Bosniak Classification 2019
Cystic Renal Masses
Chris Lunt and Frederieke Elsinger
BC Cancer Agency Vancouver and Luzerner Kantonsspital
Publicationdate
In this article we describe the 2019 Bosniak classification of renal cystic lesions.
The goals of the new 2019 Bosniak classification are to reduce interobserver variability, improve the precision rate of malignancy within each category and to increase specificity and thereby reducing the rate of unnecessary treatment of benign lesions.
Overview
 A cystic renal mass is defined as a lesion in which <25% of the mass is composed of enhancing tissue
A cystic renal mass is defined as a lesion in which <25% of the mass is composed of enhancing tissue
The Bosniak 2019 classification defines a cystic renal mass as one in which <25% of the mass is composed of enhancing tissue in order to avoid an aggressive necrosed solid renal mass being termed Bosniak IV.
Bosniak I and Bosniak II masses that are characterized as benign may be described as “cysts” and the term “cystic renal mass” should be applied to Bosniak IIF, III and IV lesions.
Terms such as ‘complicated cyst’ or ‘complex cyst’ can be confusing and should be avoided.
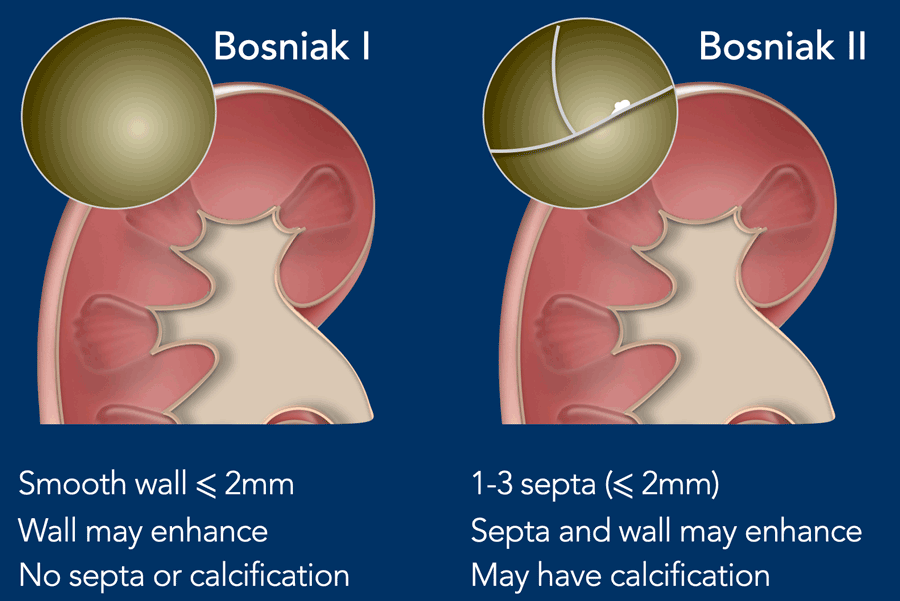
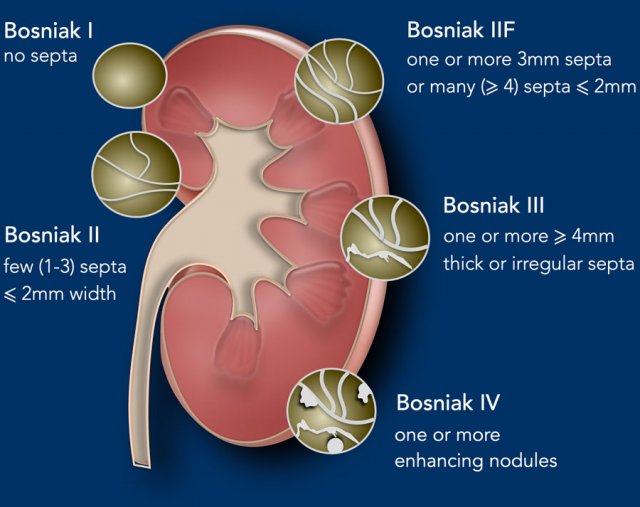
Bosniak I
- Well-defined, thin (≤ 2 mm) smooth wall; homogeneous simple fluid (- 9 to 20 HU); no septa or calcifications; the wall may enhance
Bosniak II
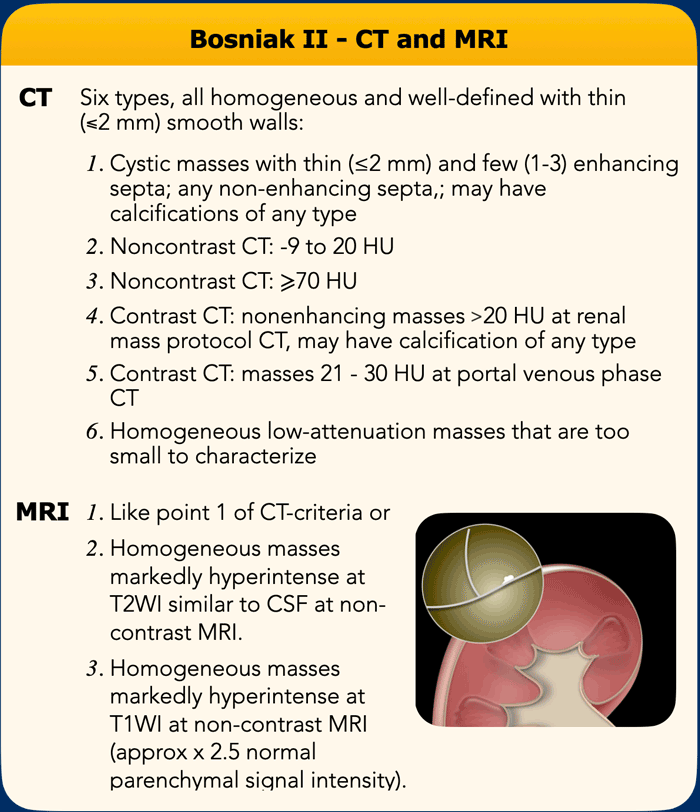
Six types, all well-defined with thin (≤ 2 mm) smooth walls:
- Cystic masses with thin (≤ 2 mm) and few (1–3) septa; septa and wall may enhance; may have calcification of any type
- Homogeneous hyperattenuating (≥ 70 HU) masses at non-contrast CT
- Homogeneous non-enhancing masses > 20 HU at renal mass protocol CT. May have calcification of any type
- Homogeneous masses -9 to 20 HU at non-contrast CT
- Homogeneous masses 21 to 30 HU at portal venous phase CT
- Homogeneous low-attenuation masses that are too small to characterize
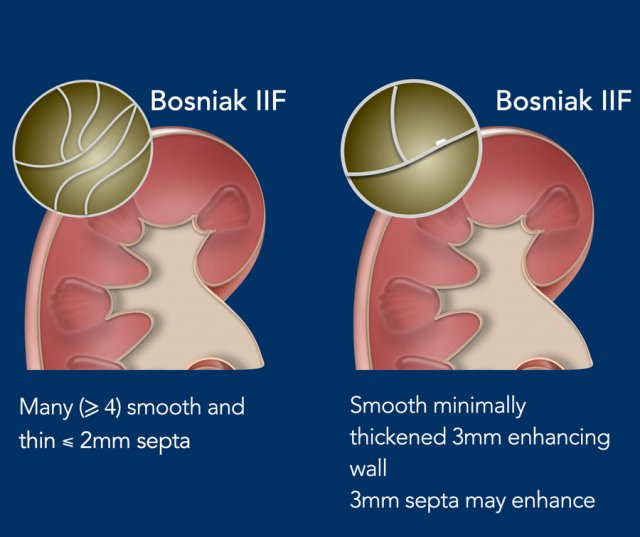
Bosniak IIF
Two types:
- Cystic masses with a smooth minimally thickened (3 mm) enhancing wall, or smooth minimal thickening (3 mm) of one or more enhancing septa.
- Cystic masses with many (≥ 4) smooth thin (≤ 2 mm) enhancing septa.
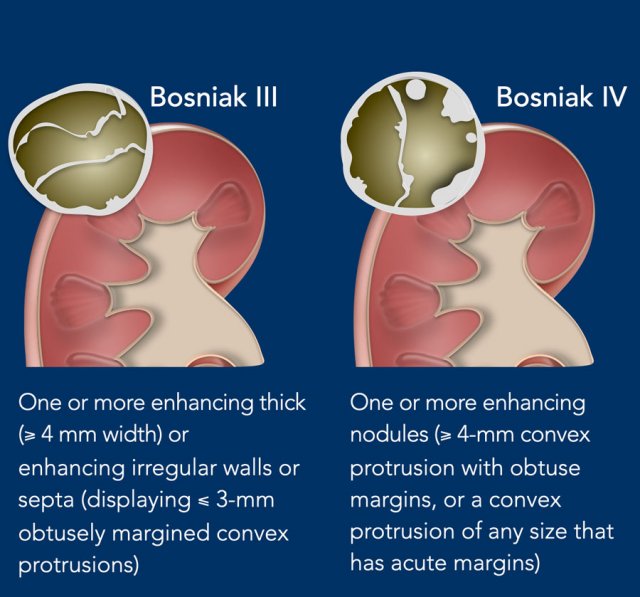
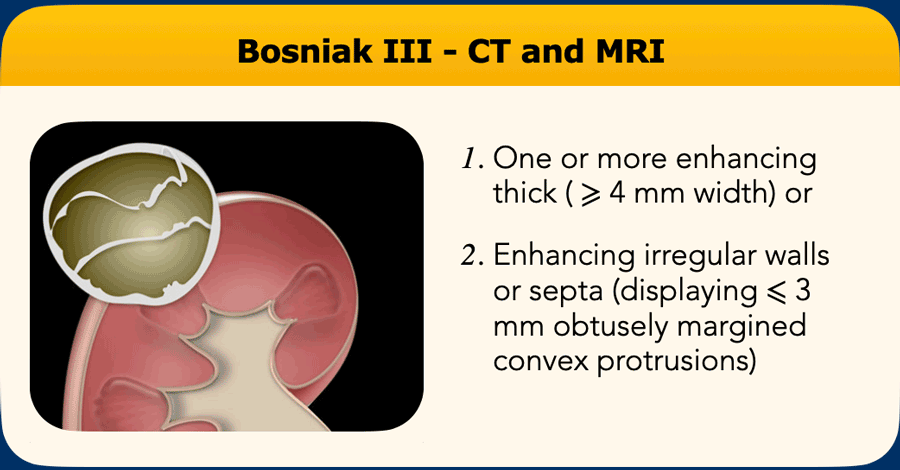
Bosniak III
One or more enhancing thick (≥ 4 mm width) or enhancing irregular (displaying ≤ 3-mm obtusely margined convex protrusion[s]) walls or septa.
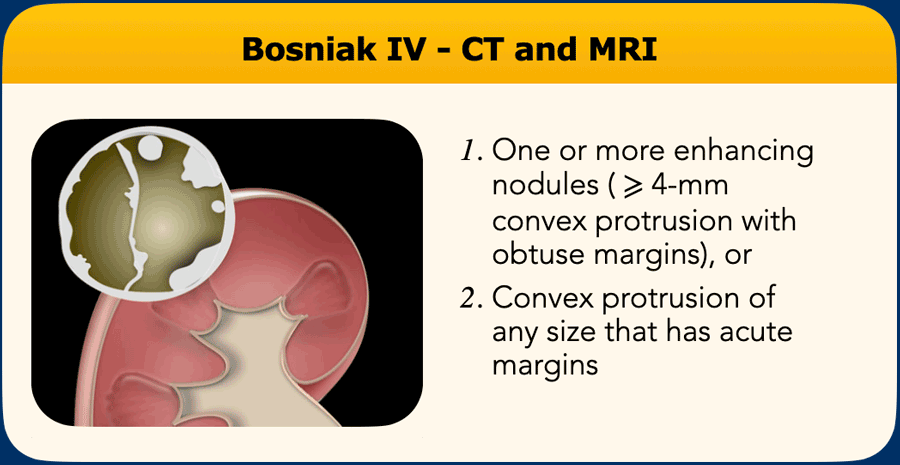
Bosniak IV
One or more enhancing nodules (≥ 4-mm convex protrusion with obtuse margins, or a convex protrusion of any size that has acute margins)
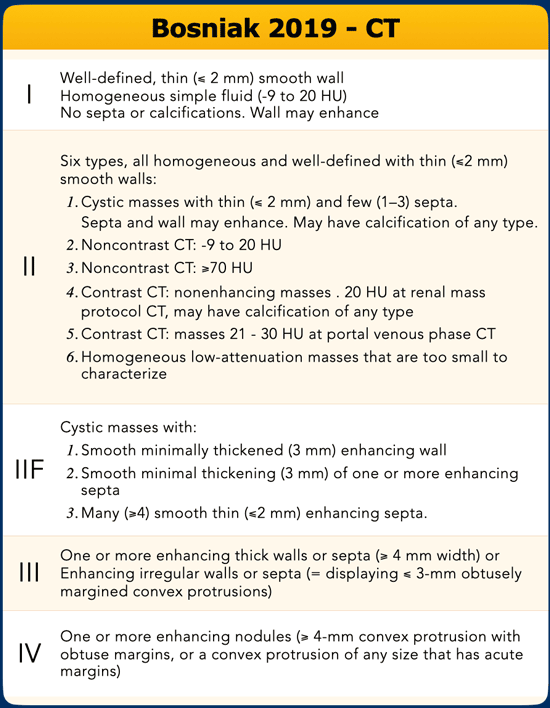
This table summarizes the Bosniak 2019 classification..
 Portal venous scan of a cyst with mean HU of 25 in the anterior right Kidney. According to the new Bosniak criteria all cyst with HU <30 are likely benign and can be classified as Bosniak II without any additional imaging
Portal venous scan of a cyst with mean HU of 25 in the anterior right Kidney. According to the new Bosniak criteria all cyst with HU <30 are likely benign and can be classified as Bosniak II without any additional imaging
Malignancy rate
Bosniak I masses are universally considered to be benign, and although there are occasional case reports of malignancy being found in these lesions, this is thought to be due to incorrect scan technique or incorrect image interpretation leading to incorrectly assigning a Bosniak I grade.
Malignancy rates in Bosniak II lesions are <1% and may be as low a 0%. A caveat to this is in patients with Von Hippel Lindau syndrome, hereditary leiomyomatosis and other RCC syndromes where benign appearing cystic masses may still harbor malignancy and the application of the Bosniak system is not recommended.
The incidence of malignancy in Bosniak IIF lesions is reported between 0-38% likely owing to differences in subjective grading of imaging features as well as strong selection bias whereby only the more worrisome lesions are resected. However, lesions in which there is progression of features from IIF to category III or IV have a high rate of malignancy of 85%, comparable to lesions initially characterised as Bosniak IV.
Bosniak III lesions are considered indeterminate with around half being malignant. Current practice regarding resection or observation varies between institutions and depends heavily on lesion size, patient comorbidities and surgeon preference.
Bosniak IV lesions are found to be malignant in around 90% of cases and treatment is recommended in most cases if patient characteristics allow
The system is used to predict the likelihood of cancer, not the biologic behavior.
It is unclear which criteria are more predictive for cancer aggressiveness than others.
Size and growth rate are not included in the updated classification. It is however likely that the smaller the lesion, the more likely it is to be benign. Growth rate and change of morphology do however play an important role in the surveillance of lesions.
It is important to include patients’ age, comorbidities, life expectancy, personal preferences and risk tolerance into the considerations to treat or observe.
 Solid renal tumor with small cystic or necrotic components
Solid renal tumor with small cystic or necrotic components
When not to apply Bosniak
The Bosniak classification should not be applied to lesions with an infectious, inflammatory or vascular etiology.
Lesions with a solid component of > 25% are likely necrotic solid masses. These necrotic solid masses, as opposed to cystic masses, have a less indolent behavior.
It is therefore important not to confuse indolent cystic cancer with more aggressive forms.
Lesions with abundant thick nodular calcifications on CT can mask enhancement. In these lesions MRI with subtraction is advised to rule out enhancing soft tissue components.
Hyperattenuating non-enhancing lesions larger than 3 cm and heterogeneous non-enhancing lesions on CT can also benefit from further evaluation with MRI to exclude enhancement before assigning a Bosniak category.
case 1
CT of a solid lesion with smaller cystic/necrotic components.
As more than 25% of the mass is composed of solid tissue this likely represents a necrotic mass in stead of a cystic lesion.
Bosniak criteria should not be used.
 Solid renal tumor with cystic components
Solid renal tumor with cystic components
case 2
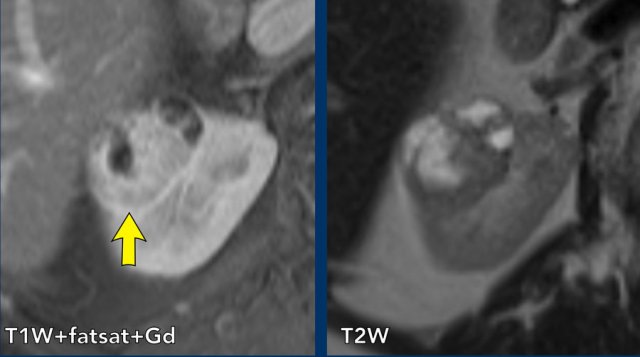
MRI of a more solid than cystic lesion in the right kidney.
 Renal abscess
Renal abscess
case 3
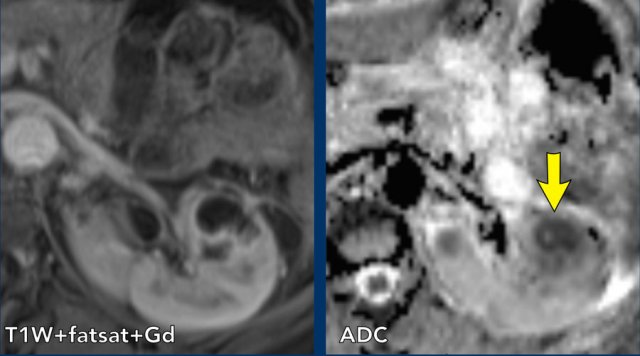
There is a non-enhancing area in the left kidney on the T1W-image.
This area has low values in the ADC map in keeping with diffusion restriction.
This proved to be an abscess.
Definitions
Septa
A septum is defined as a linear or curvilinear structure that connects two surfaces.
Up to 3 septa are considered “few” and in keeping with a Bosniak II lesion.
4 or more septa are termed “many” and if enhancing are features of a 2F lesion (in the absence of more worrisome features)
In the left diagram there are 2 septa connecting two surfaces (Bosniak II), and in the right diagram there are 5 different septa, defined as Bosniak IIF.
Enhancement
Prior versions of the Bosniak classification divided enhancement between “perceived” and measurable, and all masses in which an area of enhancement could be measured could only be categorised as Bosniak III or IV.
However, there was no evidence base for the distinction between perceived and measurable enhancement increasing risk of malignancy
In the 2019 classification all enhancement is considered equal.
Enhancement can be unequivocally perceived when comparing non-contrast and contrast-enhanced images performed using the same acquisition technique or ‘measurable’ using conventionally sized regions of interest” (not pixel values).
Specifically an increase of ≥20 HU on contrast-enhanced CT, or ≥15% signal intensity on contrast enhanced MR.
If a feature is not unequivocally enhancing visibly and is too small to measure accurately then it is considered non-enhancing.
Image
T2W coronal image of a cyst with many septa in the left kidney. On the T1W fatsat after contrast, these septa show obvious enhancement in comparison to the pre-contrast sequence.
A cyst with many, thin septa is categorized as a Bosniak IIF
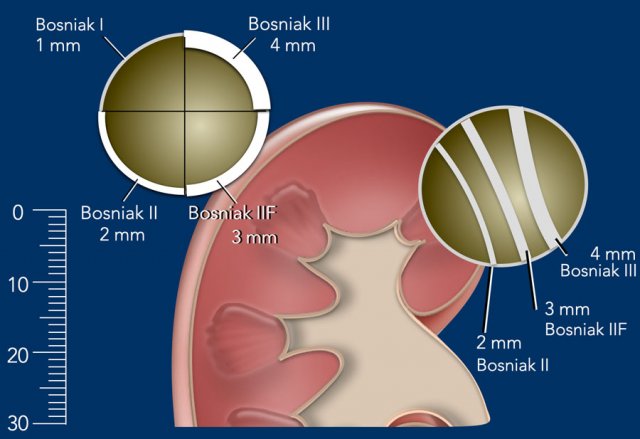
Septal and wall thickness
Although there is still likely to be some inter observer variation in the measurement of enhancing septal and wall thickness, the new 2019 guidance provides values for thickness in each Bosniak category, replacing the prior descriptive classification of “minimally thickened” or “thickened”.
A cyst with smooth thin enhancing wall ≤ 2mm thickness without septa is considered a Bosniak I cyst.
A smooth ≤ 2mm enhancing wall with 1-3 septa ≤ 2mm thickness is Bosniak II
A smooth and minimally thickened wall or septa (3mm) is considered Bosniak IIF
Any smoothly thickened wall or septa ≥ 4mm is categorized as Bosniak III.
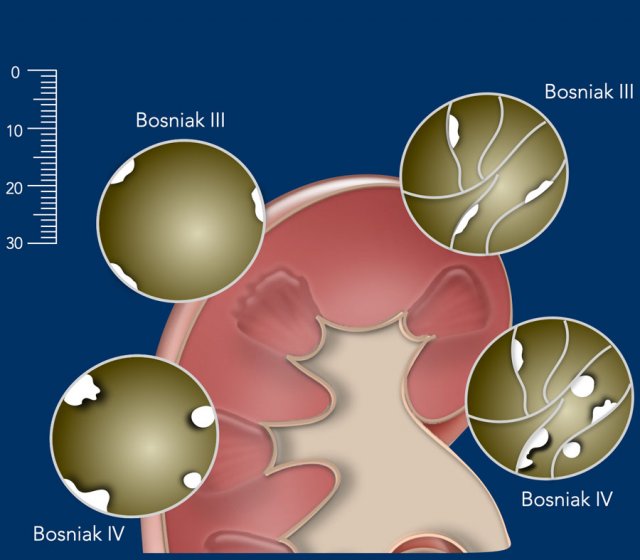
Wall irregularity and Nodularity
The distinction between irregularity of enhancing wall or septa and a nodule relates to the angle formed with the associated wall or septum and the thickness.
Enhancing areas which form acute angles with a wall or septum are considered nodules and are always categorized as Bosniak IV features.
Enhancing areas which form obtuse margins with the septal or mural surface are considered thickening if ≤3mm.
An enhancing area with obtuse margins is considered a nodule if ≥4mm when measured perpendicular to the underlying surface.
If an area of obtuse angled thickening is present on both sides of a septum then the combined thickness on both sides of the septum should be measured, excluding the thickness of the underlying septum itself.
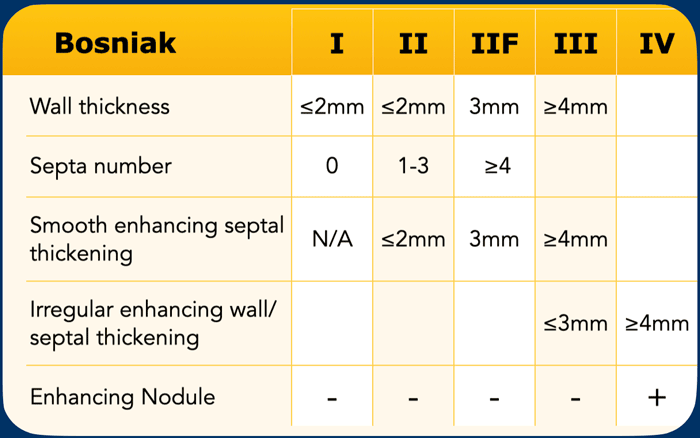
This table summarizes the different measurements of the wall and septal thickness in the Bosniak classification.
Bosniak I
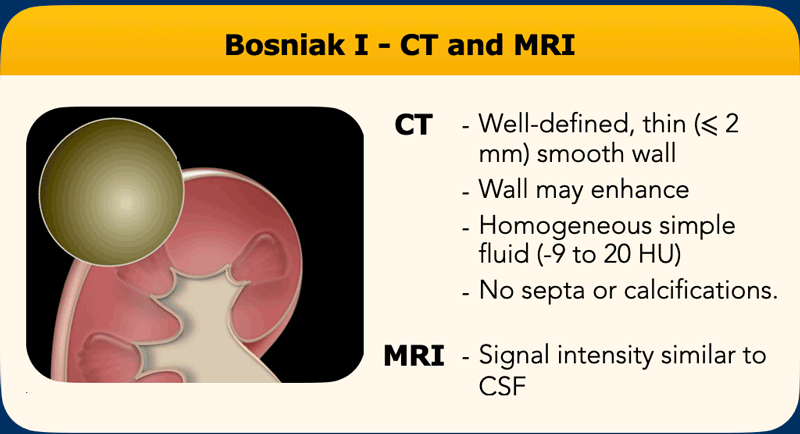
On contrast CT Bosniak I cyst are well defined with a thin (≤2mm) smooth wall and contain homogenous, simple fluid (-9 – 20 HU) and no septa or calcifications.
The wall may enhance.

case 1
CT in portovenous phase.
There is a typical Bosniak I cyst in the left kidney.
The cyst has a well-defined thin smooth wall.
There are no septa or calcifications.
The content of the cyst is homogeneous and has a low HU.
MRI characteristics of Bosniak I cysts are the same as on CT.
The fluid within the cyst has a signal intensity similar to CSF.
case 2
Right kidney with typical Bosniak I cyst on MR
Bosniak II
In the 2019 version of the Bosniak classification more types of lesions can be characterized as Bosniak II (see table) in an attempt to increase specificity and to reduce the need to image or treat likely benign lesions.
Bosniak II lesion are now allowed to show enhancement, which is no longer a Bosniak III characteristic.
Most incidental kidney lesions are detected on single phase portal venous studies. If these lesions are homogeneous and have a HU of 21-30, malignancy is highly unlikely and Bosniak II can be applied.
Masses that are evaluated with a renal specific contrast protocol and have a HU of > 20 and show no enhancement are also assigned Bosniak II.
All thin walled cystic masses with enhancing septa and/or any type of calcification can now be categorized as Bosniak II, as long as the septa are few (1-3) and thin (≤ 2mm).
Homogeneous masses with Houndsfield units of -9-20 or ≥70 on non-contrast CT, as well as lesions -too small to characterize- but otherwise homogeneous and low-attenuating, can be placed in the Bosniak II category.
Many masses are discovered incidentally on CT or MR examinations performed for other indications not using a dedicated renal imaging protocol. Despite this, many masses can be safely described as benign.
Well defined homogeneous masses seen on non-contrast CT measuring between -9 to 20 HU or >70 HU are highly likely to be benign cysts and can be ignored.
On contrast enhanced CT the adjacent enhancing renal parenchyma may increase measured density (pseudo enhancement) within benign cysts. Therefore, cystic masses measuring <30 HU in the portal venous phase are also considered benign.
On unenhanced MR, well defined homogeneous masses which are hyperintense on T1 (around 2.5x normal parenchymal intensity) or well defined masses with T2 signal intensity similar to CSF are considered benign.
Small masses may not be characterizable due to partial voluming if the slice thickness is more than half the diameter of the mass. In practice, pseudo enhancement can occur in masses up to 1.5cm in diameter and if these otherwise appear homogeneous they should be considered benign Bosniak II lesions.
case 1
Bosniak II cyst with only a few, thin, calcified septa.
 Bosniak II cyst
Bosniak II cyst
case 2
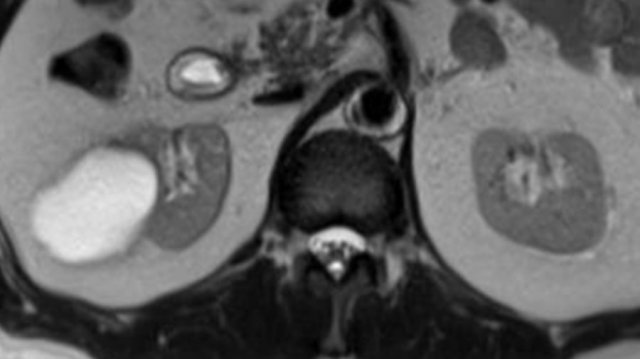
On the T2W-image a cyst with 3 smooth thin septa in the medial aspect of the right kidney (arrow).
The fluid has a high T2W signal intensity.
On the T1W-image post Gadolinium there is enhancement of the septa.
The lesion is classified as a Bosniak II cyst.
No follow up is indicated.
Notice that there is a second solid renal mass posteriorly.
case 3
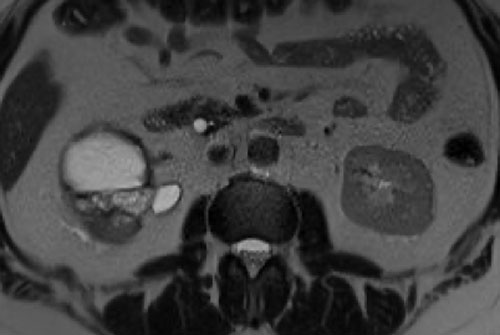
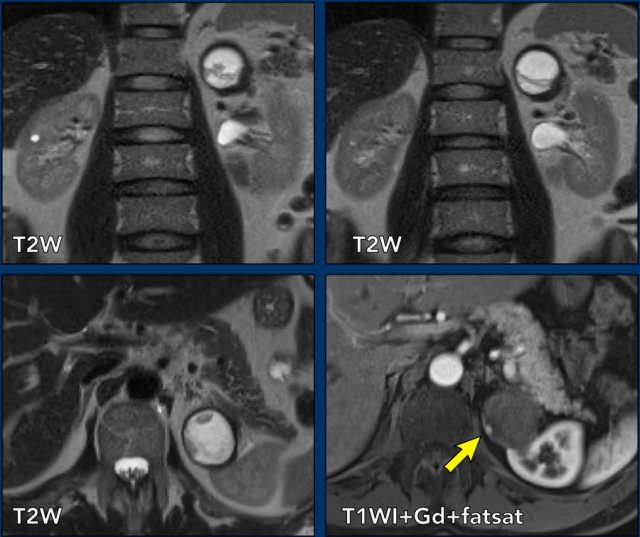
The images are axial T2W, a coronal T1W image with fatsat and Gadolinium and finally a coronal T2W.
There is a cystic lesion within the right kidney with many (> 4) thin septa.
The septa are better seen on the axial images .
The septa show no enhancement.
According to the old classification this lesions would be classified as IIF.
In the updated 2019 classification non-enhancing septa cannot be counted as such, and the lesion is therefore downgraded to a Bosniak II cyst.
This cyst had previously hemorrhaged and didn’t show any changes in follow-up over 5 years.
 Click on image for enlarged view.
Click on image for enlarged view.
case 4
Small masses may not be characterizable due to partial voluming if the slice thickness is more than half the diameter of the mass.
Pseudoenhancement can occur in masses up to 1.5 cm in diameter.
If these lesions otherwise appear homogeneous, they should be considered benign Bosniak II lesions.
Images
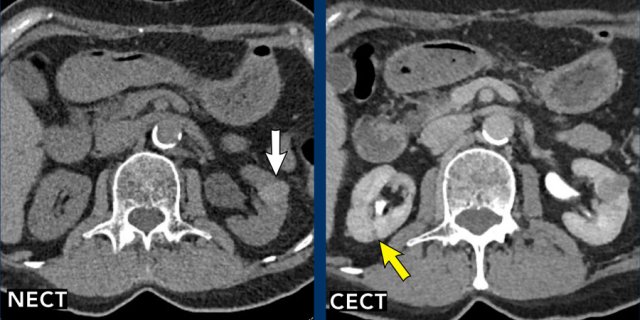
Lesion 1 (yellow arrow)
A homogeneous, hypodense lesion is seen in the posterior right kidney. This lesion is too small to characterize and is classified as Bosniak II.
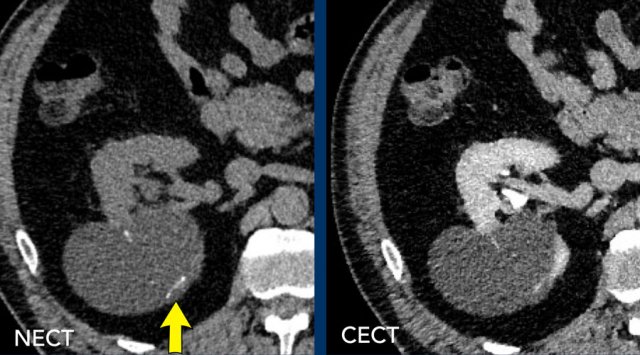
Lesion 2 (white arrow)
On the non-enhanced CT (NECT) there is a hyperdense lesion in the left kidney with HU > 70, which would normally correspond to a Bosniak II lesion (white arrow). A contrast-enhanced CT (CECT) in the portovenous phase shows no significant contrast uptake but there is an inhomogeneous appearance.
This requires additional imaging with MRI (see next images).
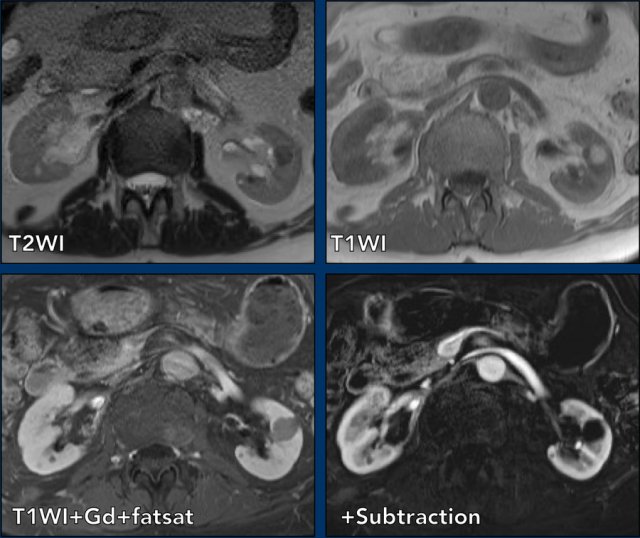
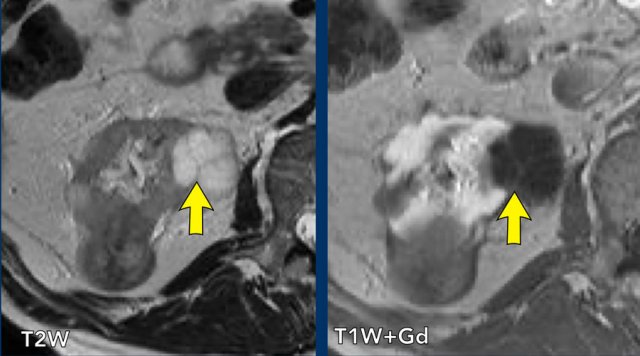
MRI of the same patient.
The lesion is hypointense on T2WI and hyperintense on T1WI.
There is no contrast enhancement on the subtraction sequence.
On MRI the lesion could be confirmed as Bosniak II.
Bosniak IIF
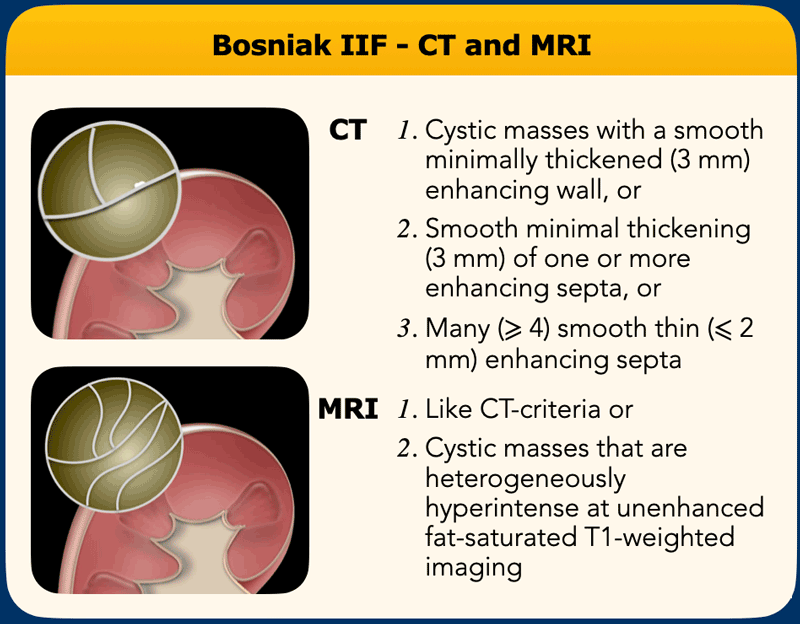
Not much has changed in the IIF category, besides that the criteria are now more well defined. Cystic IIF masses have either more than a few (≥4 ) thin (≤2mm) septa or few (1-3) minimally thickened (3 mm) septa both on CT and on MRI.
Heterogeneous masses on CT without significant contrast enhancement should be considered as incompletely characterized. MRI is recommended to further asses these lesions before applying the Bosniak criteria.
New in the IIF section are cystic masses that are heterogeneously hyperintense on unenhanced fat saturated T1W-imaging.
This is the only mass type that is categorized greater than Bosniak II without enhancing features. The reasoning behind this is that papillary cancers can present with this finding.
Progression over time is a strong indicator of malignancy, but is not included in the Bosniak classification.
case 1
Scroll through the images.
Axial T2WI and coronal T1WI with fatsat and Gadolinium.
There is a cystic mass in the left kidney with many thin enhancing septa.
The lesion is classified as Bosniak IIF.

case 2
There is a cystic mass in the right kidney with many (> 4) smooth thin enhancing septa.
The lesion is classified as Bosniak IIF.
Bosniak III
According to the previous criteria, Bosniak III masses are ‘indeterminate’ with about half of the resected masses being benign, resulting in potential harm of treatment without clinical benefit.
In 2019 the criteria have been more clearly defined. Any cystic mass with one or more irregular septa or irregular enhancing wall of 3 mm or smooth thickened wall or septation of ≥4mm are considered Bosniak III.
The term ‘irregular’ is defined as diffuse convex protrusions that have obtuse margins with the wall or septa (see section wall irregularity above).
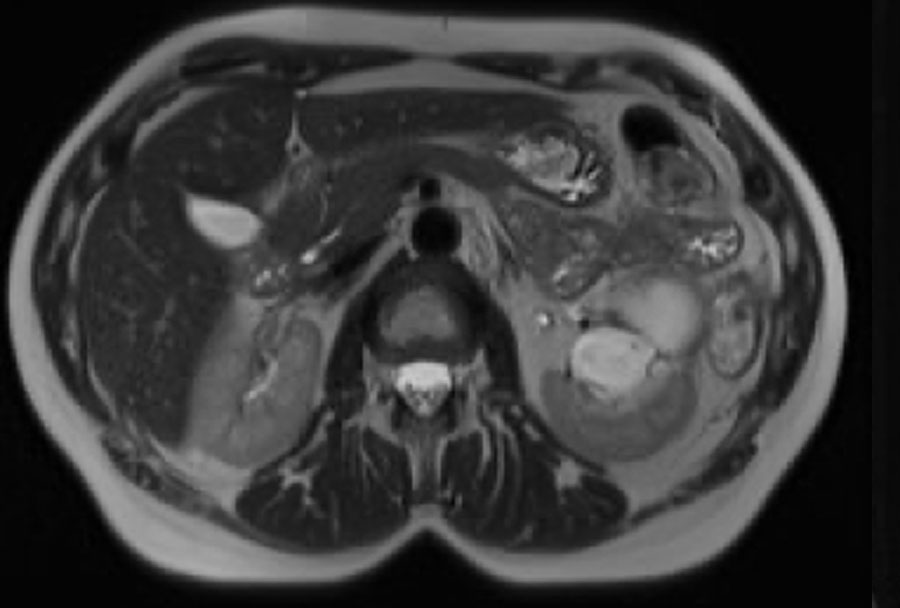
case 1
MRI of an exophytic cortical cyst in the left kidney with few, irregular thickened (3 mm) septa with obtuse margins which enhance after contrast, in keeping with findings of a Bosniak III cyst.
It was decided to surgically remove the lesion and it proved to be a clear cell carcinoma.
Bosniak IV
Cystic masses with Bosniak IV characteristics are highly likely to be malignant (90%) and present with larger soft tissue components and thick enhancing irregular walls.
They are therefore more easily recognized as suspicious lesions.
Nodules are defined as focal enhancing convex protrusions of any size with acute angles to the septa or wall or a protrusion of over 4 mm with obtuse margins with the wall or septa.
Cystic masses with soft tissue components > 25% are no longer cystic masses but necrotic solid masses and the Bosniak criteria do no longer apply to these masses.
case 1
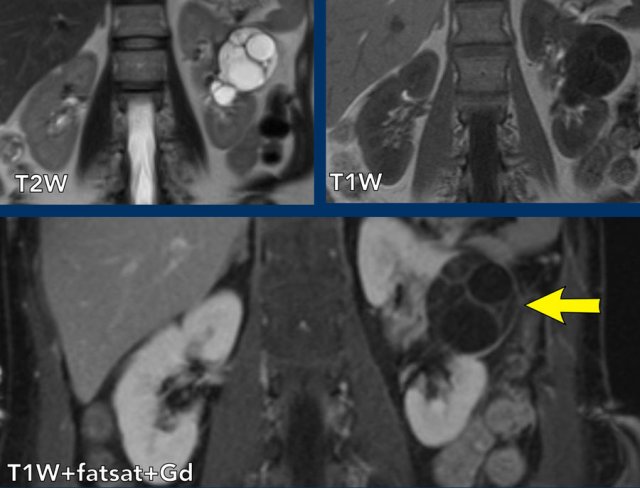
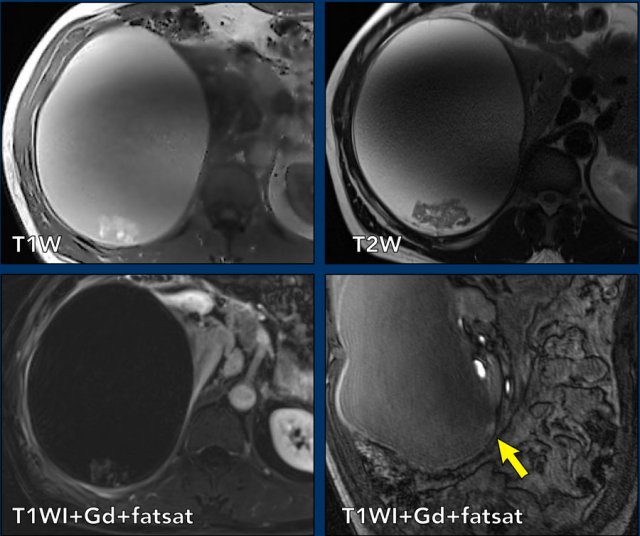
The images show a complex large right renal cyst with T1 and T2 hyperintense internal fluid and T1 hyperintense debris, which shows mild enhancement on the subtraction image.
This cyst also has an enhancing mural nodule (see arrow coronal images), classifying it as a Bosniak IV lesion.
The kidney was removed and the cyst represented a papillary renal cell carcinoma
case 2
The images show a cystic mass with a thick walled (< 4mm) cyst with a few irregular thickened septa.
On the post contrast images there is no enhancement of the septa or wall but an enhancing mural nodule can clearly be identified (arrow).
This therefore represents a Bosniak IV lesion. The lesion was excised and proved to be a clear-cell carcinoma.
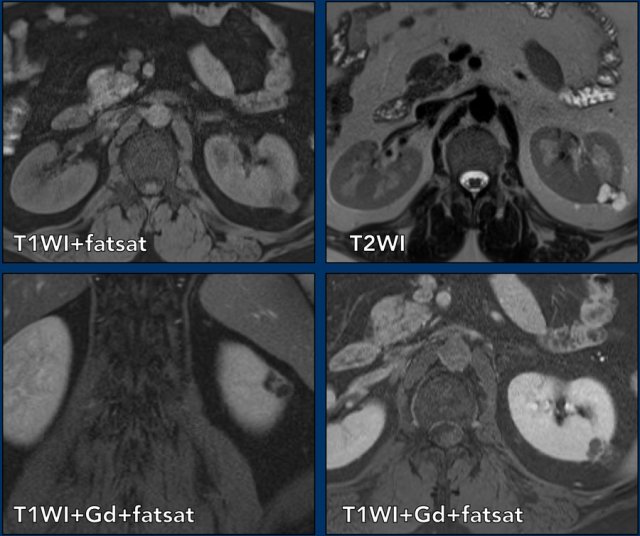
case 3
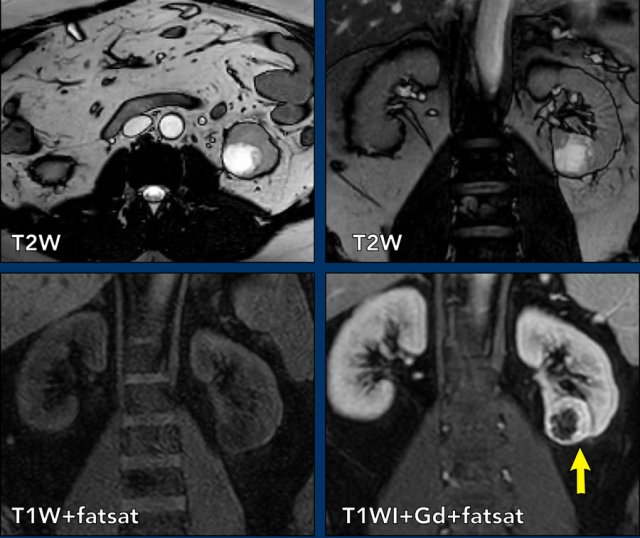
The axial and coronal T2 images show a cystic lesion within the lower pole of the left kidney with a thickened irregular wall.
As less than 25% of the lesion is comprised of solid tissue, the lesion should be classified as a cystic mass instead of a cystic solid renal tumor.
In the pre- and post-contrast coronal T1 fat suppressed images a wall thickness of more than 4 mm was measured (arrow).
The lesion was classified as a Bosniak IV cystic mass.
The mass was excized and proved to be a clear cell carcinoma.
case 4
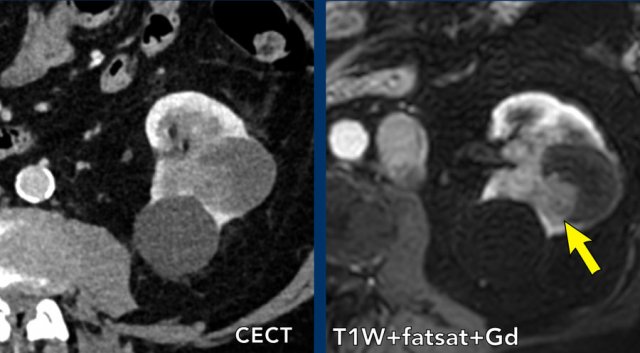
Portovenous scan with an inhomogeneous cystic lesion in the left kidney.
The hyperdense area shows enhancement on the T1W-image with fatsat, in keeping with a solid nodule in a Bosniak 4 cyst.