TI-RADS - Thyroid Imaging Reporting and Data System
Habib Ahmad and Aad van der Lugt
Radiology department of the Erasmus Medical Center in Rotterdam
Up to 67% of individuals undergoing ultrasound evaluation are found to have incidental thyroid nodules.
The high prevalence of thyroid nodules, combined with the typically indolent progression of thyroid cancer, poses a significant challenge to the optimization of patient management.
The American College of Radiology (ACR) Thyroid Imaging Reporting and Data System (TI-RADS), introduced in 2017, was developed to reduce unnecessary biopsies of benign nodules and enhance diagnostic precision.
TI-RADS categories
 Click to enlarge
Click to enlarge
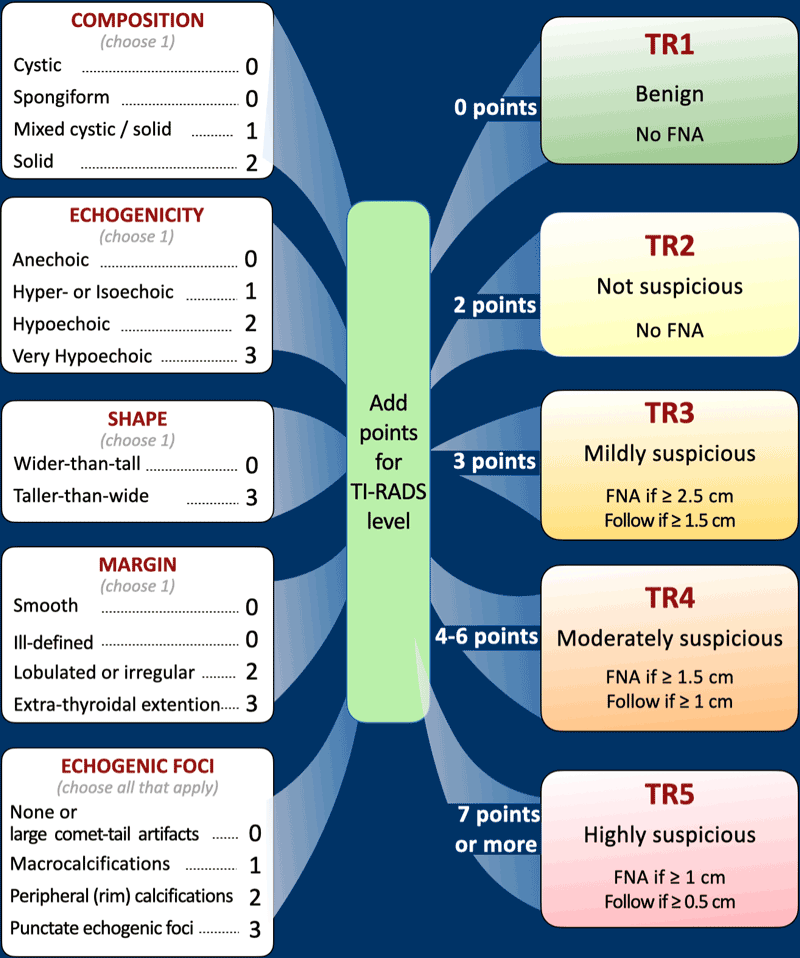
TI-RADS evaluates thyroid nodules based on five ultrasonographic features:
- composition
- echogenicity
- shape
- margin
- punctate echogenic foci.
Each feature is assigned a specific point value.
The cumulative score from all categories determines the TI-RADS level, which corresponds to a management recommendation.
Nodules measuring less than 5 mm require no follow-up, even if classified as TI-RADS 5, due to the exceedingly low likelihood of clinically significant malignancy at this size.
The 2.5 cm threshold for fine-needle aspiration (FNA) in mildly suspicious (TR3) lesions is supported by evidence indicating that survival rates in thyroid carcinoma are not compromised until tumors reach this size.
Large-scale studies have demonstrated a strong correlation between the ACR-TI-RADS classification and malignancy risk.
The risk of malignancy is:
- TR1: 0.3%
- TR2: 1.5%
- TR3: 4.8%
- TR4: 9.1%
- TR5: 35%
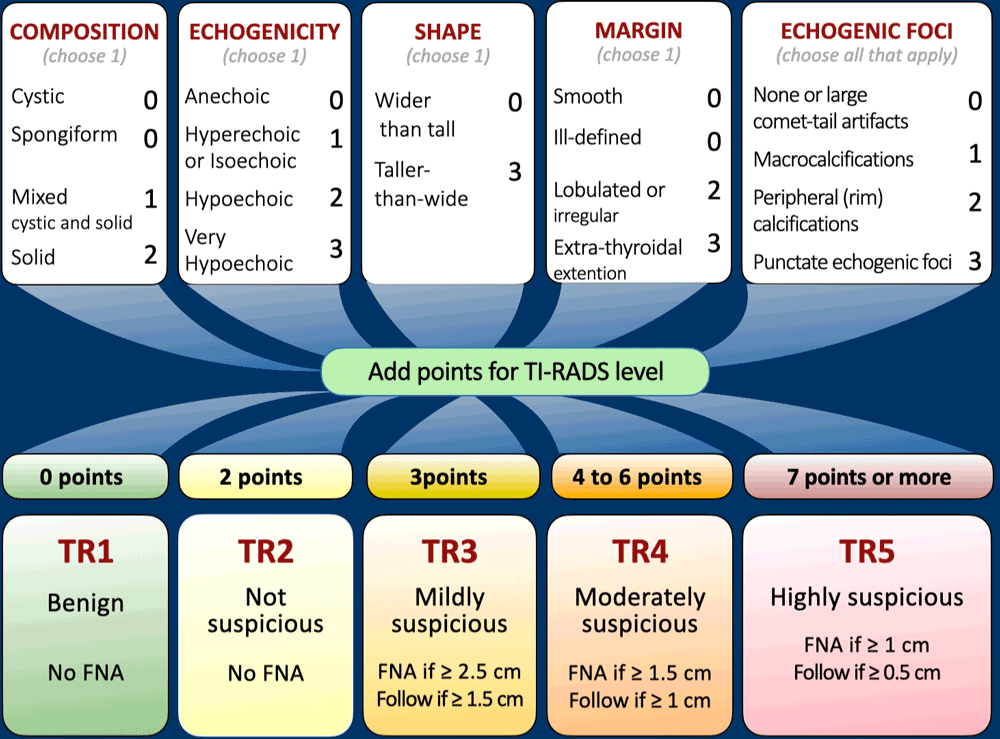
This table presents a horizontal version of the TI-RADS classification.
For a more detailed view, click to enlarge the image.
Exceptions to TI-RADS
The TI-RADS system is not applicable in several clinical scenarios, each of which carries a higher risk of thyroid cancer compared to the general adult population:
- Pediatric patients
- FDG-PET-avid thyroid nodules
- Presence of lymphadenopathy
- Known risk factors for thyroid malignancy, such as Multiple Endocrine Neoplasia (MEN) type 2
Composition

Cystic lesions, or those that are almost entirely cystic, are considered benign and are classified as TI-RADS 1.
No additional points are assigned. This also applies to spongiform nodules, which are inherently benign and do not require further ultrasonographic characterization.
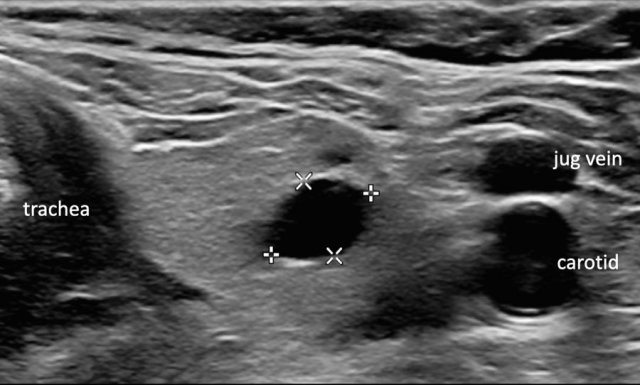
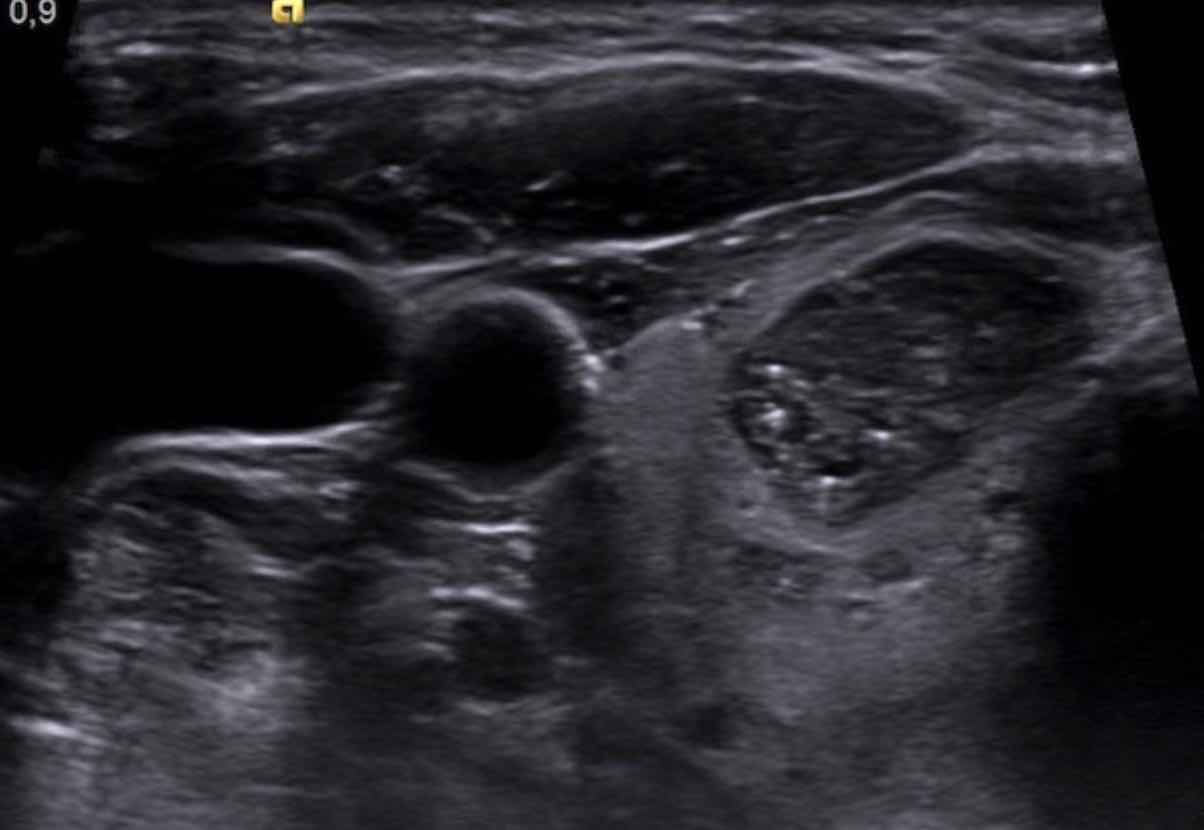
Cyst
The image depicts a typical thyroid cyst.
No further evaluation is necessary.
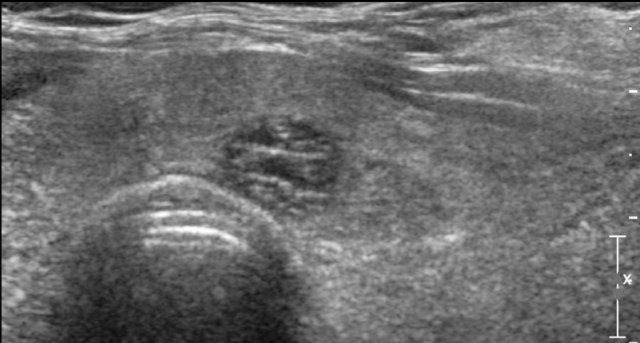
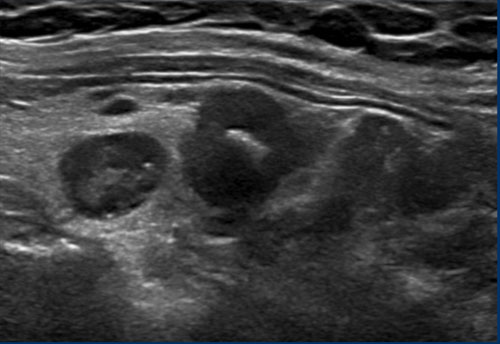
Spongiform nodules
Spongiform nodules exhibit a sponge-like appearance, with at least 50% of their composition consisting of tiny cystic components.
No further ultrasonographic characterization is required.

Mixed cystic/solid lesions
In mixed cystic/solid lesions, the proportion of cystic to solid components is not a determining factor.
These lesions receive 1 point for their mixed cystic/solid composition.
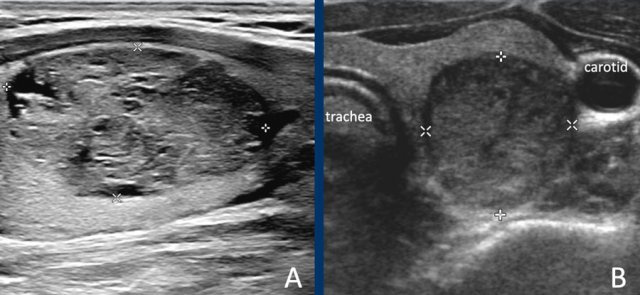
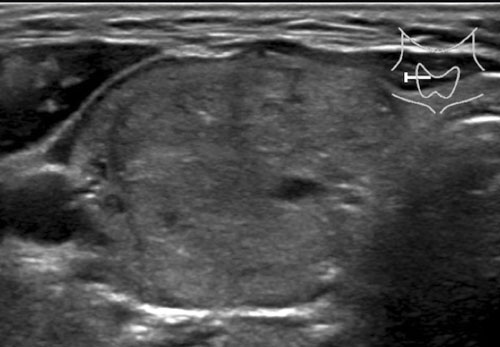
Solid lesions
- Lesion A: This lesion is almost entirely solid. Although small cystic areas are present, it does not meet the criteria for a spongiform nodule, as the cystic components constitute far less than 50% of the total nodule volume.
- Lesion B: This lesion is completely solid.
For a lesion to be classified as solid, at least 95% of its composition should be solid. This determination is based on visual estimation; precise calculation is not required.
Echogenicity

Anechoic Lesions
An anechoico lesion should appear completely black on ultrasound, indicating a cystic nature.
No further ultrasonographic characterization is required.
Hyperechoic and Isoechoic Lesions
Both hyperechoic and isoechoic lesions are assigned 1 point in the TI-RADS scoring system. For scoring purposes, there is no distinction between the two.
Echogenicity is assessed in comparison to normal thyroid parenchyma.
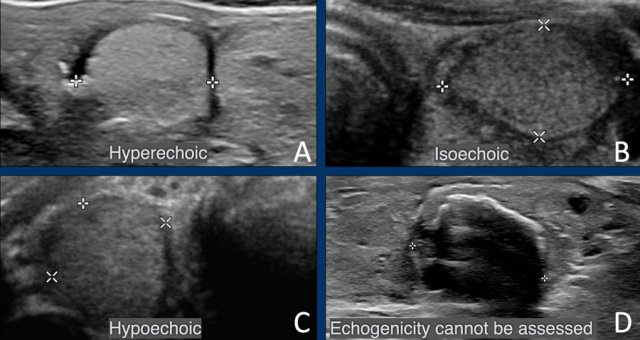
Hypoechoic Lesions
A hypoechoic lesion exhibits lower echogenicity than the surrounding normal thyroid parenchyma.
If echogenicity cannot be accurately assessed (e.g., due to the presence of calcifications), 1 point is assigned by default.
 Very hypoechoic , i.e. 3 points in TI-RADS.
Very hypoechoic , i.e. 3 points in TI-RADS.
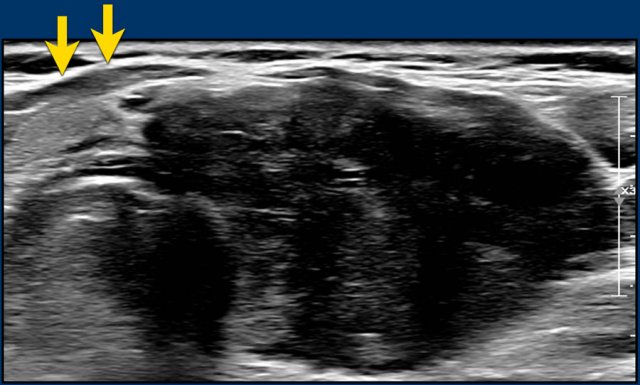
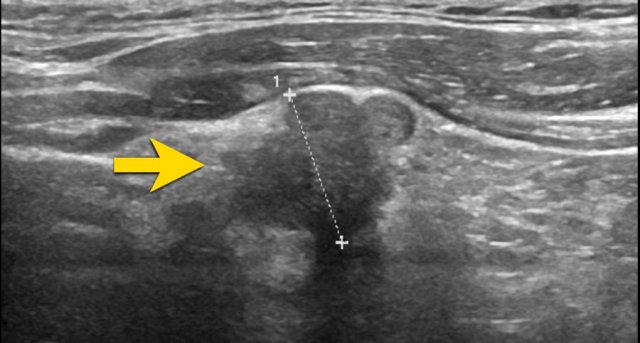
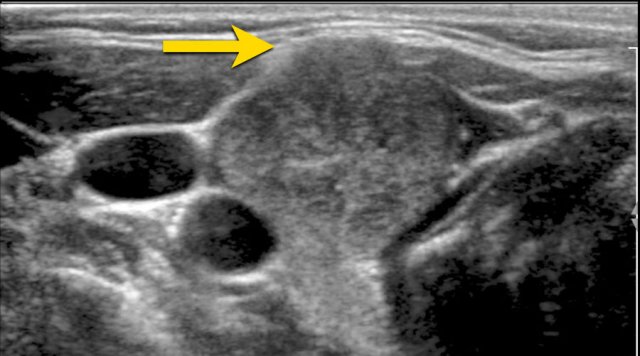
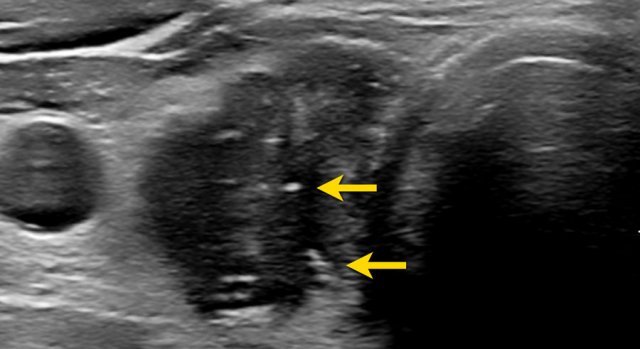
Markedly Hypoechoic Lesions
A markedly hypoechoic lesion demonstrates even lower echogenicity than normal muscle tissue.
Note that, in the provided image, the lesion is more hypoechoic compared to the strap muscles (indicated by arrows).
Shape
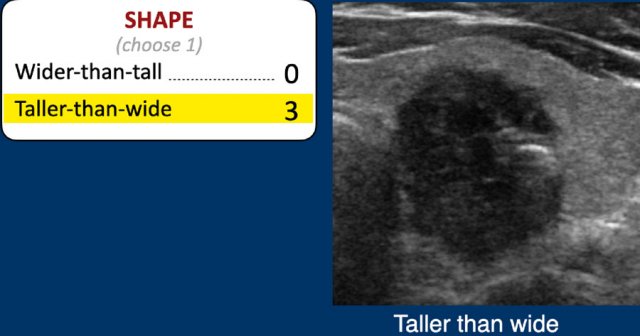
The shape should be assesed in the axial plane.
A taller-than-wide shape is a strong predictor of malignancy, and therefore gets 3 points.
Margin
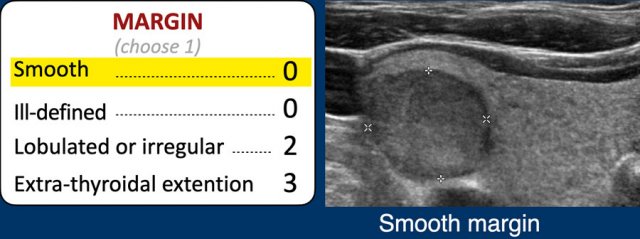
Assessment of Nodule Margins
The margin of a thyroid nodule is often best evaluated on the anterior aspect.
- Smooth: The margin is entirely smooth.
- Ill-defined: The margins of the nodule cannot be clearly distinguished from the surrounding thyroid parenchyma. This is considered a benign feature and should not be confused with an irregular margin.
- Lobulated or Irregular: Margins appear lobulated, spiculated, irregular, or angulated.
- Extrathyroidal Extension: This is challenging to assess on ultrasound. Clear invasion of adjacent structures must be evident; mere bulging into nearby structures is insufficient to classify as extrathyroidal extension.
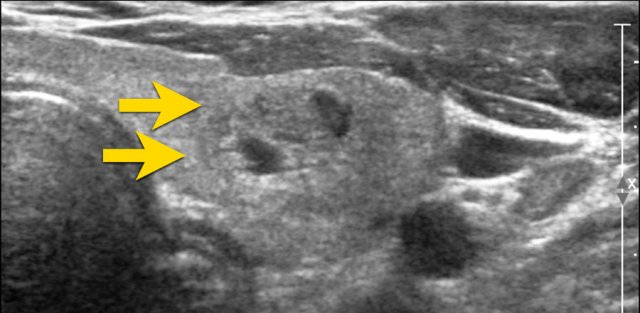
Ill-defined Nodule
In the provided image, only small segments of the nodule's border are discernible (indicated by the arrows).
The majority of the margin is indistinct from the thyroid parenchyma.
TI-RADS Score: 0 points.
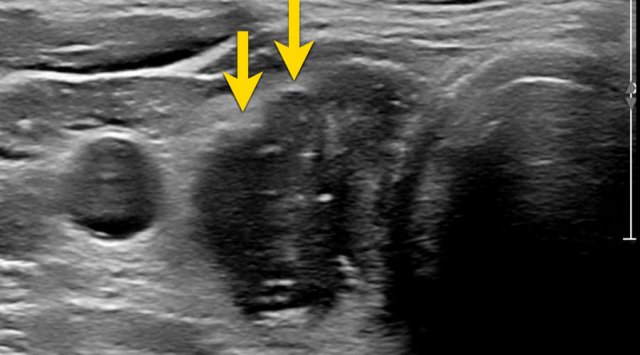
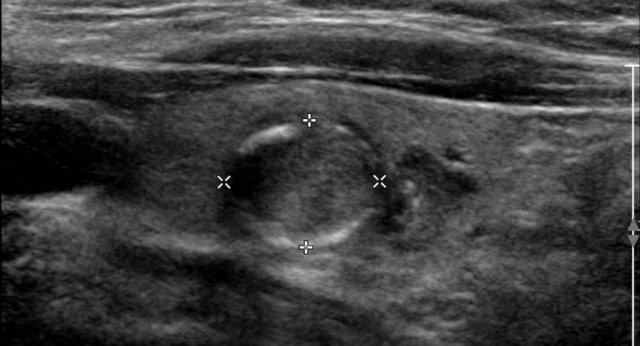
Nodule with Irregular, Angulated Margins
This nodule exhibits irregular, angulated margins.
TI-RADS Score: 2 points.
Nodule with Irregular, Lobulated Margin
The image demonstrates an irregular, lobulated margin on the anterior surface of the nodule.
TI-RADS Score: 2 points.
 Exophytic growth but no frank invasion.
Exophytic growth but no frank invasion.
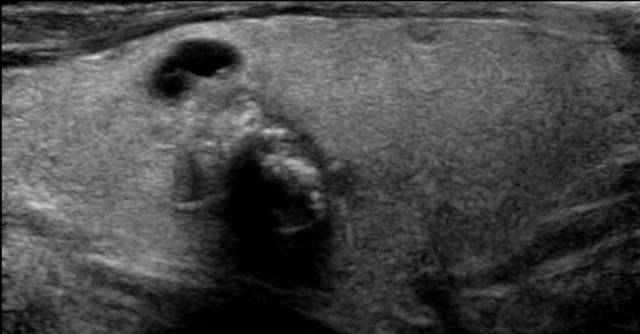
Nodule with Exophytic Growth
This nodule shows exophytic growth with compression of adjacent structures.
However, there is no definitive evidence of frank invasion, and thus, it does not qualify as extrathyroidal extension.
Echogenic foci
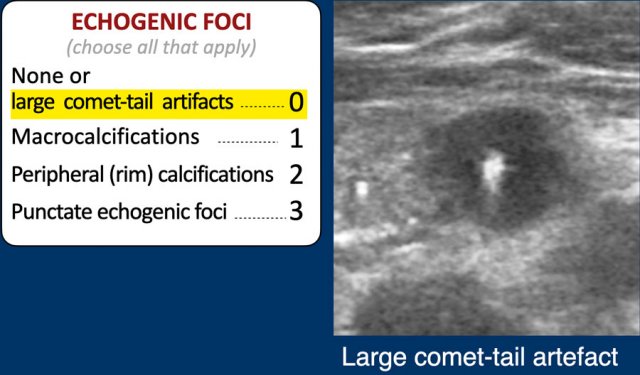
Comet Tail Artifact and Echogenic Foci
The echogenic foci category is unique in that multiple features may apply simultaneously, and all relevant options must be selected.
Points for each applicable feature are added to the total TI-RADS score.
For example, if both punctate echogenic foci and rim calcifications are present, the total TI-RADS points would be 3 + 2 = 5 points.
0 Points is assigned for:
- Absence of echogenic foci.
- Large comet tail artifacts (>1 mm), as illustrated in the figure.
Macrocalcification
This nodule exhibits large macrocalcifications with associated acoustic shadowing.
TI-RADS Score: 1 point.
Rim calcification
Peripheral rim calcifications may be either complete or incomplete.
TI-RADS Score: 2 points.
Microcalcifications
Punctate echogenic foci, also referred to as microcalcifications, are a strong predictor of malignancy and are assigned 3 points in the TI-RADS system.
The American College of Radiology (ACR) lexicon further refines this category, as echogenic foci may also be visible in normal thyroid tissue.
Punctate echogenic foci should only be classified as such when they are clearly identifiable and confined within the nodule.

Additionally, small comet tail artifacts with a length of less than 1 mm are included in the category of microcalcifications.
TI-RADS Score: 3 points.
Growth
Nodule Growth According to TI-RADS and ATA Guidelines
Growth of a thyroid nodule, as defined by TI-RADS, aligns with the American Thyroid Association (ATA) guidelines. Significant growth is indicated by either:
- A ≥20% increase in at least two nodule dimensions, with a minimum increase of 2 mm, or
- A ≥50% increase in volume.
If a nodule demonstrates no change in size over a 5-year period, it can be considered benign in behavior, and no further follow-up is required. Size comparisons should be made with the oldest available imaging study, not solely the most recent one. If interval growth occurs but does not meet FNA criteria, the next follow-up should be scheduled after 1 year, regardless of the TI-RADS category.
Multiple Nodules
Management of Multiple Nodules
When multiple nodules are present, no more than four nodules should be classified, and FNA is not recommended for more than two nodules.
In cases of multiple nodules, the nodule meeting TI-RADS FNA criteria should be sampled, which is not necessarily the dominant or largest nodule.
Overdiagnosis and Overtreatment
Clinical Significance of Thyroid Nodules
Once a thyroid nodule is detected, the primary diagnostic question is whether it is benign or malignant.
Depending on the referenced series, 6%–13% of thyroid nodules selected for FNA will prove malignant.
The majority of incidentally detected thyroid cancers are of papillary origin, which, unlike anaplastic thyroid cancer (responsible for over half of thyroid cancer deaths despite comprising only 1%–2% of cases), is typically indolent.
Given that papillary thyroid cancer is the most common and well-differentiated subtype, its prognosis is excellent, with a 30-year survival rate of 95%.
However, many of these cancers would likely remain asymptomatic during a patient’s lifetime, raising concerns about overdiagnosis.
Research efforts should focus on identifying the small subset of thyroid cancers that are aggressive and impact survival.
Examples
Composition
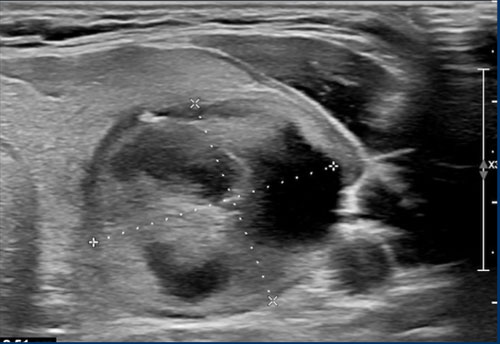
Case 1
Examine the image and assign a TI-RADS score.
Scroll the image to view the TI-RADS score.
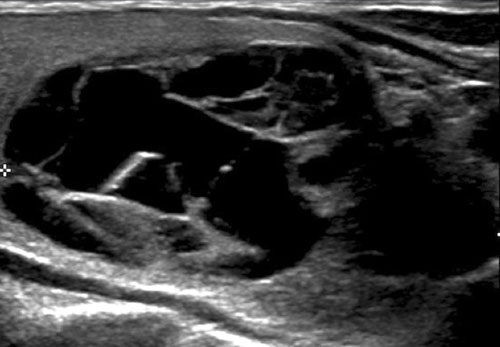
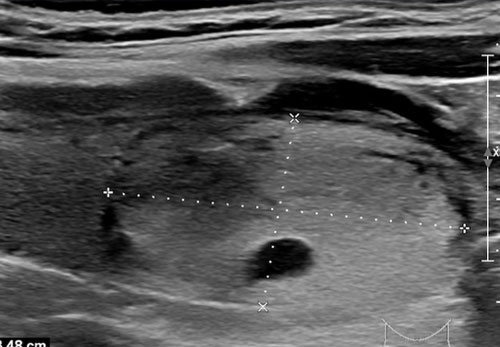
This nodule exhibits a mixed composition, with a cystic component centrally located.
Case 2
Examine the image and assign a TI-RADS score.
Scroll the image to view the TI-RADS score.
Case 3
Examine the image and assign a TI-RADS score.
Scroll the image to view the TI-RADS score.
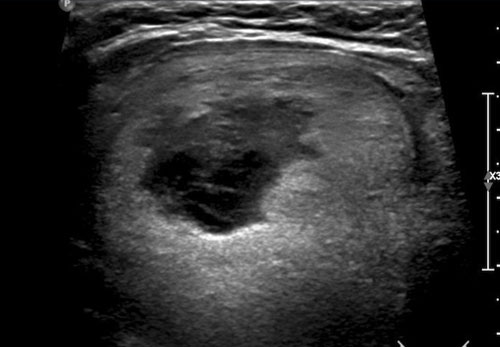
Case 4
Examine the image and assign a TI-RADS score.
Scroll the image to view the TI-RADS score.
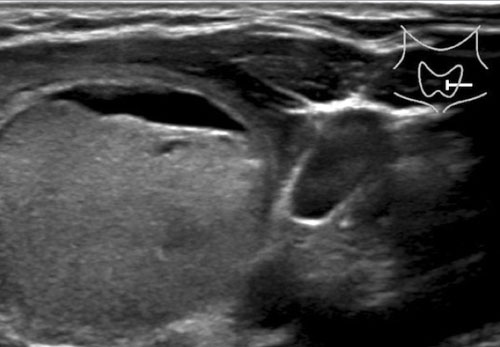
This nodule is predominantly solid.
The cystic component is minimal, warranting 2 points for composition.
Echogenicity
Case 1
First, examine the ultrasound image.
Proceed with the analysis below.
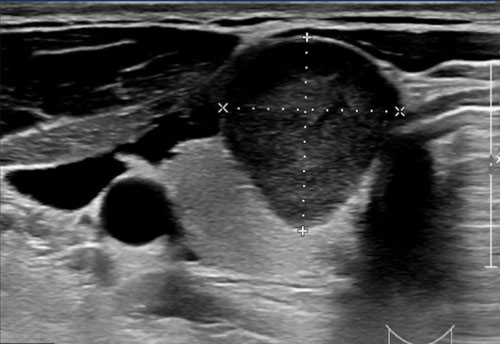
There is posterior acoustic enhancement, suggesting that this lesion may be cystic.
In such cases, color Doppler imaging can be useful for further evaluation; however, it was not performed in this instance.
Case 2
Examine the image and assign a TI-RADS score.
Scroll the image to view the TI-RADS score.
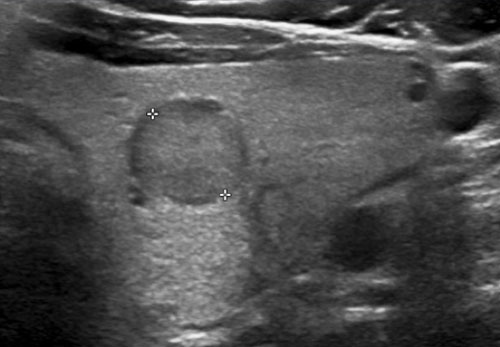
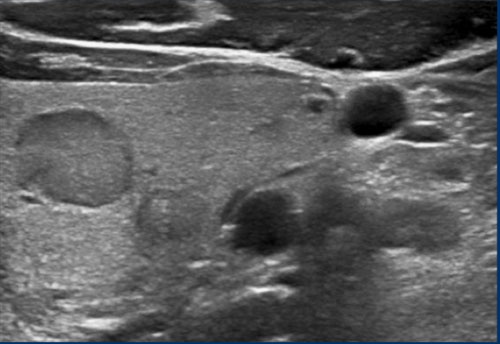
This nodule is hypoechoic relative to the normal thyroid tissue visible on the ventral aspect of the nodule.
TI-RADS Score: 2 points for hypoechoic echogenicity.
Case 3
Examine the image and assign a TI-RADS score.
Scroll the image to view the TI-RADS score.
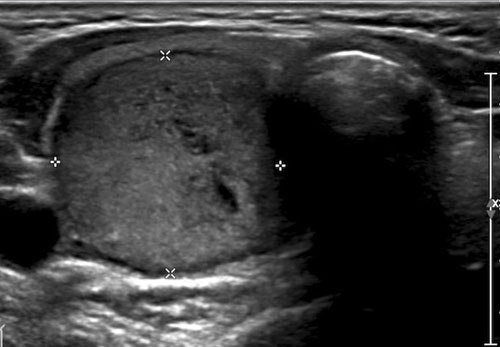
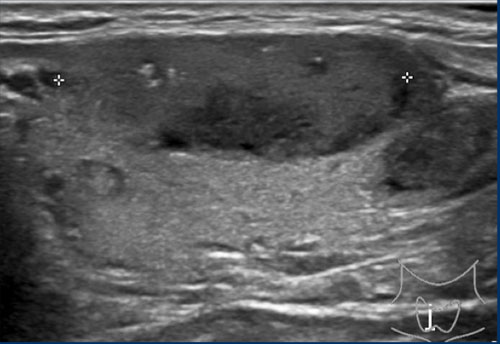
This is a hyperechoic nodule.
TI-RADS Score: 1 point for echogenicity.
Shape
Case
Examine the image and assign a TI-RADS score.
Scroll the image to view the TI-RADS score.
TI-RADS Score: 3 points for a taller-than-wide shape.
Margin
Case 1
Examine the image and assign a TI-RADS score.
Scroll the image to view the TI-RADS score.
Examine the image and assign a TI-RADS score.
Scroll the image to view the TI-RADS score.
Proceed with the analysis below.
Although the margin is ill-defined on the cranial aspect, this still results in 0 points for the margin.
Echogenic foci
Case 1
Examine the image and assign a TI-RADS score.
Scroll the image to view the TI-RADS score.
Case 2
Examine the image and assign a TI-RADS score.
Scroll the image to view the TI-RADS score.
Proceed with the analysis below.
TI-RADS Score: 1 point for the presence of macrocalcification.
This lesion is classified as TI-RADS 5, primarily due to its markedly hypoechoic echogenicity.
If the lesion is also taller than wide, this would contribute an additional 3 points.
Case 3
Examine the image and assign a TI-RADS score.
Scroll the image to view the TI-RADS score.
Note the subtle echogenic foci present.
A total of 6 points corresponds to a TI-RADS score of 4.