Breast Implants
Normal imaging findings and complications
Esteban van Keulen, Saskia Fuchs, Maud Hegeman and Robin Smithuis
Department of Radiology of the Tergooi MC hospital in Hilversum, University Medical Center Utrecht and the Alrijne hospital in Leiderdorp, the Netherlands
Publicationdate
Breast augmentation surgery is the most popular cosmetic surgery procedure worldwide.
The number of women who have breast implants for augmentation or reconstruction is increasing.
The risk of rupture increases with the age of the implant and is seen more often in reconstruction after mastectomy for breast cancer than in implants for cosmetic augmentation.
In this review we will focus on the role of imaging in describing normal and abnormal findings of common implants.
This review is based on a presentation given by Saskia Fuchs, Esteban van Keulen en Maud Hegeman during the Sandwich course of the Radiological Society of the Netherlands in februari 2021.
Introduction
Location and type of implant
About 80% of breast implants are for cosmetic augmentation, while about 20% are for breast reconstruction following mastectomy.
Breast implants consist of a silicone outer envelope and a silicone or saline filling.
Capsule
All breast implants will become encapsulated. This can start within weeks to years after implantation.
It is a physiological foreign body reaction of fibrous tissue that will form around the implant.
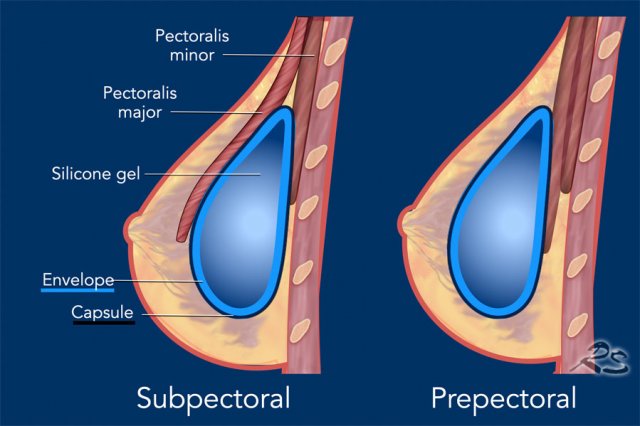
Breast implants are placed:
- Subpectoral (retropectoral) between pectoralis major and minor muscles or
- Prepectoral (sub- or retroglandular) anterior to the pectoralis major muscle or
- Dual plane - a combination of both - most of the implant is subpectoral, but the inferolateral part is not covered by muscle.
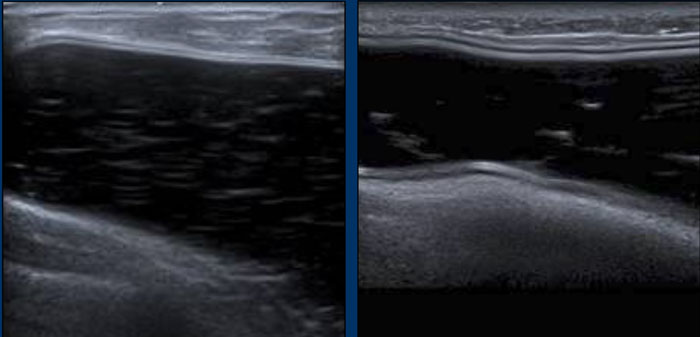
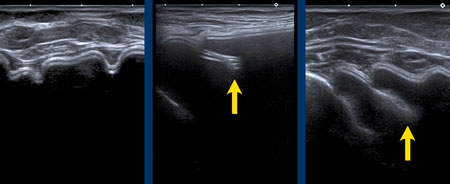
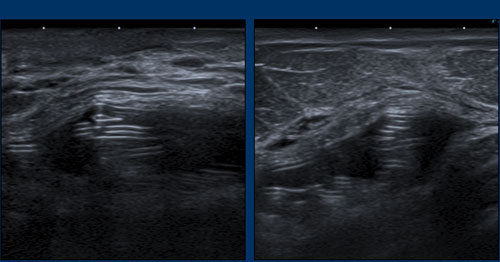
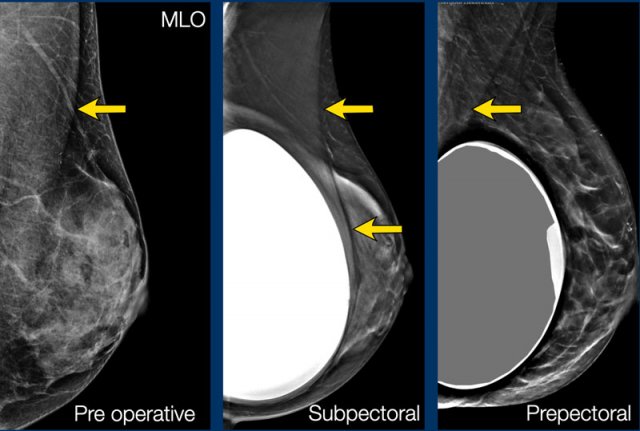 Arros indicate the pectoral muscle
Arros indicate the pectoral muscle
Subpectoral implant
In this technique, the pectoralis major muscle is elevated from the chest wall.
Palpability
of the edges of the implant will be lower in general.
Mammograms are usually less distorted compared to the prepectoral group.
Prepectoral implant
In the prepectoral technique, the implant is placed in front of the pectoral muscle posterior to the glandular tissue.
Rippling is observed as the most common complication.
Mammograms are somewhat more distorted.
The location of the implant in relation to the pectoral muscle is best recognized on the oblique views.
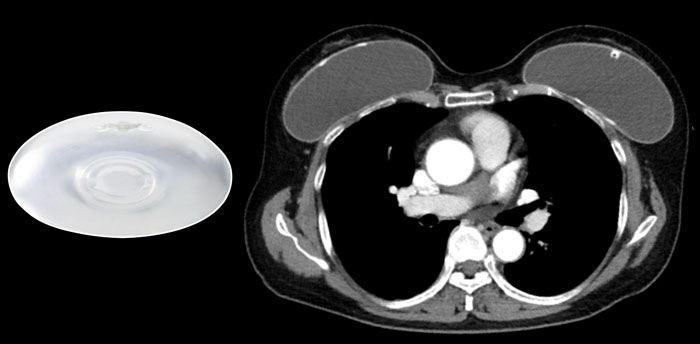
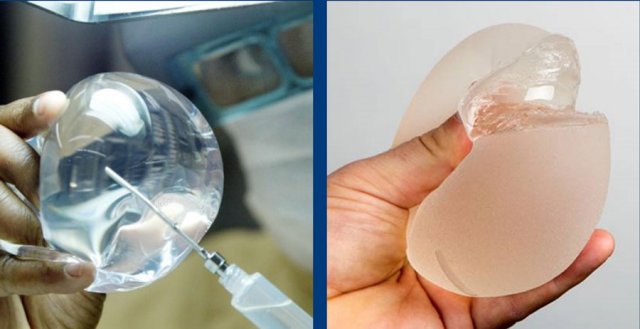 Saline filled implant and a silicone filled implant which is cut to show the form-stable content.
Saline filled implant and a silicone filled implant which is cut to show the form-stable content.
Silicone filled implants
The most used breast implants consists of an outer silicone elastomer envelope and an inner filling of silicone gel.
The silicone filling has evaluated over the years into a more form-stable mass (figure).
Saline filled implants
Saline filled implants also have a silicone outer envelope. They
can be primarily used for cosmetic augmentation or
used
as breast tissue expanders in reconstructive surgery as a temporary device and gradually filled with saline. Saline filled implants are more prone to trauma
resulting in immediate deflation.
Breast implants may be round or anatomically pre-shaped.
The surface of the envelope can be smooth or textured including a polyurethane covering to prevent the implant from turning.
Some implants have a patch, which is a textured area on its surface to keep the implant in place or as a palpable orientation mark for the surgeon.
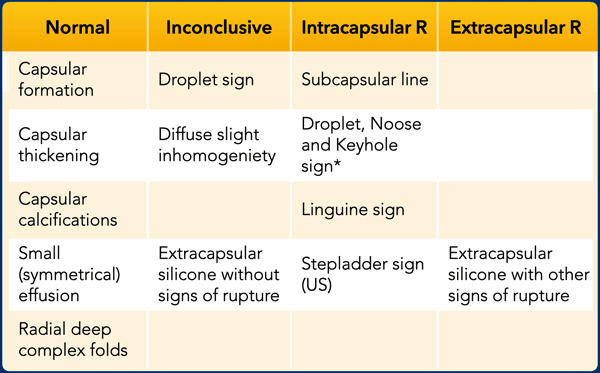 * Must be considered as an uncertain finding if it is only seen as a single sign on a single image (which is uncommon).
* Must be considered as an uncertain finding if it is only seen as a single sign on a single image (which is uncommon).
Imaging findings
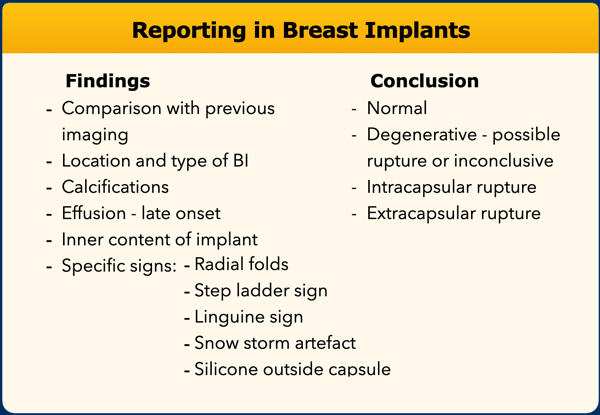
This table summarizes normal and abnormal findings in breast implants.
When the droplet-, noose- or keyhole sign is seen as a single sign on a single image, which is uncommon, then it must be considered as an uncertain finding.
The Linguine sign is most specific for intracapsular rupture.
Normal findings
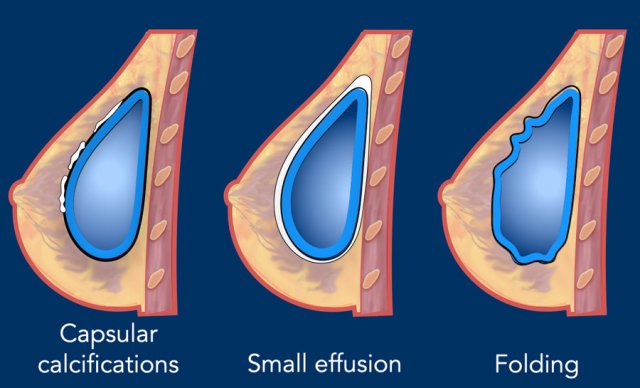
Capsular calcifications
Calcifications can be found in about 25% of the breast implants. The incidence of capsular calcifications increases with age of implants. These calcifications do not indicate rupture, although associated with some degeneration of the envelope.
Effusion
A
small amount of periprosthetic fluid is frequently seen and is almost always normal.
However
it still can be a seroma, hematoma or infection and must be correlated to
clinical symptoms. There is no absolute diameter that should be interpreted as
abnormal. Comparing
with the contralateral implant can be helpful.
Folding
Palpable folds can occur especially in prepectoral implants with a superficial location in women with few surrounding tissue. These folds can be impressed and pop back at physical examination. Folding is a normal finding.
 Capsular calcifications. Possible intracapsular rupture of the breast implant on the right.
Capsular calcifications. Possible intracapsular rupture of the breast implant on the right.
On this axial CT-image there is capsular thickening with severe capsular calcifications.
On the right side there also is an irregular content and some linear lines, which is suspicious for intracapsular rupture.
Degenerative changes
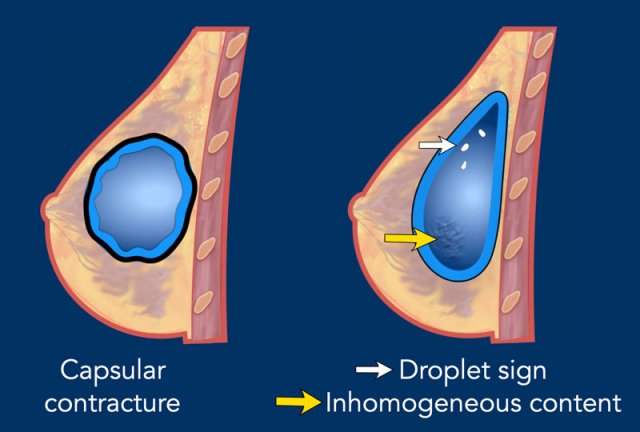
Capsular contraction
The incidence of contraction of the capsule is up to 25% in 10 years and is seen more often in breast reconstruction than in cosmetic breast augmentation. The capsule will become thick and hardens, the implant shape will usually become rounder and less compressible.
Droplet sign
The droplet sign and inhomogeneous content are degenerative changes that may indicate intracapsular rupture, but are not definitive proof of rupture.
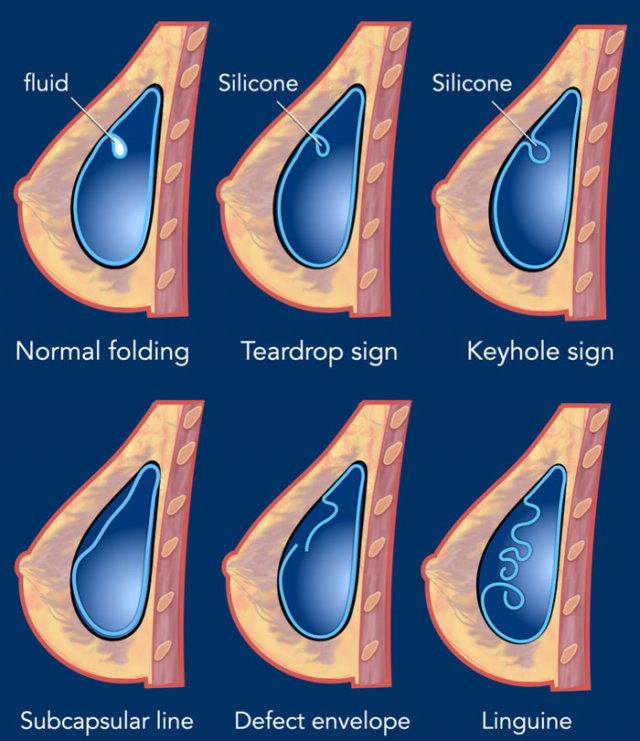
Intracapsular rupture
An intracapsular rupture occurs when the shell of the implant ruptures but the fibrous capsule formed by the breast remains intact.
Silicone does not freely extravasate, but is stuck between the capsule and the envelope.
This makes it difficult to detect on clinical exam or mammography. There are many signs described that indicate intracapsular rupture, but it all comes down to silicone between the capsule and the envelope.
Intracapsular rupture is best seen on MRI.
Teardrop sign
It is a focal invagination of the silicone envelope where the two walls do touch. A small amount of silicone is within the teardrop, which means that it is outside the envelope.
Keyhole sign
Also known as nose-sign. It is a focal invagination of the silicone envelope where the two walls do not touch. A small amount of silicone is within the keyhole and outside the envelope.
Linguine sign
The ruptured envelope appears as curvilinear lines that look like Linguine pasta.
These signs of intracapsular rupture need to be differentiated from normal folding which may contain some fluid, which is normal periprosthetic fluid (figure).
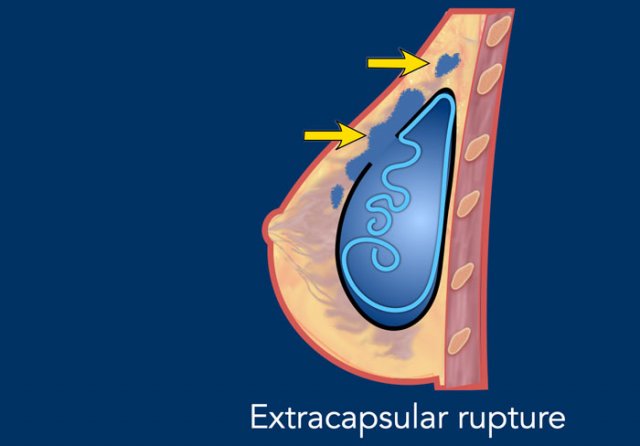
Extracapsular rupture
In extracapsular rupture the silicone from the ruptured implant migrates freely beyond the envelope and the fibrous capsule into the surrounding breast tissue.
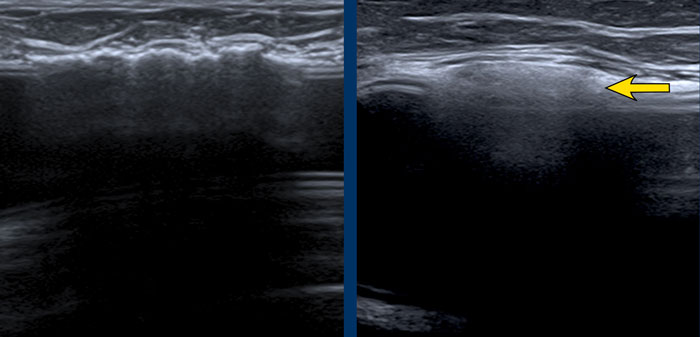
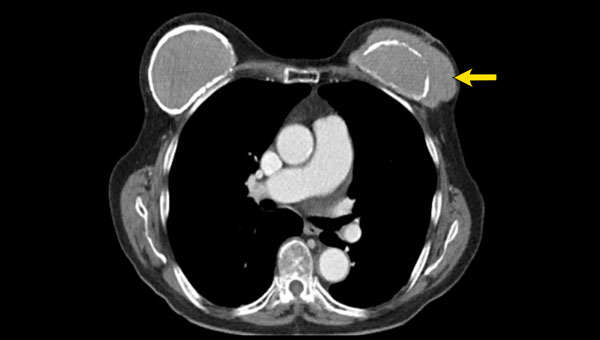
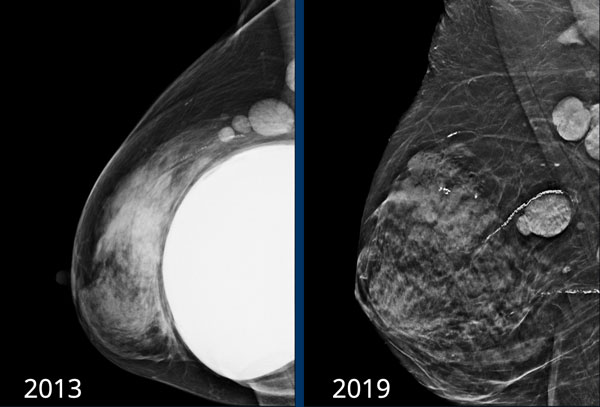
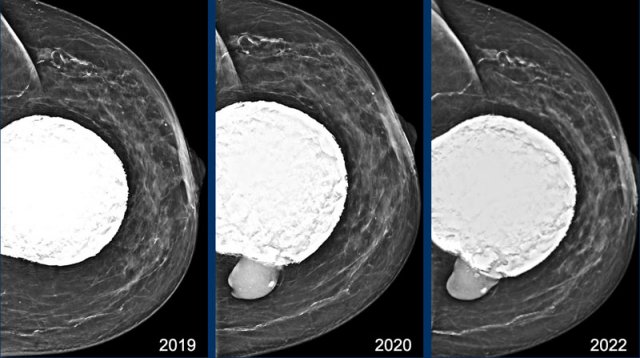 Capsular calcifications and extracapsular rupture (arrow)
Capsular calcifications and extracapsular rupture (arrow)
In 2019 the mammogram shows extensive capsular calcifications and a very round shape of the breast implant.
This indicates a contracture of the implant.
At follow up in 2020 the contour has changed and now there is silicone beyond the capsule, which is a definitive sign of extracapsular rupture (arrow).
This elderly patient did not not want surgery, but only wanted screening for possible malignancy.
In 2022 at follow up exam not much has changed. Modern Silicone gel is more cohesive and has less tendency to spread.
Reporting
When you examine the patient with ultrasound, mention the degree of evaluability.
The condition of the implant can be obscured by capsular calcifications or the posterior border can be hard to see in big volume of implant.
No Bi-Rads classification in the MRI report as the protocol is not able to detect breastcancer.
Ultrasound
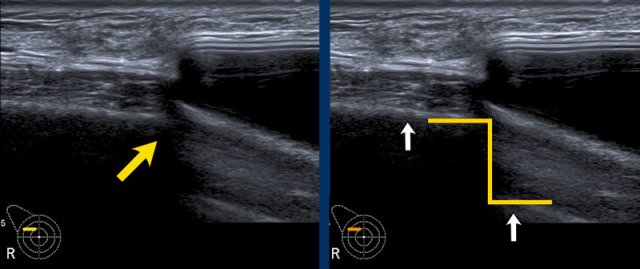
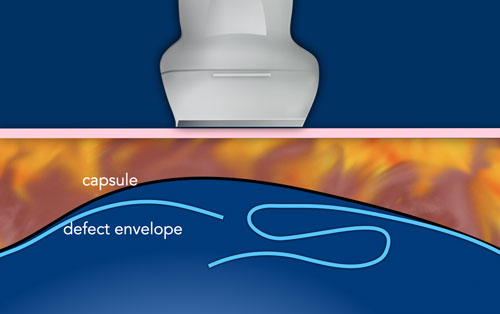
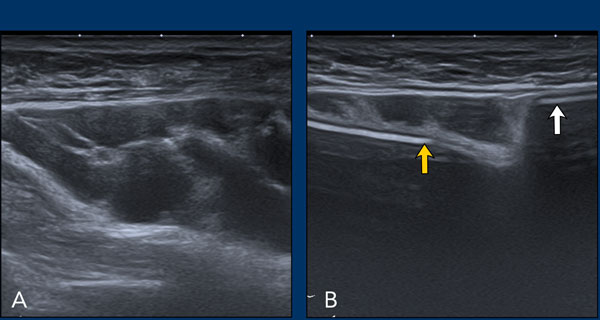
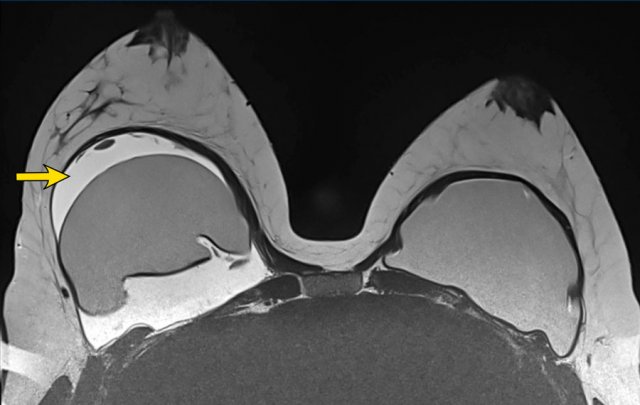
 Envelope (yellow arrow) and capsule (white arrow) anterior to the envelope
Envelope (yellow arrow) and capsule (white arrow) anterior to the envelope
Normal findings
Inverted Oreo sign
The envelope of the prosthesis can be seen as an inverted Oreo cookie. The first white line is the outer interface of the envelope and the second white line is the inner interface between the envelope and the Silicone gel (yellow arrow).
In between the outer layer of the envelope and the surrounding capsule there is a virtual space that can fill and broaden.
The capsule is seen apart from the envelope as a separate white line anterior to the envelope (white arrow).
Envelope and capsule together are called envelope-capsule complex.
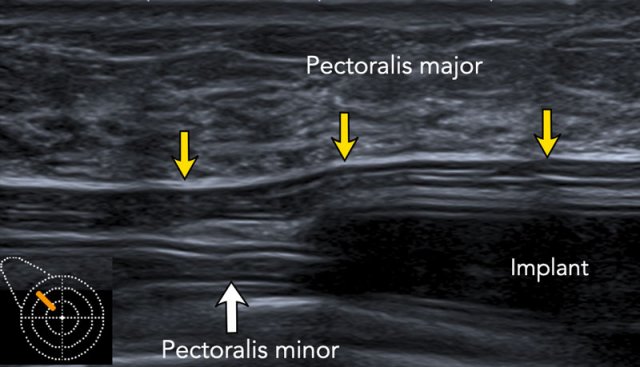
The location of breast implant is best evaluated in the upper lateral quadrant. Look for the pectoralis muscle in relation to the implant.
The lower part of implant is usually not completely covered by the pectoralis muscle.
Image
This is a breast implant in subpectoral position.
The pectoralis major is seen anteriorly to the implant.
More caudally the major pectoralis muscle thins and will be more difficult to see.
 Step off sign in silicone prosthesis
Step off sign in silicone prosthesis
Step off sign
The step off sign is an artefact caused by a lower transmission speed of the ultrasound waves through Silicone ( 970m/sec in Silicone gel and 1540m/sec through water).
As a result the chest wall seems to be deeper at the level of the prosthesis.
This artefact is not seen in saline filled implants.
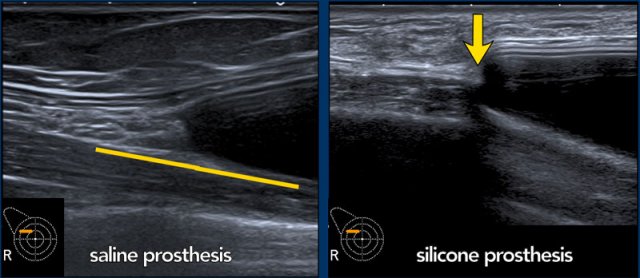
Here you can see the difference between a saline and a silicone prosthesis.
 Capsular calcifications
Capsular calcifications
Capsular calcifications
Capsular calcifications can be single or multiple.
Sometimes they are linear or diffuse and thick.
 Reverberation artefacts
Reverberation artefacts
Reverberation artefacts
In the anterior area of the prosthesis frequently parallel horizontal echogenic lines can be seen caused by reverberation artefacts.
These artefacts can be reduced by using less pressure with the transducer or by using harmonic imaging.
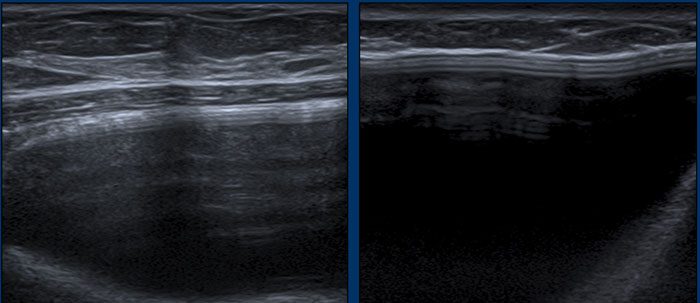
 Normal inhomogeneous aspect postoperative
Normal inhomogeneous aspect postoperative
Diffuse somewhat inhomogeneous internal aspect of BI can be seen, also short after operation. So this aspect without other signs of complications does not indicate definite intracapsular rupture.
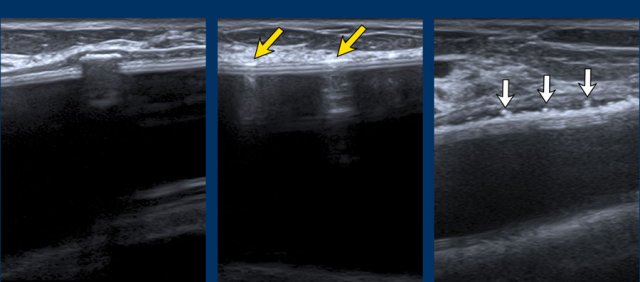
 Capsular calcifications versus extracapsular leakage of Silicone.
Capsular calcifications versus extracapsular leakage of Silicone.
Sometimes when there is a thick layer of calcifications it may mimic the snowstorm artefact, which is caused by extravasated silicone gel.
Images
On the left intense calcifications.
On the right snowstorm artefact caused by extracapsular leakage of silicone gel.
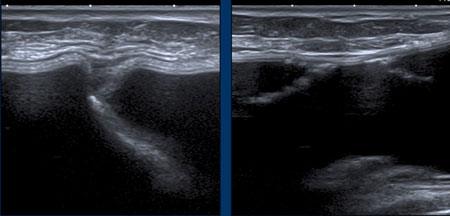
 Different types of valves
Different types of valves
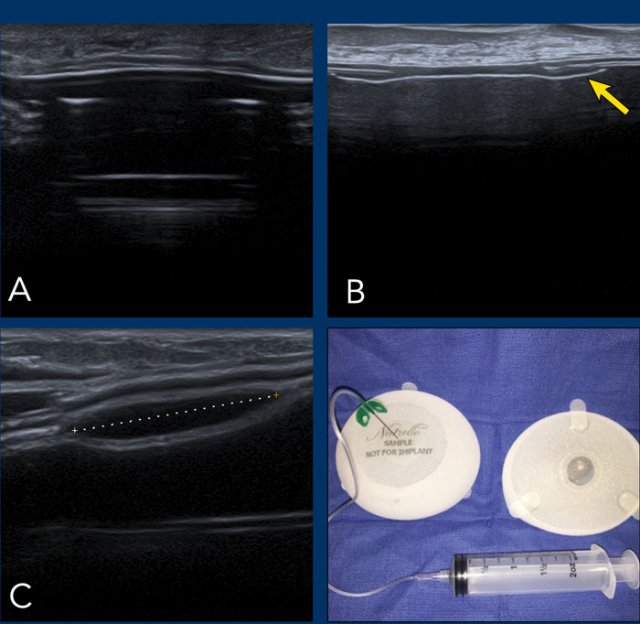
Images
A. Saline implant with a fill valve
B. Symmetrical sharp deliniated and centrally located diaphragm that simulates an atypical appearance of the envelope.
C. Different type of reservoir.
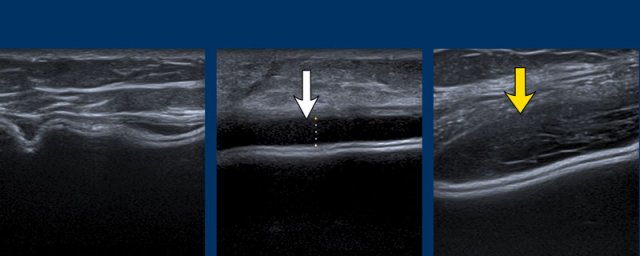
 Band-like marking on a breast implant
Band-like marking on a breast implant
Markings
Mammography showing a breast implant with a small circular band.
On ultrasound it is recognized as a linear structure by looking in two planes (circle on axial scan and arrows on sagittal scan).
It should not be confused with a problem of the envelope.
A small amount of anechoic periprosthetic fluid is normal (image far left).
Increasing amounts of effusion or more echogenic fluid can be punctured for investigation, depending on clinical findings.
Folding
Folds are seen in many forms. They are dynamic.
When turning outwards they are sometimes palpable, especially at the edges of the breast implant and at locations where there is little tissue between the implant and the skin.
These folds are normal findings.
Radial folds
Deep linear or curved lines within the implant can be hard to call.
Are they inner radial folds or part of a collapsed envelope as a result of intracapsular rupture? Try to look for more signs and follow the line to look for continuity with the envelope.
In some cases MRI is needed to solve this problem.
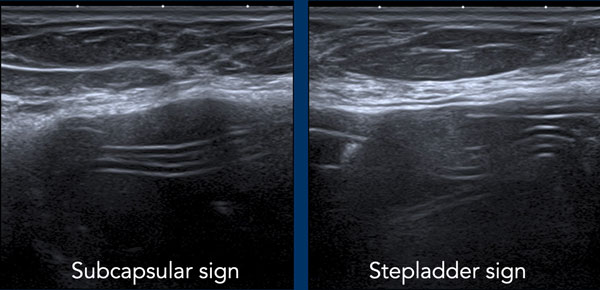
Intracapsular rupture
When the envelope ruptures, but the capsule stays intact, it is called intracapsular rupture.
The Silicone does migrate between the envelope and the capsule, but does not migrate into the breast tissue or beyond.
Signs to look for are:
- Subcapsular sign: Parallel lines within the content of the breast implant, not following the outer envelope-capsular complex.
- Stepladder sign: More layers of parallel lines within the content of the implant.
This sign is similar to the Linguine sign as seen on MR. - Snowstorm artefacts outside the envelope
Stepladder sign
US can detect intracapsular rupture by identifying a series of horizontal echogenic straight or curvilinear lines, somewhat parallel, traversing the interior of the implant, commonly known as the “stepladder sign”.
It is important not to confuse the stepladder sign with normal prominent radial folds.
Images
More examples of the “stepladder sign”.
 Stepladder sign in a patient with extreme capsular calcifications.
Stepladder sign in a patient with extreme capsular calcifications.
In this patient heavily capsular calcifications did obscure the condition of the prosthesis.
However when looking from a different angle it was obvious that there was a stepladder sign indicating rupture.
Due to the widespread calcifications, it was not sure whether it was only an intracapsular rupture or also some extracapsular leakage of Silicone.
 Intracapsular rupture
Intracapsular rupture
A. The envelope can no longer be found around the surface of the implant. The inner content is complete inhomogeneous and degenerated.
B. The envelope is collapsed (yellow arrow) and does not follow the outer envelope-capsular complex (white arrow).
There is an inhomogenous collection between the envelope and the capsule containing Silicone. .

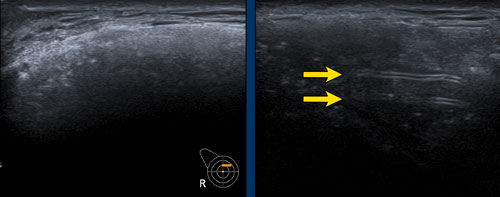
Extracapsular rupture
Extracapsular silicone implant rupture is defined as rupture of both the implant shell and the fibrous capsule with macroscopic silicone leakage that extends beyond the fibrous capsule into the surrounding breast tissue and beyond.
The Silicone which is beyond the capsule causes an acustic shadow called "snowstorm" or "dirty shadow" (figure).
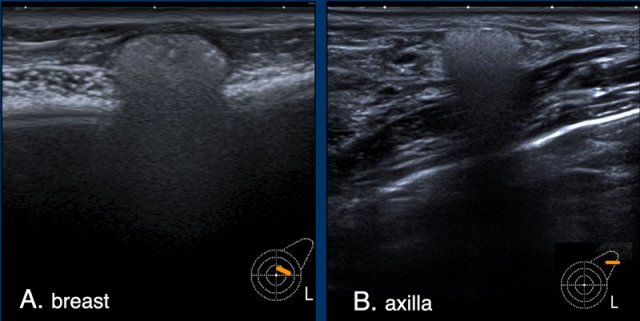
A. There is free Silicone visible outside of the envelope/capsular complex. This is a sign of extracapsular rupture. However there were no other signs of rupture of the prosthesis.
This probably is a Silicone deposit of an older implant that was removed because of extracapsular leakage.
B. The snowstorm sign in an axillary lymph node is highly specific for Silicone deposition in the lymph node.
US is more sensitive than MRI in finding these lymph node deposits.
MRI
Protocol
MRI is the gold standard for evaluation of the integrity of the breast implant with a sensitivity of 80-90% and specificity of 90-97% for detecting ruptures.
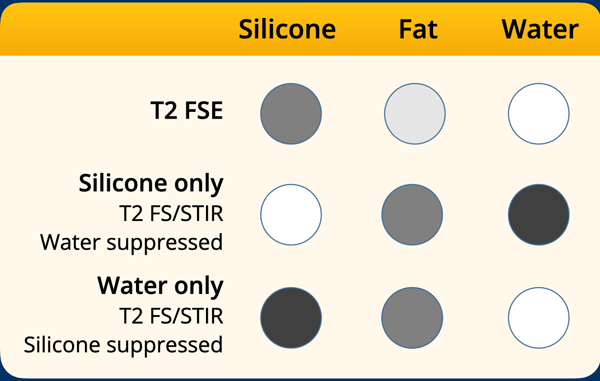
It has a high spatial resolution and the ability to suppress or enhance the signal of Silicone, water and fat.
A combination of sequences can be used to detect complications.
Gadolinium i.v. is not needed.
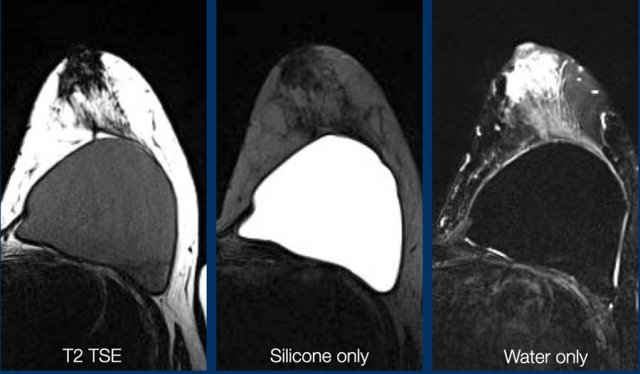
T2W-images
These are best for studying the anatomy and provide high resolution. They also give information about lymph adenopathy.
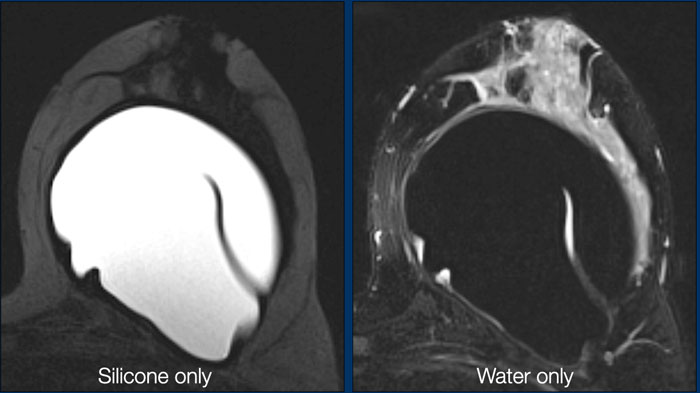
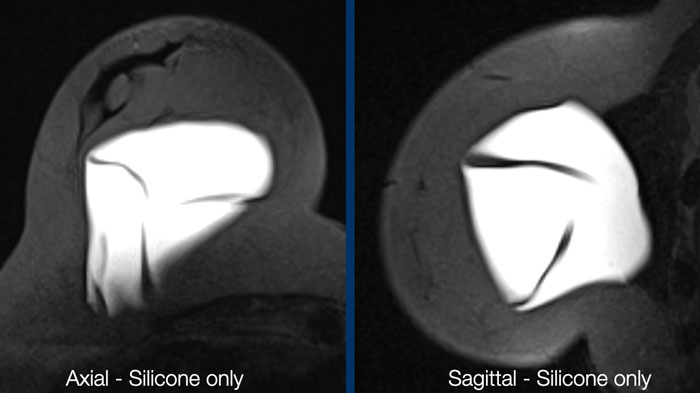
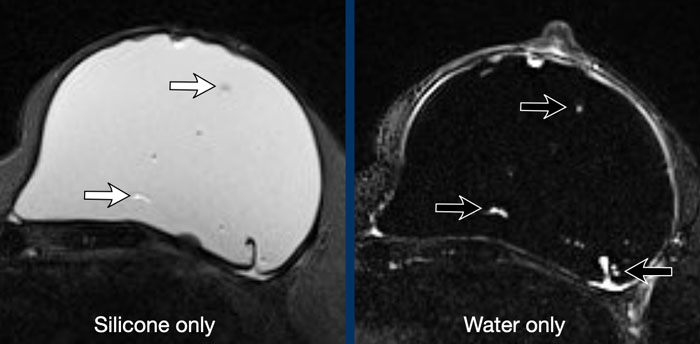
Silicone-only-images
These are STIR-images, in which fat is suppressed, combined with water suppression. As a result there is only signal of the silicone material. This sequence is ideal for studying rupture of the envelope and detecting silicone outside the envelope or outside the capsule.
Water-only-images
A combination of fat saturation and silicone suppression gives information about fluid collections within or around the prosthesis.
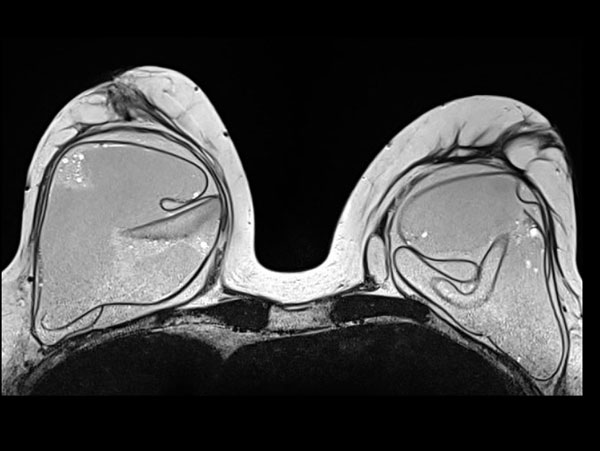
Normal findings
Small effusions are commonly seen.
They have a different signal intensity than Silicone and should not be confused with the keyhole sign.
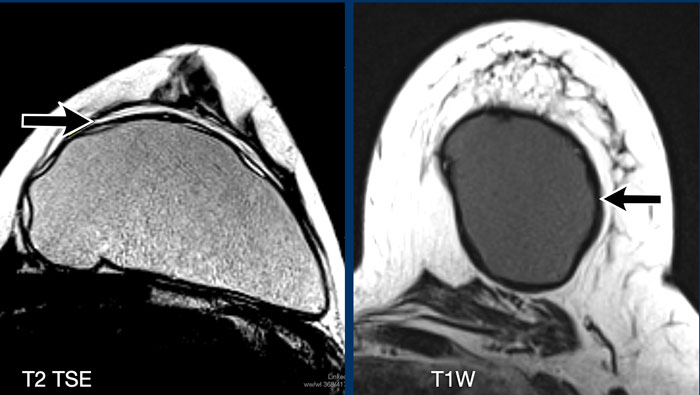
The T2W-image shows an effusion filling the virtual space between the envelope and the capsule. This is a normal finding.
The T1W-image shows a hypointens
thickened capsule. The capsule will show hypointense on any sequence.
The contour of the implant is more
rounded, which indicates capsular contraction.
Although signs of contraction can be well seen on imaging, the degree of contraction is estimated by physical exanination.
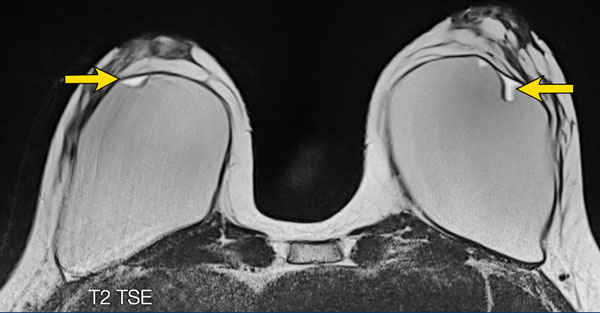
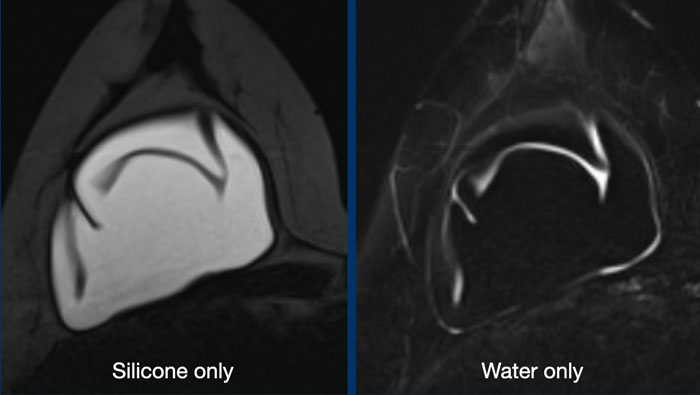
 Normal radial folds
Normal radial folds
Radial folds are infoldings of the envelope extending from the surface into the gel content.
This is also a normal finding.
The content within the fold-lines should not contain Silicone.
 Normal radial folds
Normal radial folds
More normal radial folds.
 Normal radial folds
Normal radial folds
Here more examples of normal infolding of the envelope.
There is no silicone content within these folds.
 Normal radial folds
Normal radial folds
Another example of an extensive deep course of normal radial folds.
Water droplet sign
Multiple small round internal drops with fluid signal within the silicone gel can be a sign of degeneration.
However there should be more signs to consider a possible rupture.
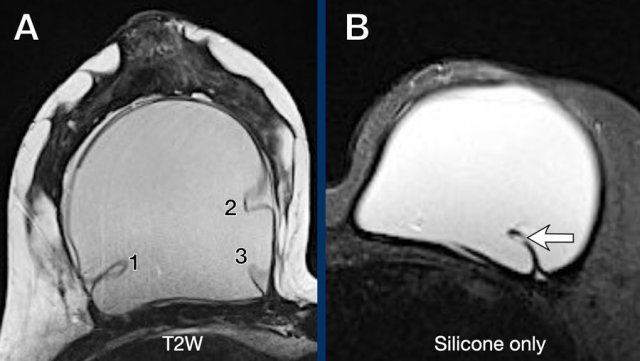
Intracapsular rupture
When there is silicone within a fold, then it is a sign of intracapsular rupture.
The images show:
- Teardrop sign: where the walls touch each other (1).
- Keyhole or Noose sign: different shapes, the walls do not touch each other (2-3).
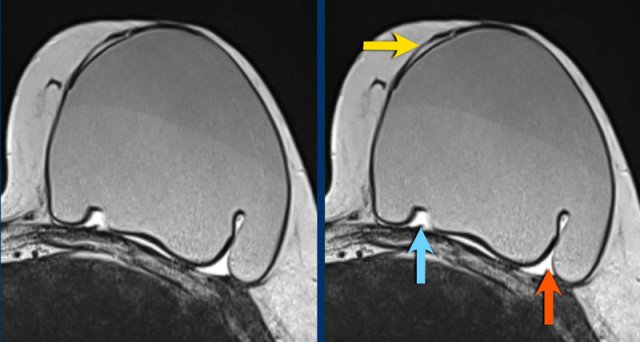
Here another example of the different presentations of intracapsular rupture with silicone outside the envelope, but within the capsule.
- subcapsular line (yellow arrow)
- nose sign (blue arrow)
- teardrop sign (red arrow)
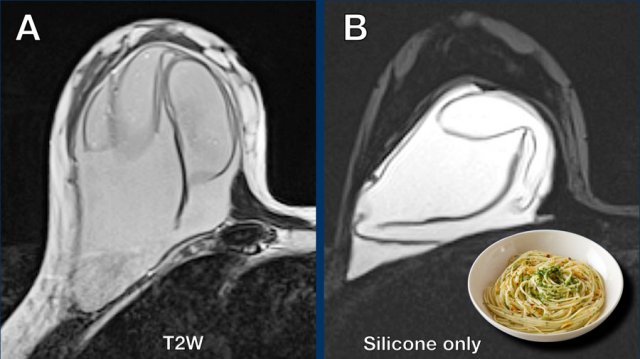
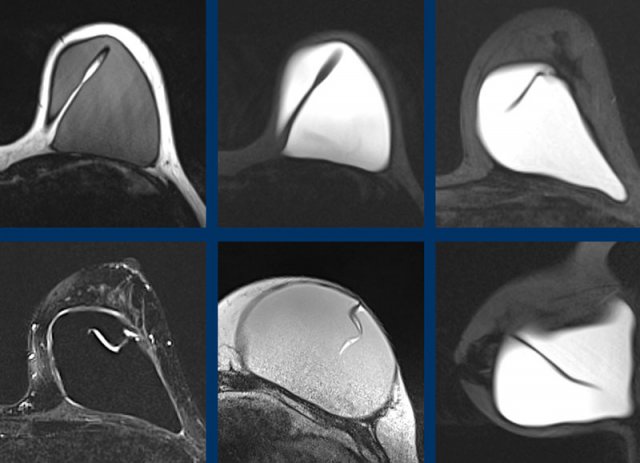
Linguine sign
This is the most reliable sign of intracapsular rupture.
The curvilinear lines which are formed by the ruptured envelope resemble Linguine pasta.
First study the image and answer the following question:
- Which signs do you see.
- How suspective is each of these findings for rupture?
Then scroll the image.
- Green: degenerative but not a sign of rupture.
- Orange: suspective of intracapsular rupture but not a definitive sign. You need other sequences to determine whether it is Silicone.
- Red: Linguine sign - proof of intracapsular rupture.
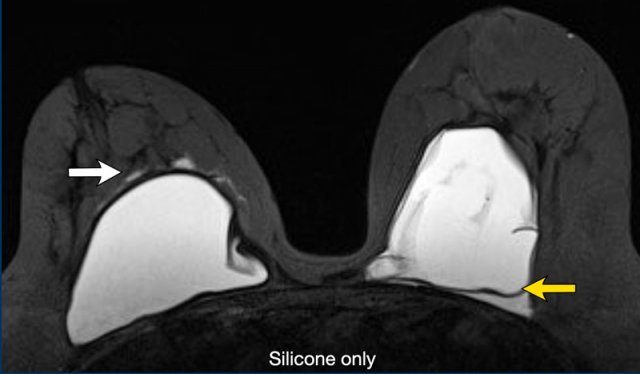
Extracapsular rupture
This woman has an extracapsular rupture on the right with silicone outside the thickened capsule (white arrow).
In the left breast there is an intracapsular rupture indicated by the subcapsular line with silicone on both sides of the line (yellow arrow).
Another example of extracapsular rupture with silicone outside the capsular border.
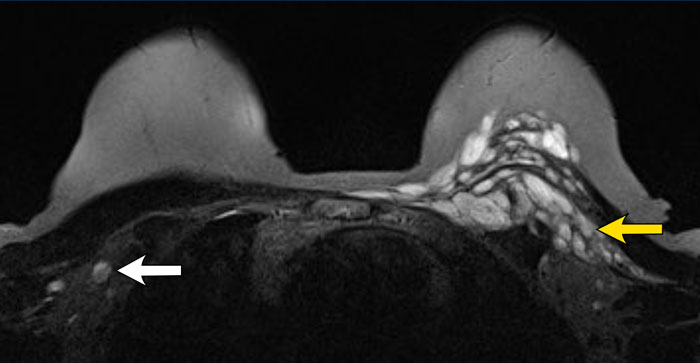 Residual Silicone after explantation
Residual Silicone after explantation
This patient had bilateral removal of the breast implants.
On the right there is high signal of silicone material in lymph nodes (white arrow).
On the left there is residual silicone anterior and posterior to the major pectoralis muscle (yellow arrow) and also within the muscle.
When a new silicone prosthesis is implanted, this residual silicone should not be interpreted as extracapsular leakage of the new implant.
BIA-ALCL
Anaplastic Large Cell Lymphoma
BIA-ALCL or breast implant associated anaplastic large cell lymphoma is an important complication to know of silicon-filled and saline-filled breast implants.
BIA-ALCL develops primarily if not exclusively in patients with textured implants.
The estimated prevalence in these implants is 1:30.000.
Most BIA-ALCL were seen in Allergan Biocell textured breast implants and they were subsequently taken off the market.
Two-thirds of individuals with BIA-ALCL present with discomfort and swelling due to the development of periprosthetic effusion (85%) in which atypical lymphoid cells are found. Sometimes associated with a mass in 15% of cases.
Any late onset unilateral effusion or mass should be punctured and analyzed.
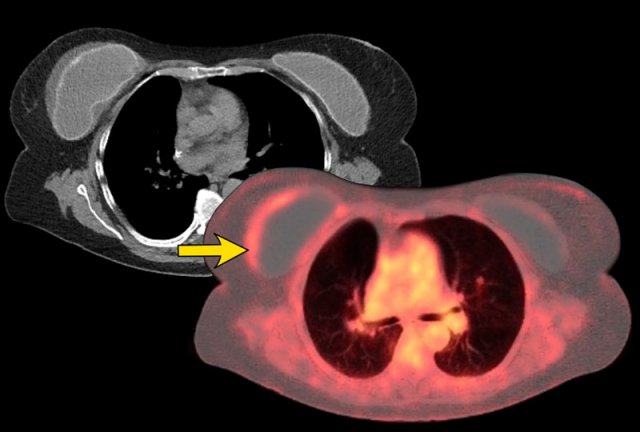
Staging is with PET-CT, like in any other lymphoma.
Most patients present with Stage 1.
The treatment is surgical excision of the implant, capsule and mass if present.
Outcome is favorable when early treated.
X-Ray and CT
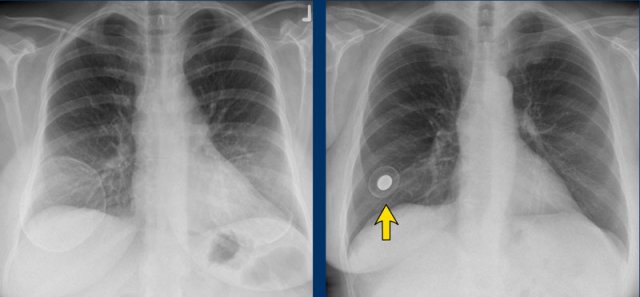
Chest X-Rays and CT do not play a role in examining breast implants.
Sometimes they can be detected on X-rays for instance when there are capsular calcifications or when a filling valve of an expandable prosthesis is seen (arrow).
Also on CT sometimes complications can be seen, but usually CT does not give adequate information about the integrity of the prosthesis.
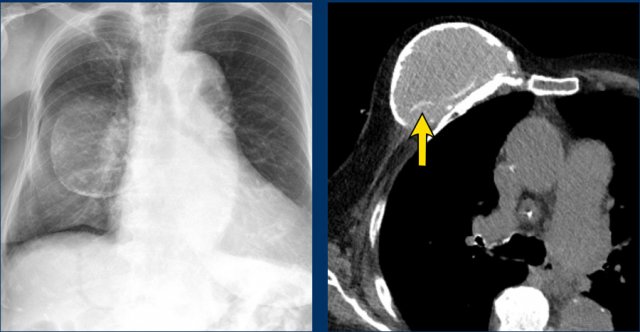 Intracapsular rupture
Intracapsular rupture
The chest film shows capsular calcifications in a medially displaced breast implant, which is not parallel to the breast contour.
The CT of the same patient shows also calcifications at the posterior side not following the contour of the implant indicating intracapsular rupture (arrow).
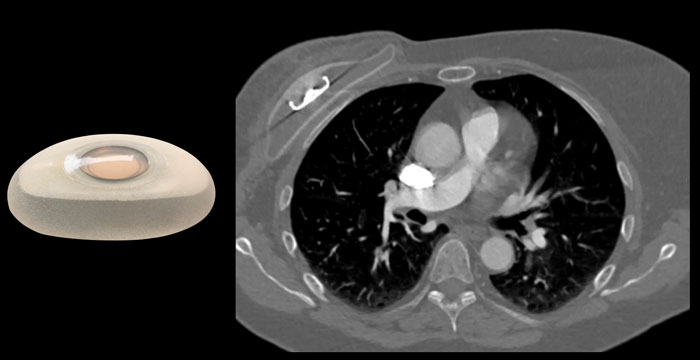
 Saline filled prosthesis
Saline filled prosthesis
An intact implant has a homogeneous grey internal density on CT with a surrounding thin more hyperdens envelope and capsule.
Location abnormalities and different types of fill valves can sometimes be seen.
This patient has a saline filled prosthesis with a low internal density.
A thin slightly hyperdens regular envelope is seen.
 Metallic valve
Metallic valve
On CT different types of fill valves of breast implants can be seen.
Capsular calcifications are frequently seen and sometimes the Linguine sign (arrow).
In most cases the findings on CT will be inconclusive.
The left implant in this patient shows capsular calcifications, which are not located at the periphery and which are discontinuous.
Unclear whether this is an extracapsular rupture or whether there is a large effusion.
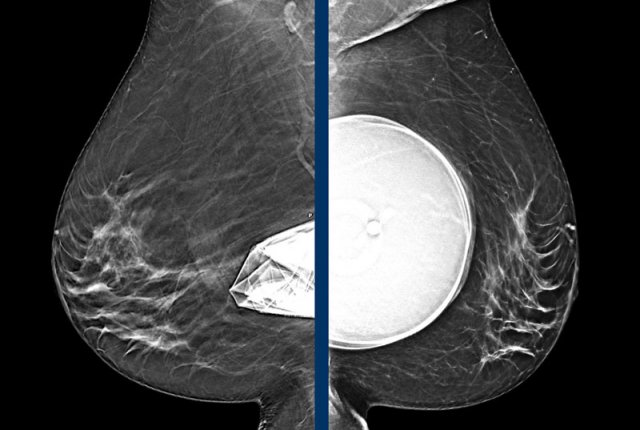
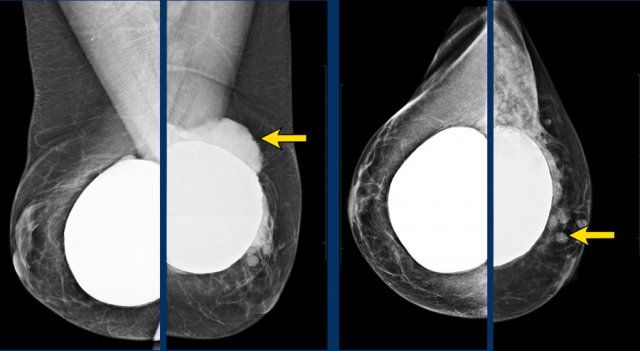
Mammography
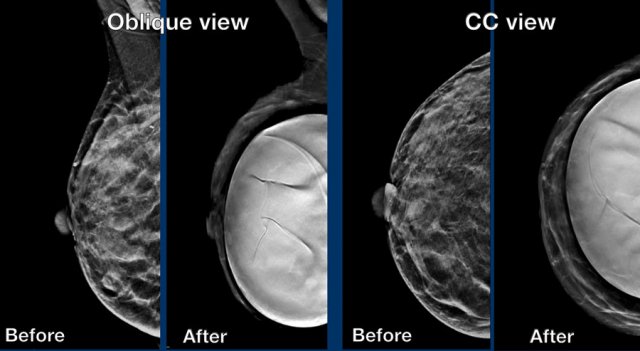
Same patient before and after prepectoral breast augmentation.
Especially prepectoral implants can reduce mammographic assessment.
Still
mammography and 3D tomosynthesis can be well performed and in fact has the highest
PPV for recognition of extra capsular silicone.
It also objectively detects changes
in time, shows calcifications, can show surrounding fluid shadow and of course adds
important findings in fibroglandular tissue.
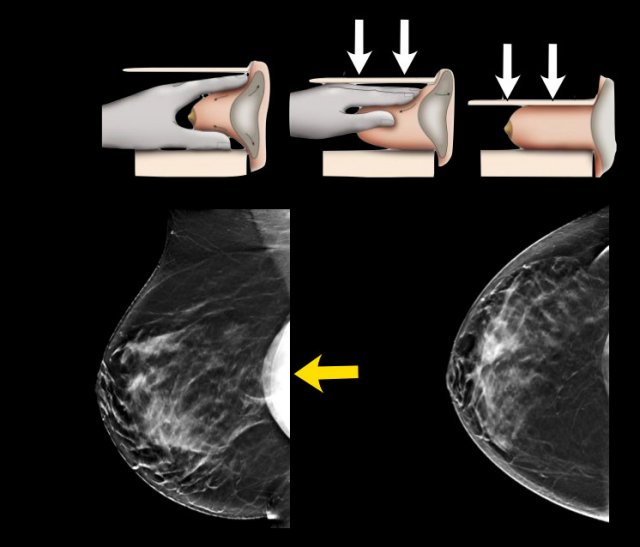
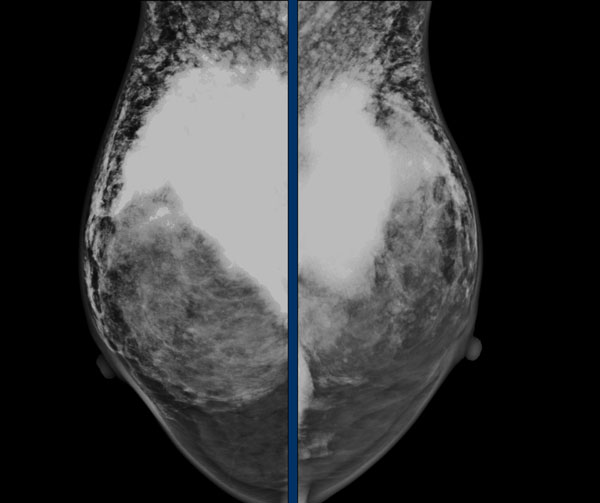
Eklund technique
Special views can be performed such as the Eklund views.
By pushing the implant posteriorly and pulling the breast tissue anteriorly better visualization of the fibroglandular tissue can be achieved.
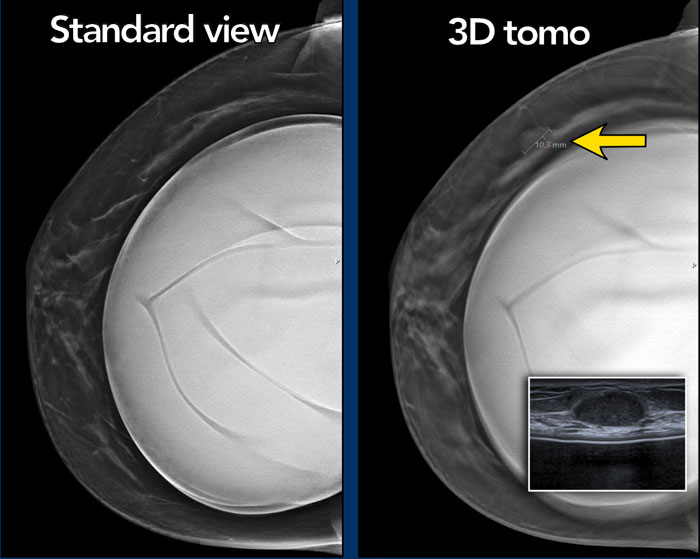
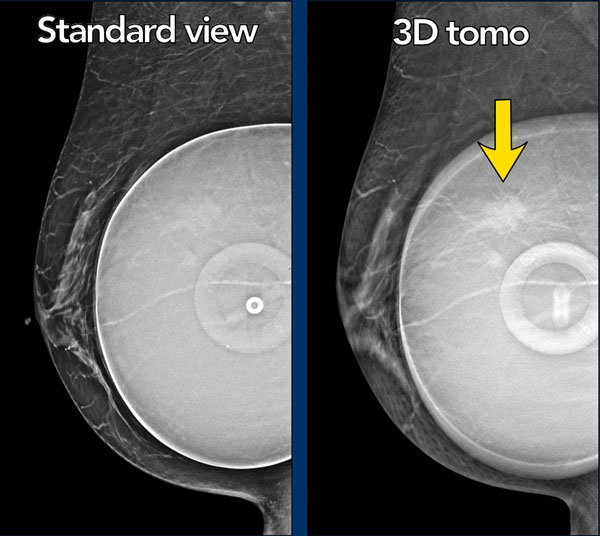
Tomosynthesis
Tomosynthesis can be very useful as in this case.
There is a mass on the lateral side, which is best seen on the 3D tomographic image.
Ultrasound guided biopsy was performed and this mass proved to be a fibroadenoma.
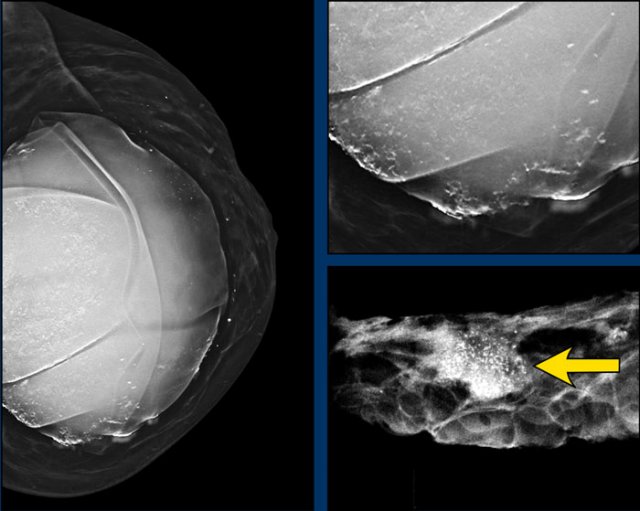
On this mammogram there were both capsular calcifications and atypical extracapsular calcifications.
Detail of the specimen showing mass and grouped calcifications.
Pathology: breast cancer grade 2, no special type (NST).
This woman has a saline filled implant and shows a discoid diaphragm, which is the fill valve.
There is a mass, which is more obvious on the tomosynthesis (image 56 out of 73).
It is a spiculated mass.
Pathology: infiltrating lobular carcinoma grade 2 and LCIS.
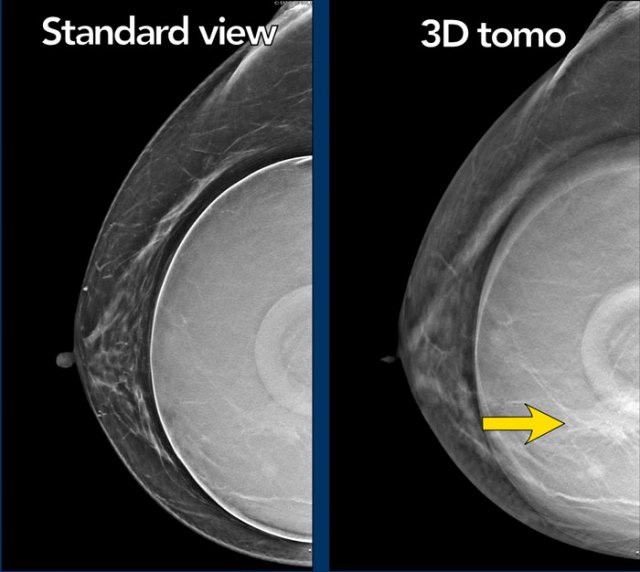
Another example of the value of tomosynthesis.
The tumor is best seen on the tomographic view.
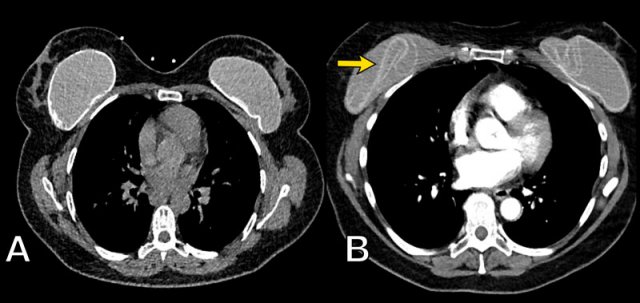
Complications of implants
The oblique view of the right breast shows a deflated ruptured Saline filled implant.
A normal saline filled implant with filling valve on the left.
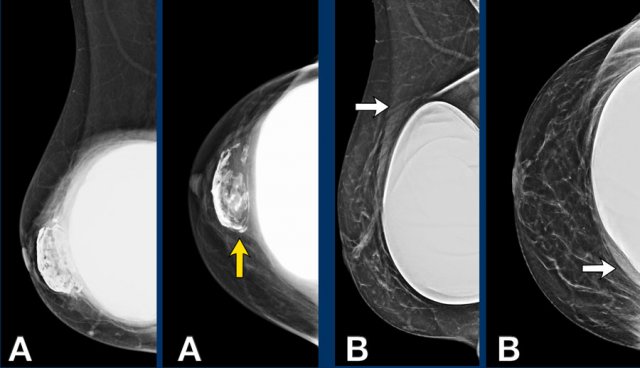
In A there are prepectoral capsular calcifications of a previous inplant and a subpectoral prosthesis.
In B there is a situation after operative capsulectomy and replacing of the subpectoral breast implant.
 Silicone leakage
Silicone leakage
Typical appearance of silicone outside of the capsule presenting as dense well deliniated masses outside the contour of the breast implant.
 Silicone granulomas
Silicone granulomas
Silicone granulomas
Silicone granulomas remainig after removal of breast implant because of previous extracapsular rupture in 2013.
Silicone granulomas can manifest as masses with suspicious morphology and enhancement dynamics on breast MRI or with increased FDG uptake on PET CT.
They
can present at the periphery of the prosthesis or in breast tissue after
rupture.
The presence of silicone implants and awareness of the possibility of a rupture and formation of silicone granulomas may help in facilitating a correct diagnosis (ref).
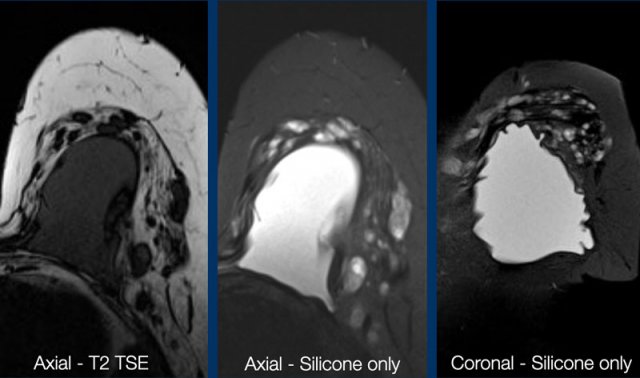
 Free silicone breast injections
Free silicone breast injections
Free silicone breast injections
This is an alternative form of breast augmentation, although it has serious adverse effects and is banned in many countries.
This patient from the Philipines presents with bilateral painful lumps in the breasts.
The massive densities in both breasts are the result of silicone intraglandular injections.
Continue with the MR...

MRI of the same patient showing free silicone as areas of high signal on silicone-only sequence.
Surgery
Removal of thickened capsule
In this video first an incision is made in the thickened capsule.
The implant is subsequently removed through this incision.
Finally the thickened capsule is removed.