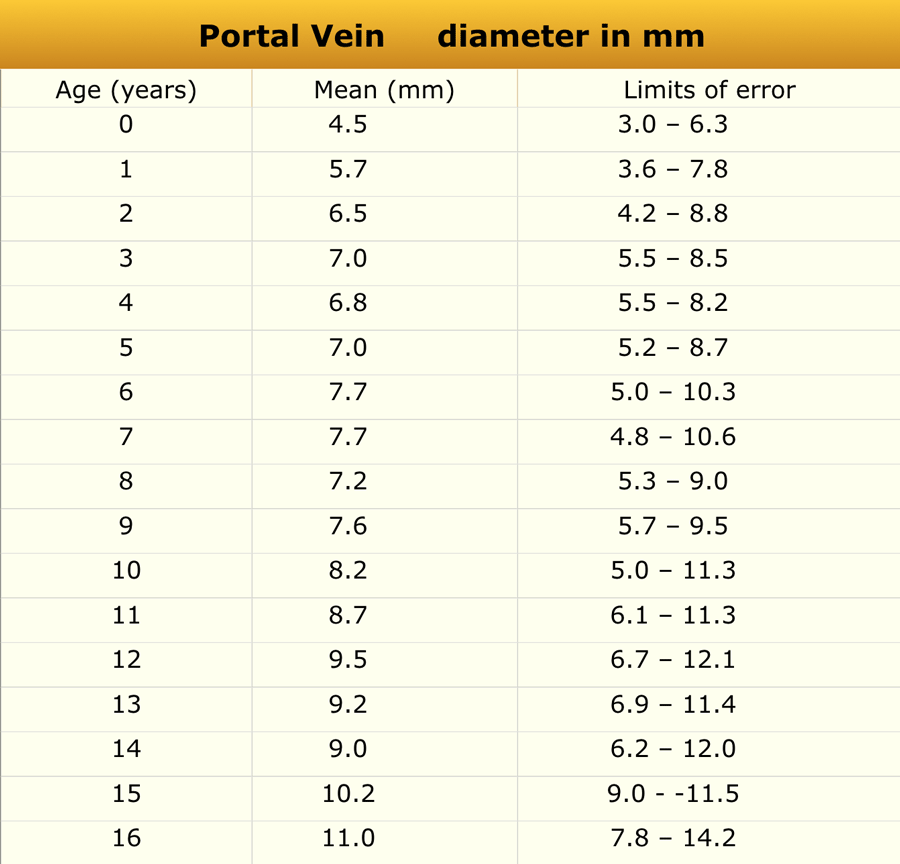
Portal vein
 Adapted from reference 9
Adapted from reference 9
Materials and Methods
A study was conducted in 150 children aged 0–16 years without clinical evidence of hepatic or intestinal disease who underwent abdominal ultrasonography.
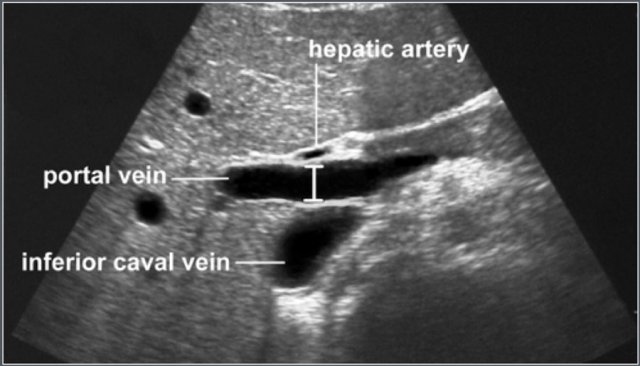 Measurement of portal vein diameter
Measurement of portal vein diameter
The portal vein was visualized in the longitudinal plane from the splenomesenteric junction to the hepatic hilum.
The maximum anteroposterior diameter was measured at the point where the hepatic artery crosses the portal vein.
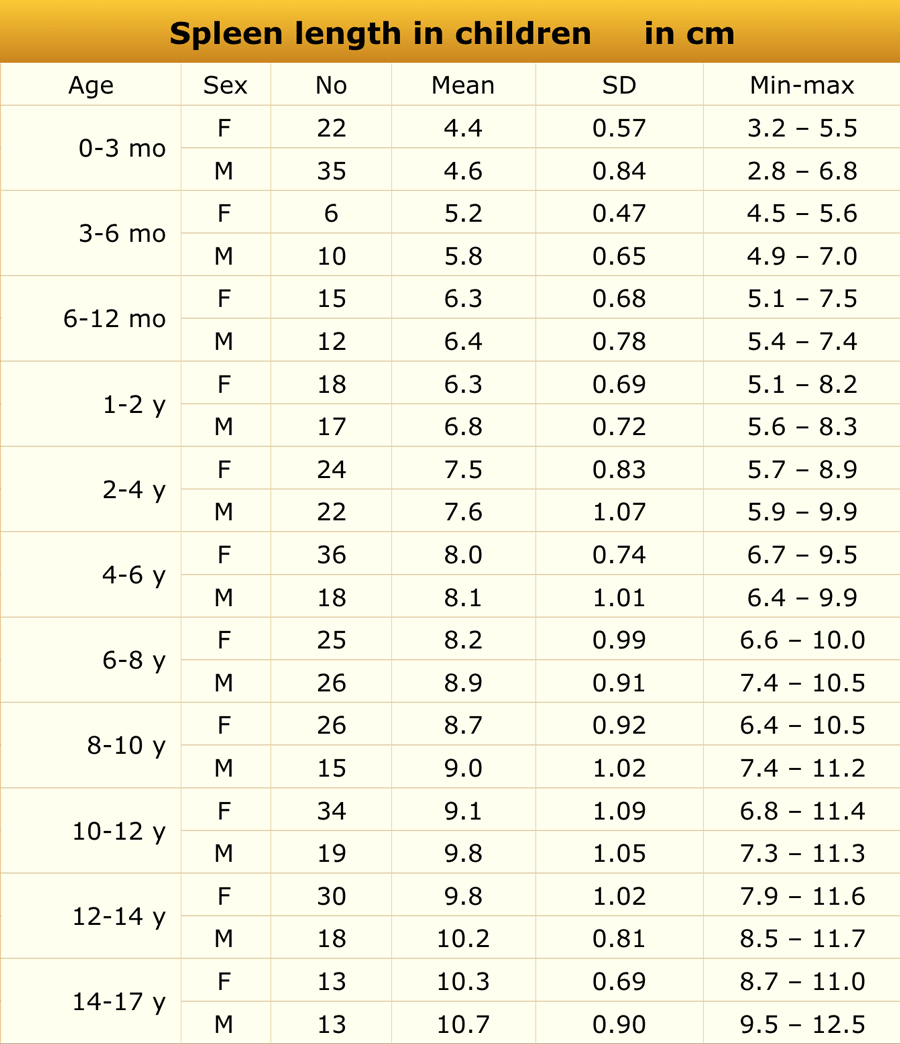
Spleen
 Adapted from reference 6
Adapted from reference 6
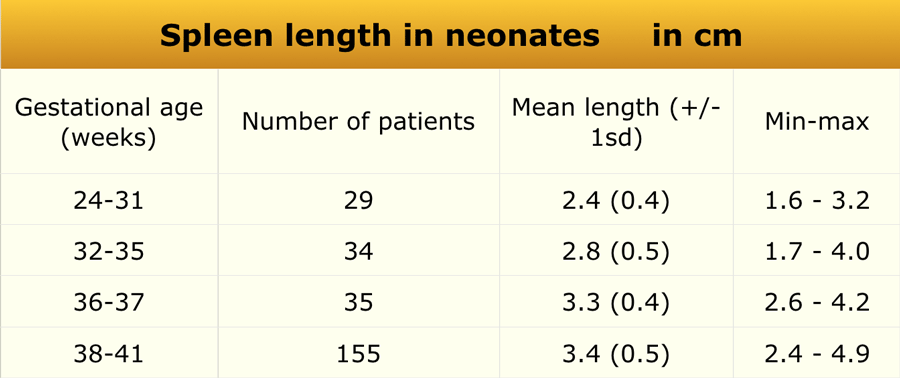
Preterm and term babies
Material and methods
US study in 261 healthy newborn infants.
Craniocaudal dimension of the spleen was determined with ultrasonography.
 Adapted from reference 11
Adapted from reference 11
Children
Materials and Methods
Ultrasonographic examination included 512 healthy children (238 boys, 274 girls; age range 1 day to 17 years) and 96 preterm infants (gestational age 25–35 weeks).
None of the subjects had medical conditions affecting spleen size.
Common causes of splenomegaly include:
- Portal hypertension
- Leukemia
- Systemic infections (e.g., Epstein–Barr virus, cytomegalovirus)
- Hematologic disorders (e.g., spherocytosis, thalassemia)
- Storage diseases
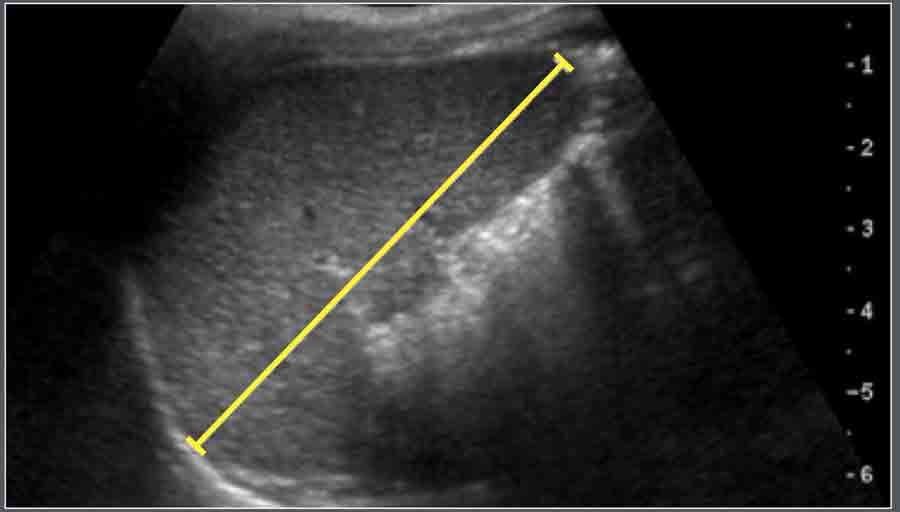
Measurement
Spleen length was defined as the maximal distance between the most superomedial and inferolateral points on a longitudinal coronal view, ideally through the splenic hilum.
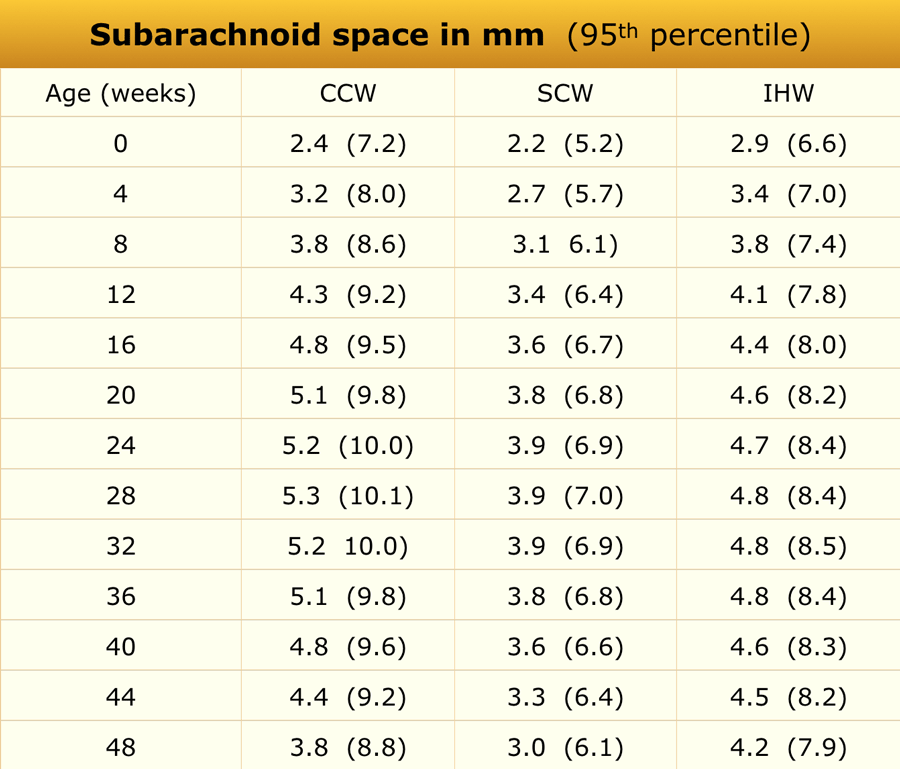
Subarachnoid space
 Adapted from reference 5
Adapted from reference 5
Materials and Methods
Ultrasonographic assessment of the subarachnoid space was performed in 278 full-term healthy Chinese infants.
Measurements were taken in the coronal plane at the level of the foramen of Monro.
Mean values were derived from regression equations, and 95% confidence intervals were calculated from the published data.
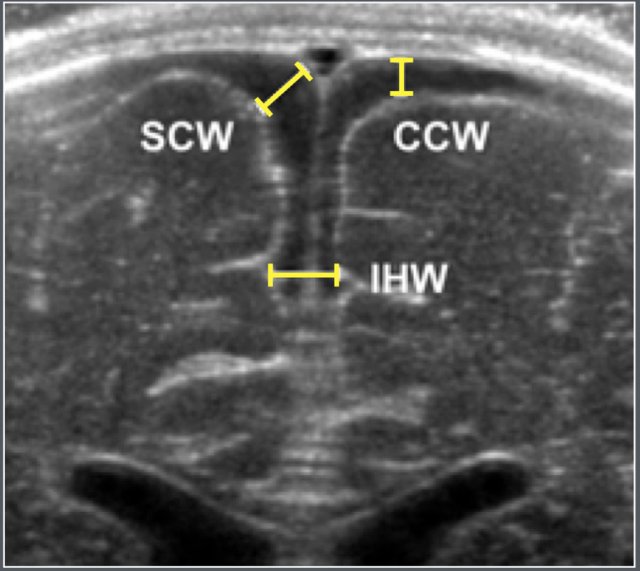
Ultrasonographic parameters
- SCW: Sinu-cortical width
- CCW: Cranio-cortical width
- IHW: Interhemispheric width
Common causes of subarachnoid space enlargement include
- Benign enlargement of the subarachnoid spaces of infancy (BESSI)
- Cerebral atrophy
- Dural sinus thrombosis
Testicle
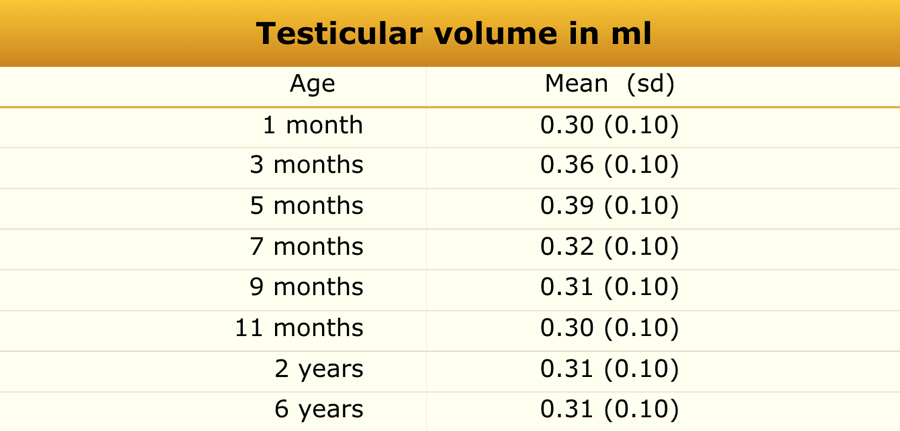 Adapted from reference 19
Adapted from reference 19
Materials and Methods
Ultrasonographic measurements were obtained from 344 boys of various ethnic backgrounds.
No significant differences were noted between ethnicities or between the right and left testes.
Common causes of testicular enlargement include
- Leukemia
- Precocious puberty
- Testicular torsion
- Epididymo-orchitis
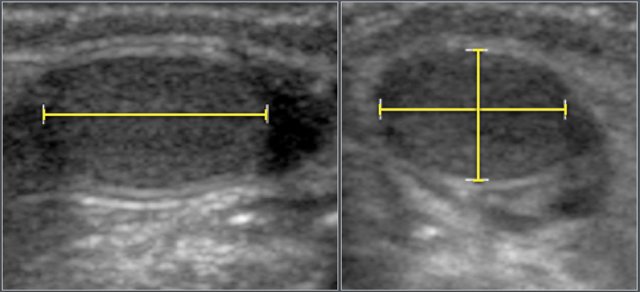
Testicular volume was calculated using the formula:
Length × Width × Height × 0.523
Thymus
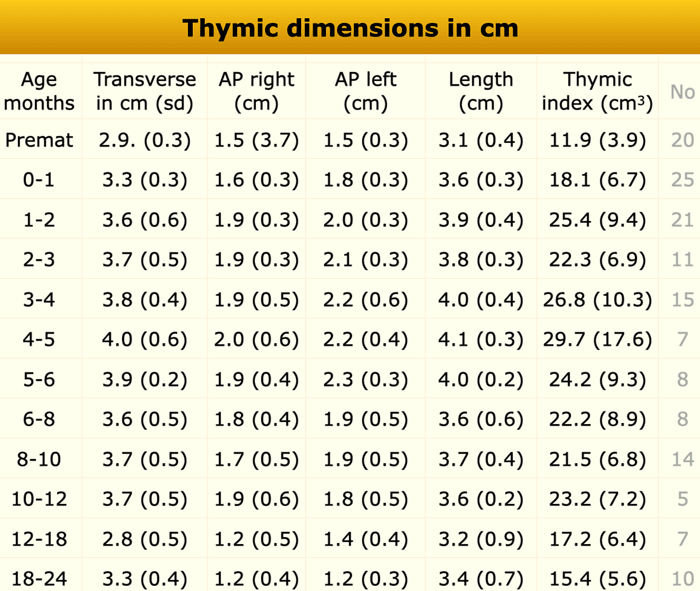 Adapted from reference 22
Adapted from reference 22
Materials and Methods
Mediastinal ultrasonography was performed in 151 healthy infants (79 boys and 72 girls) with no stress-related factorsaffecting thymic size.
Common causes of thymic enlargement include:
- Rebound thymic hyperplasia
- T-cell lymphoma or leukemia
- Thymoma
- Langerhans cell histiocytosis
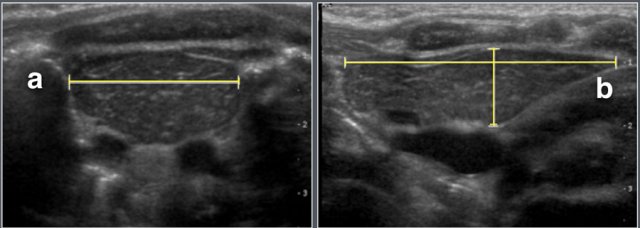
Measurements included
- Maximum transverse diameter
- Right and left lobe anteroposterior diameters
- Craniocaudal (longitudinal) length
The thymic index was calculated as:
Transverse diameter × largest sagittal area
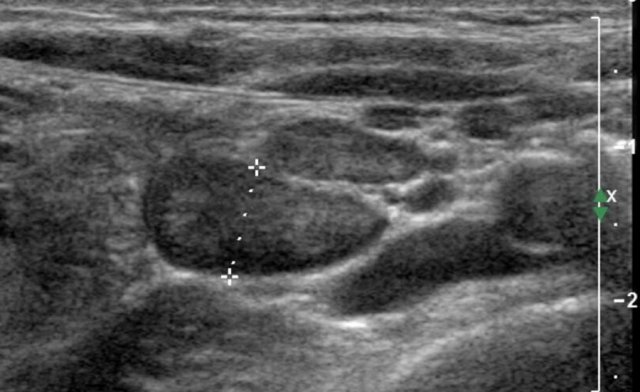
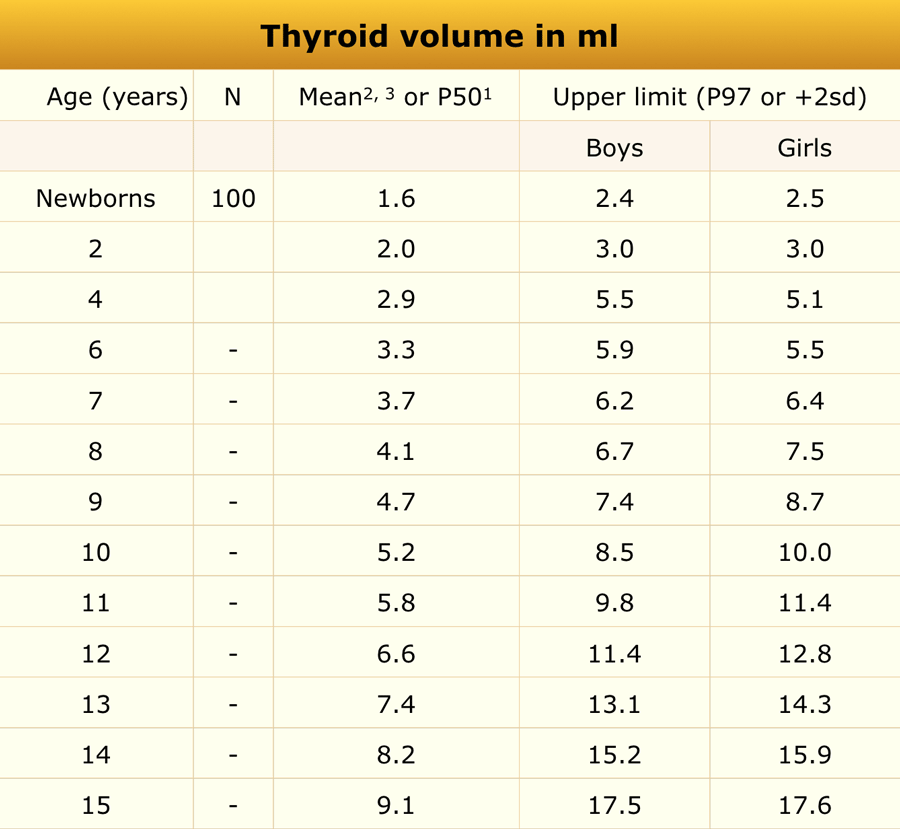
Thyroid gland
 Adapted from reference 1-3
Adapted from reference 1-3
Materials and Methods
Ultrasonographic evaluation of thyroid volume was conducted in:
- 100 English neonates (within the first week of life)
- A subset of iodine-sufficient European children (n = 5,709, aged 6–15 years)
- A group of German children (n = 252, aged 2–4 years)
Common causes of thyroid enlargement include
- Hashimoto’s thyroiditis
- Graves’ disease
- Multinodular goiter
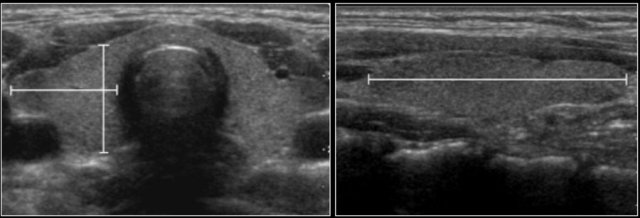
Thyroid volume was calculated as the sum of both lobes, excluding the isthmus.
The ellipsoid formula was used:
Volume = Length × Width × Height × 0.52
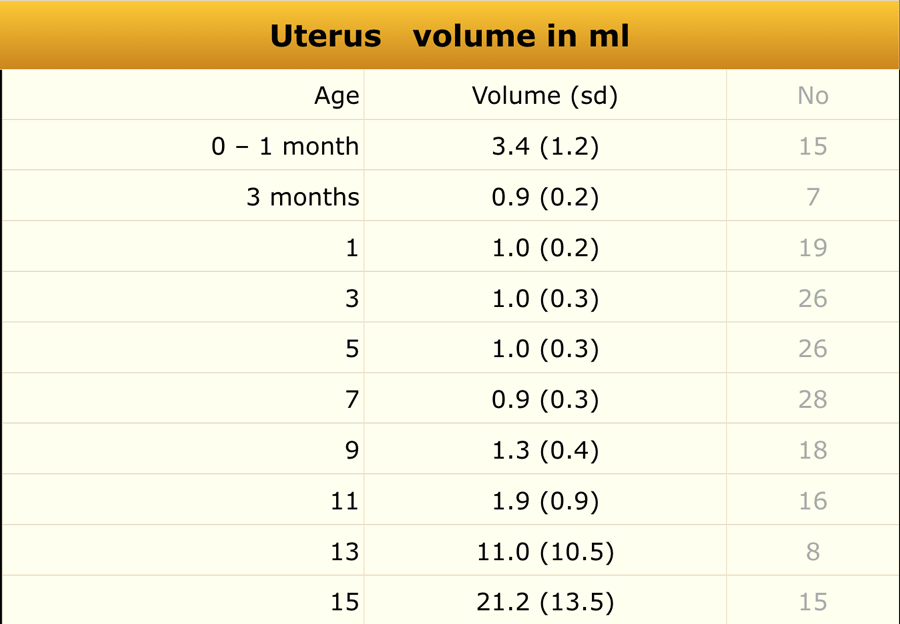
Uterus
 Adapted from reference 20
Adapted from reference 20
Materials and Methods
Ultrasonographic measurements of uterine and ovarian volumes were performed in 178 healthy girls.
Common causes of uterine enlargement include
- Precocious puberty
- Hydro- or hematometrocolpos
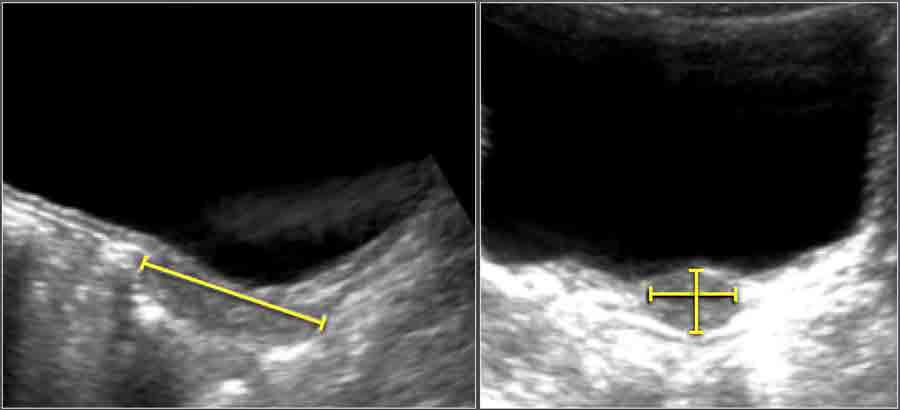
Uterine volume was calculated using the ellipsoid formula:
Length × Width × Height × 0.523
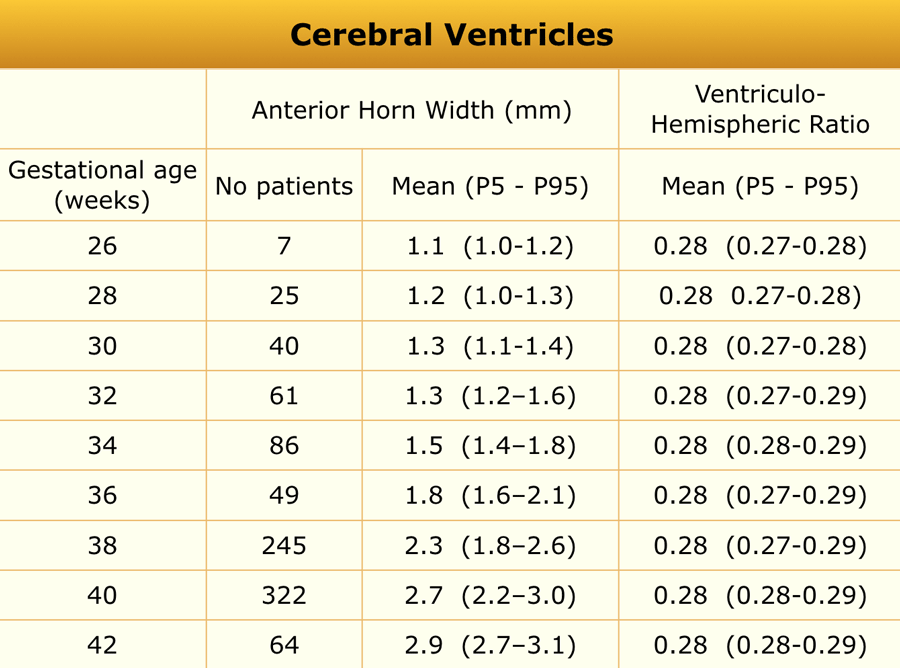
Ventricles
 Adapted from reference 4
Adapted from reference 4
Materials and Methods
An ultrasonographic study was performed in 1,483 neonates (gestational age 25–42 weeks) examined on day 3 of life.
Infants with perinatal asphyxia, CNS infection, intracranial hemorrhage, or craniospinal malformations were excluded.
Common causes of ventriculomegaly include
- Congenital malformations (e.g., holoprosencephaly)
- Obstructive hydrocephalus
- Communicating hydrocephalus
- Cerebral atrophy
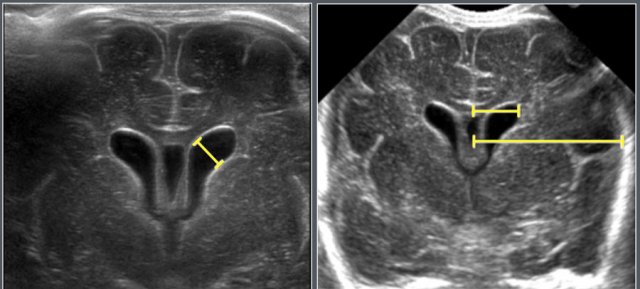
Measurements
- Anterior horn width (AHW)
- Ventriculohemispheric ratio (VHR)
Measured on coronal images at the level of the foramen of Monro.