Lung Segments and Bronchi
Onno Mets¹, David Heineman² and Robin Smithuis³
¹Radiology department and ²department of cardiothoracic surgery of the Amsterdam University Medical Center and ³Alrijne hospital in Leiden, the Netherlands
Publicationdate
The lung is anatomically divided into several lobes and subsequently into multiple segments, resembling the anatomical structure of the liver. These segments are functionally independent and can be individually affected by diseases or targeted during surgical procedures.
Familiarity of the radiologist with the anatomical divisions of the lung is essential for various aspects of clinical practice, as it may help detect abnormalities more easily, localize pathology more precisely, and helps in the communication to surgeons, pulmonologists, and other members of the multidisciplinary team.
We will first
describe the anatomy of the lung with illustrations and scrollable CT-images.
Second, we will show some cases to illustrate the added value of detailed
knowledge of lung segmental anatomy.
Anatomy

Pulmonary segments - illustration
Right Upper Lobe (in blue)
Apical segment (RB1) - Posterior segment (RB2) - Anterior segment (RB3)
Middle lobe (in green)
Lateral segment (RB4) - Medial segment (RB5)
Right Lower Lobe (in orange)
Superior segment (RB6) - Medial basal segment (RB7) - Anterior basal segment (RB8) - Lateral basal segment (RB9) - Posterior basal segment (RB10).
The Superior and Medial basal segment of the right lower lobe are not visible in this illustration because they are located posterior to the right upper and middle lobe.
Left Upper Lobe (in blue)
Apicoposterior segment (LB1/2) - Anterior segment (LB3)
Lingula (in green)
Superior segment (LB4) - Inferior segment (LB5)
Left Lower Lobe (in orange)
Superior segment (LB6) - Anterior basal segment (LB8) - Lateral basal segment (LB9) - Posterior basal segment (LB10).
The Superior segment of the left lower lobe is not visible in this illustration because it is located posterior to the left upper lobe.
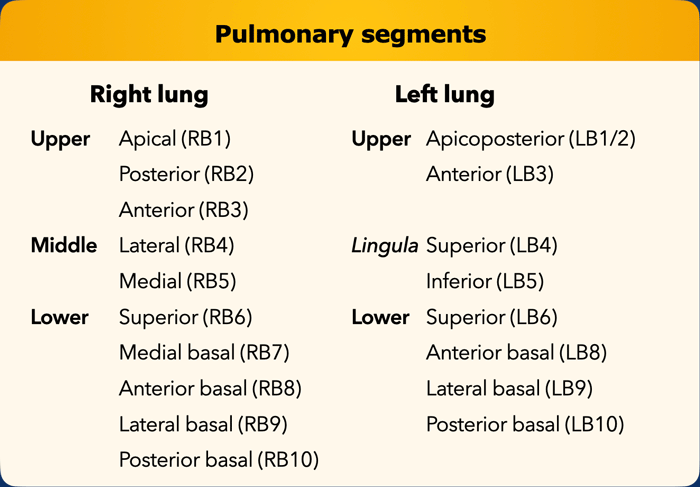 List of all pulmonary segments. In brackets the numeration according to the Boyden classification, which is often used by surgeons and pulmonologists. Note that segment 7 is omitted on the left side.
List of all pulmonary segments. In brackets the numeration according to the Boyden classification, which is often used by surgeons and pulmonologists. Note that segment 7 is omitted on the left side.
There is some symmetry in the
segmental anatomy of the lungs, since the left is only slightly different from
the right lung.
The right lung has three lobes (ie. upper, middle and lower) with ten segments,
while the left lung has two lobes (ie. upper and lower) with less segments.
In
the left upper lobe the apical and posterior segment share a common trunk
segmental bronchus and are combined into the apicoposterior segment.
The lingula
is part of the left upper lobe and has a superior/inferior orientation, while
the middle lobe on the right is separate from the upper lobe and has a
medial/lateral orientation.
In the left lower lobe there is an anterior basal segment, but no separate medial basal segment (LB7) due to the left-sided position of the heart in the chest cavity.
Please note that both radiological
and surgical literature may differ somewhat regarding naming of the left-sided
segments, with some articles mentioning an anteromedial basal segment (LB7/8)
in the left lower lobe.
Also, the apicoposterior segment of the left upper lobe
is sometimes regarded as two separate segments that only share a common trunk.

Bronchial tree
From the
trachea and main bronchi, the airways further divide into the lobar (ie.
secondary) bronchi, and thereafter into the segmental (ie. tertiary) airways.
Pulmonary segments are based on this generation of bronchi.
Pulmonary
segments are a functionally independent unit of the lung, supplied by their own
segmental bronchus and pulmonary artery and with their own venous and lymphatic
drainage.
This allows for loss of a segment, without affecting the adjacent
segments.
Surgeons use this knowledge for planning and executing segmentectomies, a procedure increasingly favoured over lobectomy for small peripheral lesions without lymph node involvement, as it is hypothesized that preservation of lung tissue will benefit pulmonary function post-operatively without compromising oncological treatment principles.

Bronchi on CT
Scroll through the images to see how the trachea divides into the right and left main bronchus and further into lobar and segmental bronchi.

Lungsegments on CT
Scroll through the images to see how the lungs are divided into segments.
Congenital Bronchial variants
Some variation in the prevailing patterns of bronchial branching exists.
To detect abnormalities, knowledge of several anatomic principles is crucial, especially the classic segmental branching as described above.
Tracheal and accessory cardiac bronchus are rather notable airway variants, but smaller and less conspicuous variations in both airway and vascular anatomy occur at the (sub)segmental level.

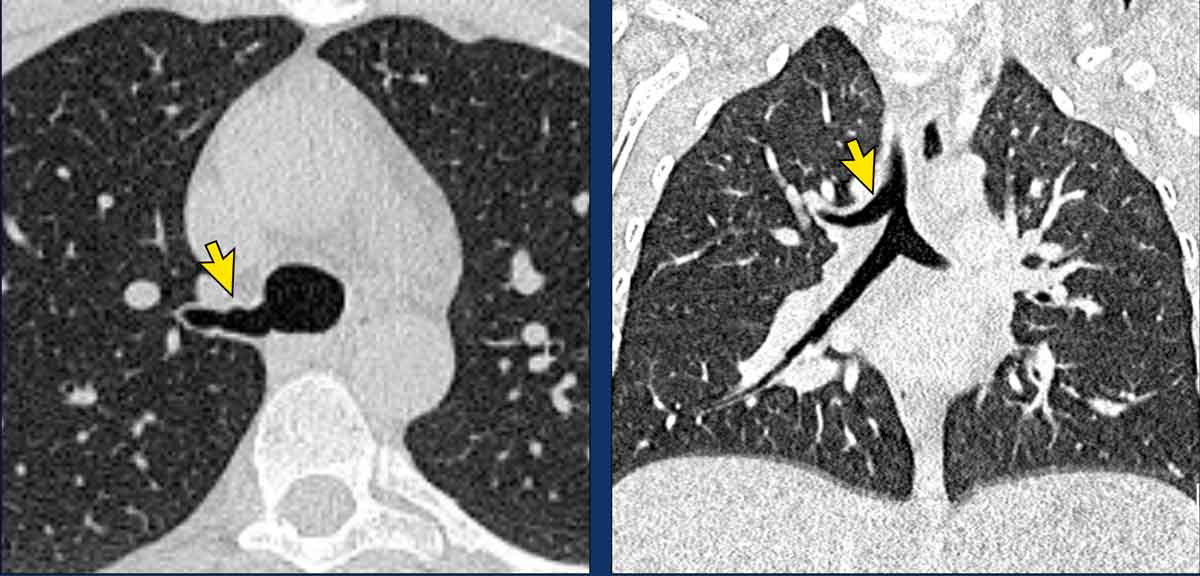
Lobus vena azygos
A very common variant in lung anatomy is the azygos lobe, where an
accessory fissure is present either with or without the azygos vein coursing
through the fissure.
Accessory fissures elsewhere as well as incomplete fissures are also a
common finding and mainly of no clinical
relevance.
Images
Azygos lobe in a 74 y.o male with the azygos vein in the normal position (yellow arrow).

Here another case, where the azygos vein courses through the azygos fissure (arrowheads).
 Tracheal bronchus
Tracheal bronchus
Tracheal bronchus
In tracheal bronchus the right upper
lobe is partially aerated by a bronchus that originates directly from the
supracarinal trachea.
Image
Incidental tracheal bronchus in a 28 y.o. male scanned for oncological
follow-up (axial image), and in a 2 y.o. male scanned for recurrent infections
(coronal image).

Cardiac bronchus
A cardiac bronchus is a truly supernumerary bronchus that originates opposite to the right upper lobe orifice on the medial side of the bronchus intermedius. It may aerate a small portion of parenchyma, or it may be a blind ending structure.
Patients are mostly asymptomatic, although recurrent infections may occur due to insufficient mucous clearance.
Image
Cardiac bronchus in a 57 y.o.
female in follow-up for interstitial lung disease.

Heterotaxy
A rare variant occurs in heterotaxy syndrome, where there is abnormal left-right orientation of anatomy which is neither normal situs solitus nor situs inversus.
In this context, isomerism describes mirrored anatomy, where in either right or left isomerism bronchial anatomy is similar on both sides.
Heterotaxy is often associated with congenital cardiac and other developmental abnormalities.
Image
Thick-slab MinIP (minimal intensity projection) in left isomerism in a
54 y.o. female with congenital heart disease, showing symmetrical bronchial
anatomy with ‘two left lungs.

Bronchial atresia
Interruption
of the bronchial tree is also possible, as is the case in bronchial atresia,
where a proximal segment of the bronchus is obliterated.
Bronchial
atresia may be found incidentally, or may be associated with symptoms of
coughing, dyspnea and sometimes recurrent infection.
Imaging typically shows a branching structure with surrounding lucent lung parenchyma, representing a dilated bronchus filled with mucus that is not connected to the bronchial tree with associated lung hyperinflation.
Images
Bronchial atresia in the left lower lobe in a 47 y.o. female.
Typical branching structure with surrounding lucent lung parenchyma, representing a dilated bronchus filled with mucus (arrow).
There was absence of the posterior basal segmental bronchus orifice
(LB10) and extensive hyperinflation of the associated lung parenchyma, best seen
on the lung reconstructions.
Continue with the next image...

The thick-slab MIP (maximum intensity projection) image shows the dilated and mucus filled airways in the left lower lobe (arrow).
Iatrogenic changes

Resection
Surgeons, bronchoscopists and radiotherapists
can all alter the anatomy of the lung.
Following the airways from trachea to the segmental
level on CT will prevent overlooking changes that are
not commented on in the clinical information, or point out exactly what part of
the lungs is involved in pathology present.
Knowledge of the normal bronchial anatomy is the key to identify what has
been resected, has been treated or is displaced.
Lobectomy and segmentectomy
For resection of focal pathology surgeons can choose between an
unanatomical wedge resection, an anatomical segmental resection, (bi)lobectomy
or pneumonectomy.
Following the airways towards the staple line will establish what has been done
and which part of the lung is resected.
In the postoperative status the residual lung tissue will fill the chest cavity
on that side, and may hyperinflate and displace. Additionally, mediastinal
shift and pleural effusions may occur in this process.
Tracing the airways that
are still present will help to correctly identify displaced lung tissue.
Images
Scroll through the images.
The upper lobe, intermediate and lower lobe bronchus continue towards the
periphery.
The bronchus for the middle lobe stops where the staples are placed.

Torsion
Tracing the airways will help to identify
displaced lung tissue.
These images are of a 65 y.o. female after previous right upper lobe lobectomy.
First scroll through the images.
Images
Tracing
the airways consecutively identifies the RUL lobectomy stump, the obliterated middle
lobe bronchus and the patent lower lobe bronchi.
This identifies the caudally
displaced lung tissue as the RML, which is best seen on the sagittal view.
The RML is edematous
and no longer perfused.
There is also some congestion and atelectasis seen in
the basal segments of the RLL, that now lay on top of the infarcted RML.

Segmental ischemia
Ischemia can also occur after
segmentectomy, when blood flow to the remaining segments is insufficient either
due to compression, kinking or otherwise.
Given the expected increase in number
of segmentectomies performed over the coming years, this is a complication that
will probably be encountered more often.
Therefore, familiarization with this
entity is important.
Images
Scroll through the images.
Tracing the airways of the left lower
lobe shows patency of the first segmental branch of the left lower lobe; the superior
segmental bronchus.
The staples are located at the location of the posterior
and lateral basal segments (LB9/10), which are most often resected together.
Therefore, the pulmonary segment that shows ground glass and consolidation must
be the anterior basal segment of the left lower lobe (LB8).
The pulmonary
artery towards this segment is also not opacified, and the iodine perfusion map
emphasizes the infarction.
The patient was re-operated and resection of the
infarcted segment was performed, with histopathological confirmation.
Continue with the perfusion map...

On the iodine perfusion there is perfusion in the left upper lobe and superior segment of the left lower lobe, but no perfusion of the anterior basal segment of the left lower lobe.

Endobronchial valves
A relatively
new procedure to treat people with severe emphysema is endoscopic lung volume
reduction (ELVR).
ELVR is a form of non-surgical lung volume reduction.
One-way
endobronchial valves are inserted into the segmental airways of the most affected
lung lobe.
These endobronchial valves gradually deflate the treated part of the
lung and allow the remainder of the lung to function more effectively.
Images
Endobronchial valves in the basal segmental bronchi of the right lower
lobe after endoscopic lung volume reduction.
Note that the procedure did not induce the intended lobar collaps, with hyperinflation
of the lower lobe still present (arrowheads).
It is assumed that this is due to collateral ventilation.

Chemoradiation
Oncologic
treatment can result in substantial architectural distortion which hinders
anatomical orientation.
Tracing the airways makes it easier to
identify post-treatment lung anatomy.
By doing so, miscommunication and
contradictions between radiology reports can be prevented.
Images
Extensive
architectural changes in the right hemithorax after chemoradiotherapy for stage 4 NSCLC.
Tracing the airways shows that the right upper lobe is largely aerated, while the bronchus intermedius is occluded and as a result both the right middle and lower lobe are collapsed.
Thrombo-embolic disease

The pulmonary arteries accompany the bronchi on their course towards the periphery and thus there are lobar, segmental and subsegmental branches.
Differentiation can be made by tracing the arterial divisions in correlation to the bronchi.
In acute PE it is mainly important to correctly differentiate segmental from subsegmental emboli, as anticoagulant treatment in solitary subsegmental PE is under debate.
Images
These images are of a 59 y.o female at the emergency department,
nicely showing emboli at different levels.
Scroll through the images.
- Thrombus in the lobar artery to the right upper lobe.
- Thrombus in the orifice of the posterior basal segmental artery of the right lower lobe.
- Subsegmental thrombus in the anterior basal segment of the right lower lobe, a few divisions beyond the segmental artery.
- Thrombus at the segmental bifurcation of the left upper lobe.
- Thrombus continuing towards the periphery in the subsegmental artery.

Chronic thrombo-embolic pulmonary hypertension
Correct anatomical labelling in
chronic PE is important, as interventional treatment options of chronic emboli
in patients with pulmonary hypertension (CTEPH) highly depends on anatomical
location.
Pulmonary endarterectomy targets central emboli, up to the segmental level.
Balloon pulmonary angioplasty targets more distal lesions.
Typically, chronic emboli represent
as wall adhering thrombus, webs or acute arterial caliber changes due to
proliferation and partial removal of prior emboli.
This in contrast to acute thromboembolic disease, which typically shows either strings
of embolic thrombus at vascular bifurcations or occluding thrombus but with
preservation of arterial caliber.
Image
Wall adhering thrombus in the left main pulmonary in a patient with chronic
thrombo-embolic disease.

Thick-slab MIP images of a 70 year-old male with chronic thrombo-embolic disease with pulmonary hypertension (CTEPH).
Image
There is an acute-on-chronic
occlusive segmental thrombus in the anterior segment of the left upper lobe
(black arrow).
Pre-existent segmental occlusion in of the basal
branches with acute tapering of the peripheral vessels (blue arrow).

These images are of a 53 y.o. male with pulmonary hypertension.
Images
- Bilateral segmental webs (black arrows)
- Segmental web with acute subsegmental arterial tapering distal to it (yellow arrow).
- MIP image showing bilateral segmental webs with acute subsegmental arterial tapering distal to it (arrowheads)
Conclusion
Bilateral segmental webs, with distal subsegmental arterial tapering,
consistent with chronic thrombo-embolic pulmonary hypertension (CTEPH).

Charity
All the profits of the Radiology Assistant go to Medical Action Myanmar which is run by Dr. Nini Tun and Dr. Frank Smithuis sr, who is a professor at Oxford university and happens to be the brother of Robin Smithuis.
Click here to watch the video of Medical Action Myanmar and if you like the Radiology Assistant, please support Medical Action Myanmar with a small gift.