AO Spine Classification of Thoracolumbar Fractures
Sander P.J. Muijs¹, Wouter Foppen², Frank Smithuis³ and Robin Smithuis⁴
¹Department of Orthopedic Surgery and ²Radiology and Nuclear Medicine, University Medical Center Utrecht, ³University Medical Center Amsterdam, ⁴ Alrijne Hospital, Leiden, the Netherlands
Publicationdate
The AO spine classification is the new standard for classifying spine injury.
It is developed by the AO Spine Knowledge Forum Trauma.
The forum members looked at all existing classification
systems and formulated the most comprehensive system based on three injury
mechanisms with increasing severity: compression (A), distraction (B) and
translation (C).
The classification is a primarily CT-based and easy to use.
In most cases, MRI is not
needed for correct classification.
Click here for AO Spine Classification Systems—the complete guides which includes the video guide and studies
Overview
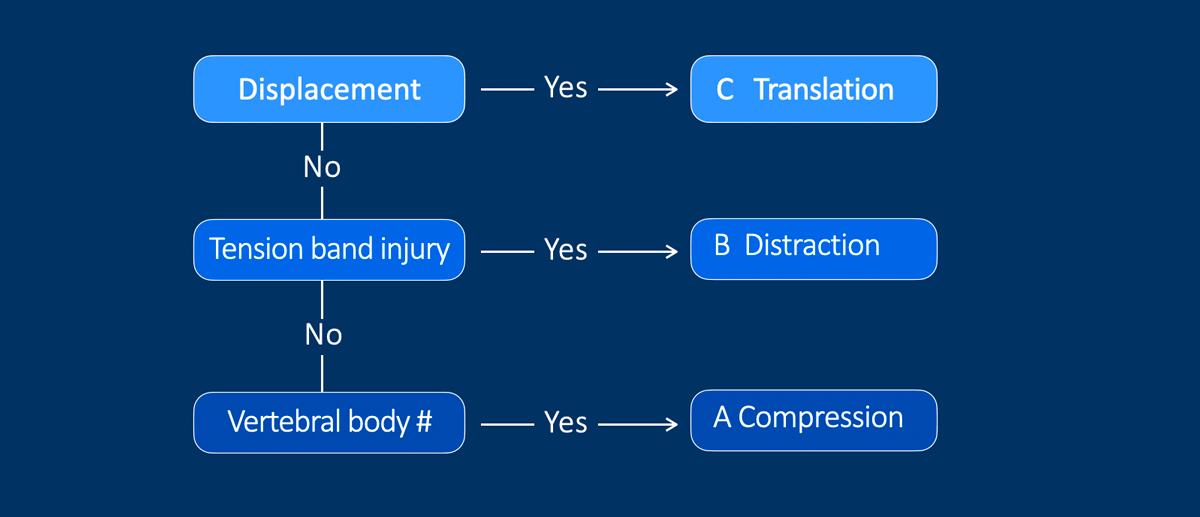
This is a simplified roadmap of the AO spine classification.
It is based on the principle, that you first look for the most severe scenario.
When you study the images, ask yourself:
- Is there displacement of a vertebral body in relation to the adjacent vertebral body, i.e. a translation injury (type C).
- If it is not a C, then the next question is, whether there is an anterior or posterior tension band injury, i.e. a distraction injury (type B).
- If it isn't a B, then the next question is, whether there is a vertebral body fracture, i.e. a compression injury (type A).
Note: Type A injury can occur isolated or in combination with a type B or C injury.
This is why the classification starts with the most extensive injuries, so you will not miss anything.
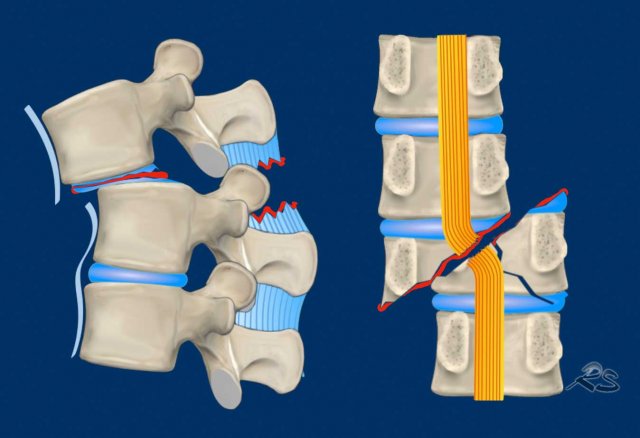
Translation
Type C - Translational injuries are characterized by dislocation of a vertebral level from the level below or above in any direction.
No subtypes are present as there are numerous possibilities of dislocating fractures.
However, they should be specified along with relevant vertebral body (A-type) or tension band (B-type) injuries to better describe the morphology.
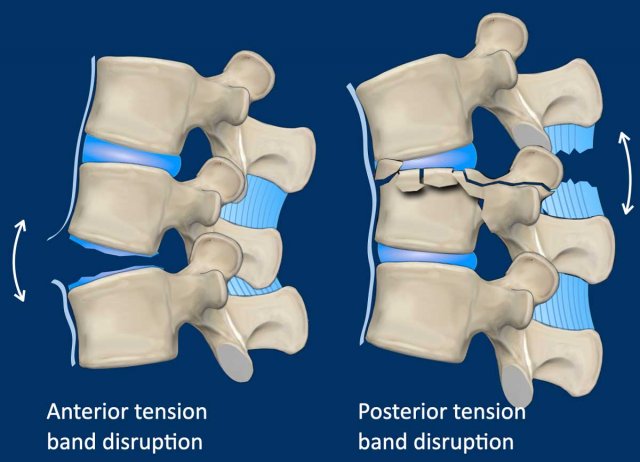
Distraction
The next most severe injury is distraction.
Distraction injury means that two or more vertebral levels are distracted or partially separated from each other.
Hyperextension can lead to distraction of the anterior tension band.
Hyperflexion can lead to distraction of the posterior tension band.
Anterior tension band
This is formed by the vertebral bodies, the anterior and posterior longitudinal ligaments and the intervertebral discs.
This type of injury is often seen in individuals with a rigid spine like diffuse idiopathic skeletal hyperostosis or ankylosing spondylitis and can occur even after minor trauma in this patient group.
Posterior tension band
This is the major stabilizer of the spine limiting flexion and reducing the axial load on the intervertebral discs.
It is formed by:
- Osseous structures: pedicles, transverse processes, spinous processes.
- Non-osseous structures: ligamentum flavum, ligamentum inter- and supraspinosum and the facet joints.
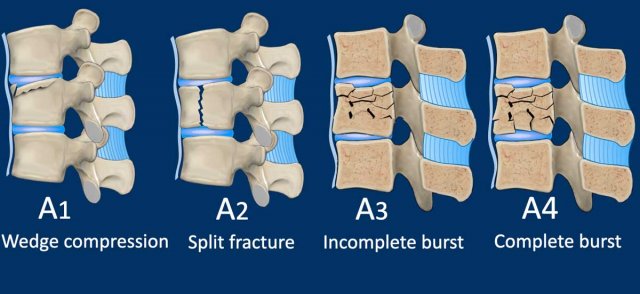
Compression
If it is not a type C or B injury, we ask ourselves whether there is a type A compression injury.
Compression injuries are fractures of the vertebral bodies:
- A1 fracture of one endplate.
- A2 split fracture where both endplates are involved without affecting the posterior wall of the vertebral body
- A3 incomplete burst fracture, where the posterior wall and one endplate are involved
- A4 complete
burst fracture, where the posterior wall and both of the endplates are
involved.
Note: Type A
injury can occur isolated or secondary to B or C injury.
In addition there is a type A0 fracture, which is a minor non-structural fracture, that does not affect the stability of the spine, e.g. a fracture of the transverse process or spinous process.
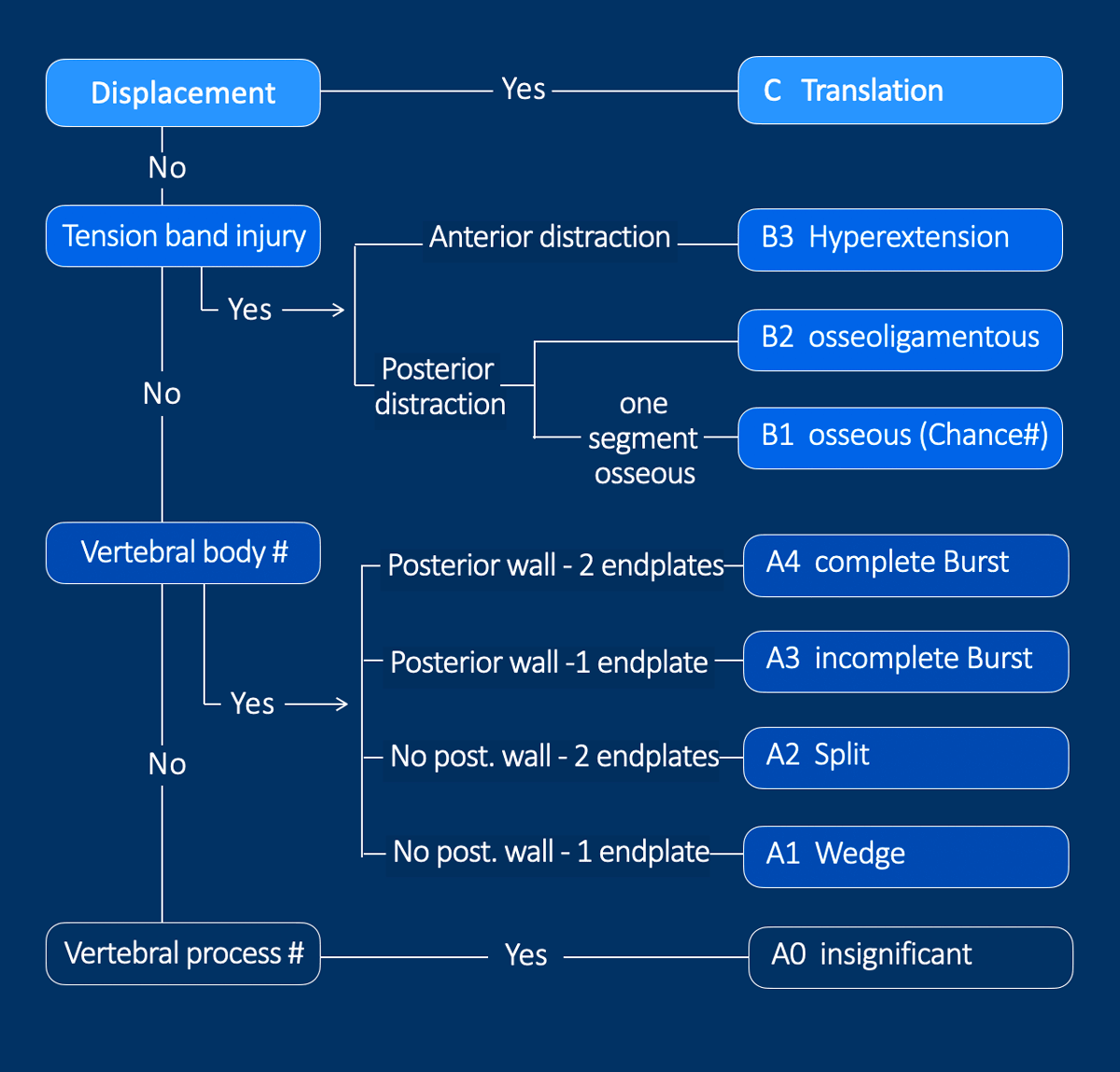
Roadmap
This is the complete version of the roadmap of the AO-spine classification.
It starts with the most severe injury, which is C translation and finally ends with the insignificant A0-injury.
C translation
When there is displacement, it is a C-type translation injury without any subclassification.
When you describe a type C injury, both involved levels which are
displaced from each other are described: e.g. Th8-Th9 AO type C.
B distraction
If there is anterior
distraction with disruption of the anterior tension band, you call it a
B3-hyperextension injury.
If there is injury to the
posterior tension band, it is usually a combination of osseous and non-osseous
injury (B2).
Occasionally it is a purely osseous injury (B1) also
known as Chance fracture.
In general a B1-type injury has a
better prognosis than a B2-type injury.
A compression
When there is a compression fracture of a vertebral body, the subclassification is determined whether there is a fracture of one or both endplates and whether the posterior wall is involved.
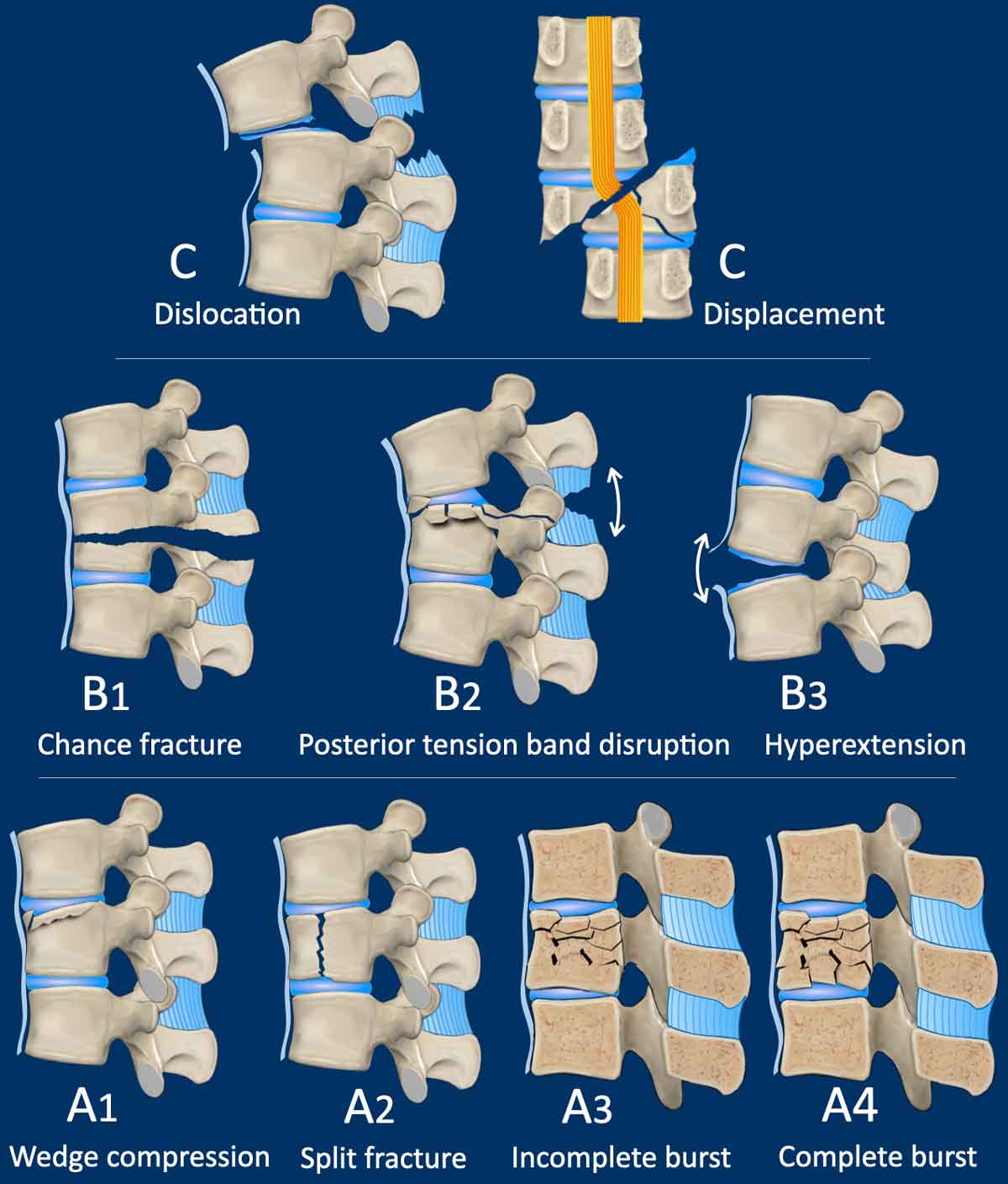
Complete overview
This illustration summarizes the different fracture types of the AO-spine classification (adapted from reference 1).
Type C - Translational injuries are characterized by:
- Dislocation or displacement of a vertebral level from the level below or above in any direction.
Type B - Distraction injuries are characterized by:
- Hyperflexion with distraction of the tension band on the posterior side.
Usually a combination of osseous and non-osseous injury (B2), but ocassionally a purely osseous injury (B1). This is also known as Chance fracture. - Hyperextension with distraction of the tension band on the anterior side (B3). This is a common injury in patients with a stiff back.
Type A - Compression fractures of the vertebral bodies:
- A1 fracture of one endplate.
- A2 split fracture where both endplates are involved.
- A3 a burst fracture, where the posterior wall and one of the endplates are involved.
- A4 a complete burst fracture, where the posterior wall and both of the endplates are involved.
A helpful tool to classify the subtypes of A injury is the following:
- Both endplates of the vertebra are each worth 1 point, the posterior wall 2 points.
- Add up the points for the involved cortices of the vertebral body and you will get the correct subtype A injury.
Type C Translational injuries
We start with the most severe injury and work from there.
Translational injuries are dislocation or displacement of a vertebral level from the level below or above.
There are no subtypes because various configurations are possible.
There is a high degree of instability and therefore an indication for surgery.
Images
Here we see a dislocation of the proximal levels to the right lateral side in the coronal plane.
Conclusion
Type C injury.
What is the highest AO-type of injury?
Images
This is a clear example of translation in the anterior direction.
Conclusion
Type C injury.
Scroll through images.
What are the findings?
What is the highest AO-type of injury?
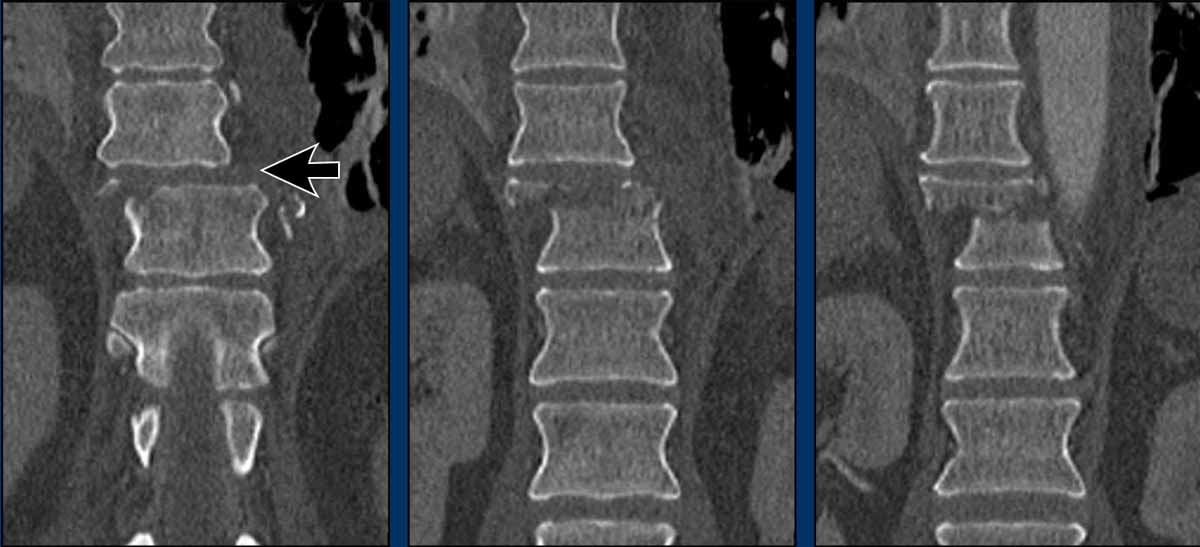
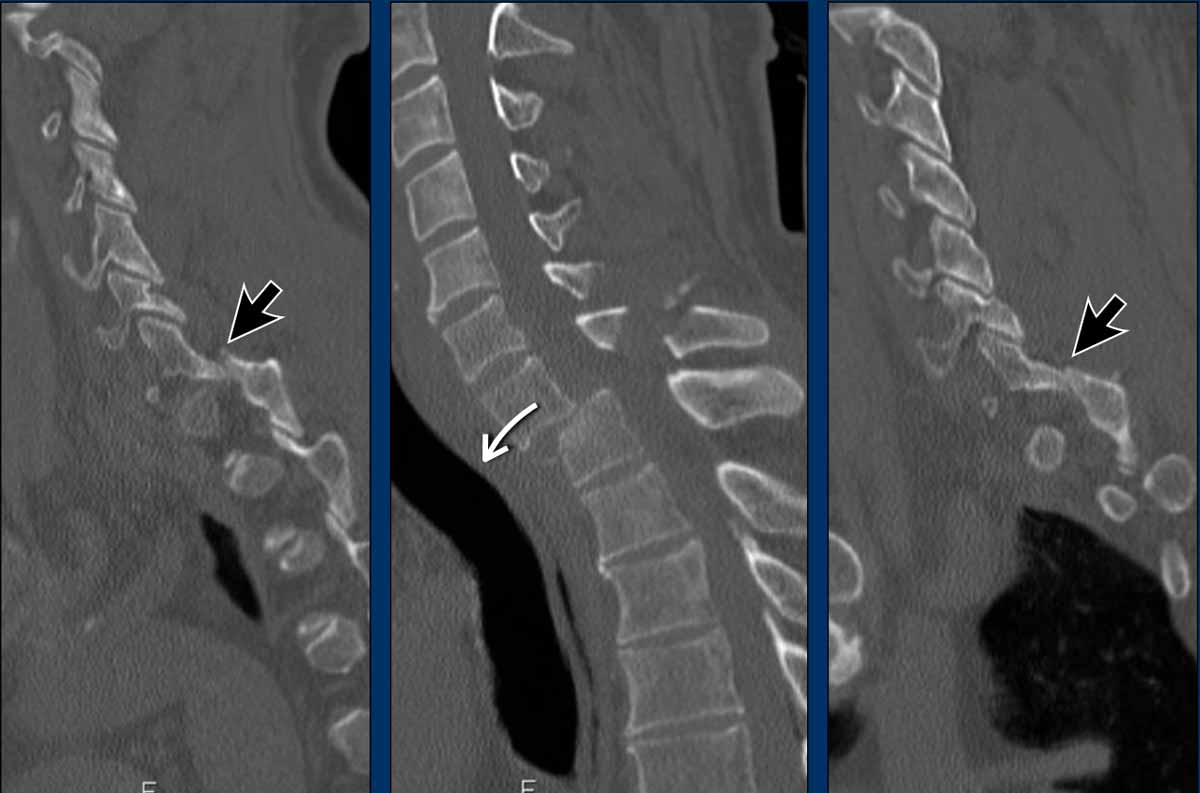
Findings
- Dislocation of the proximal vertebrae anteriorly (white arrow).
- Both facet joints are perched (black arrows). Perched means to be situated above or on the edge of something. In this case the inferior process of vertebral articular joints appears to sit on the ipsilateral superior articular process of the vertebra below.
- Due to the anterior displacement a fracture of the spinous process is seen, in a horizontal oblique course.
Conclusion
Type C injury.
First look at the images.
What are the findings?
What is the highest AO-type of injury?
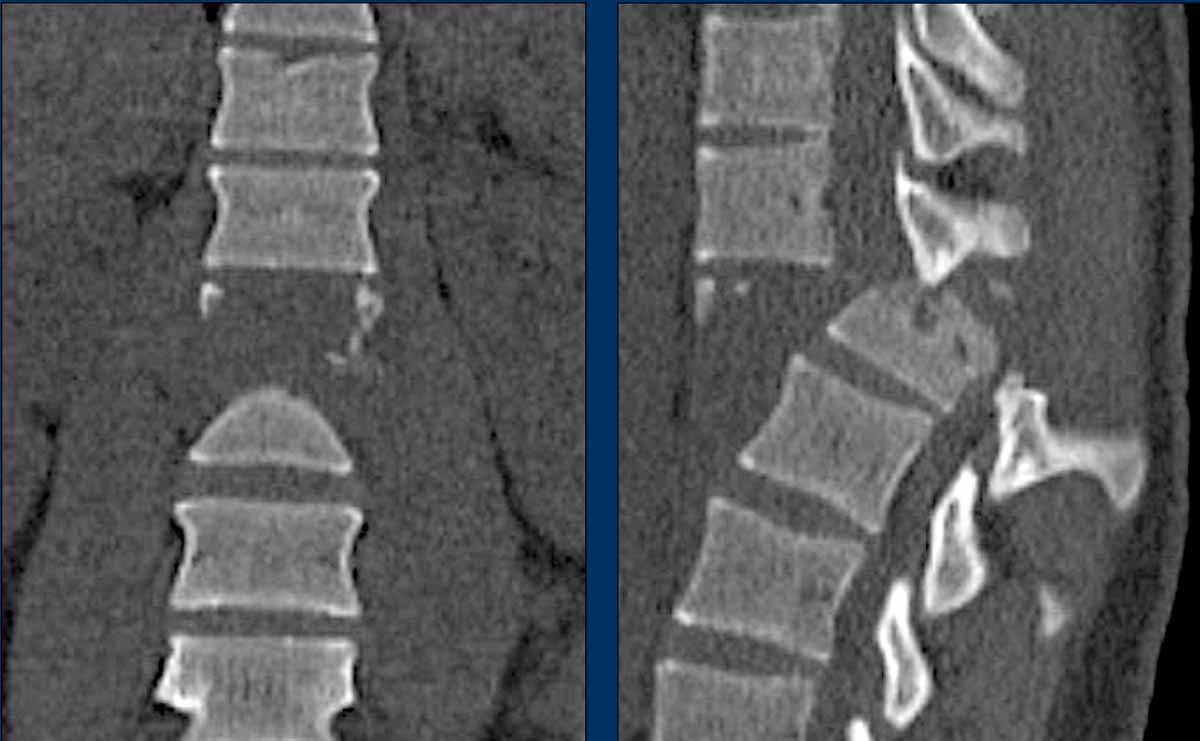
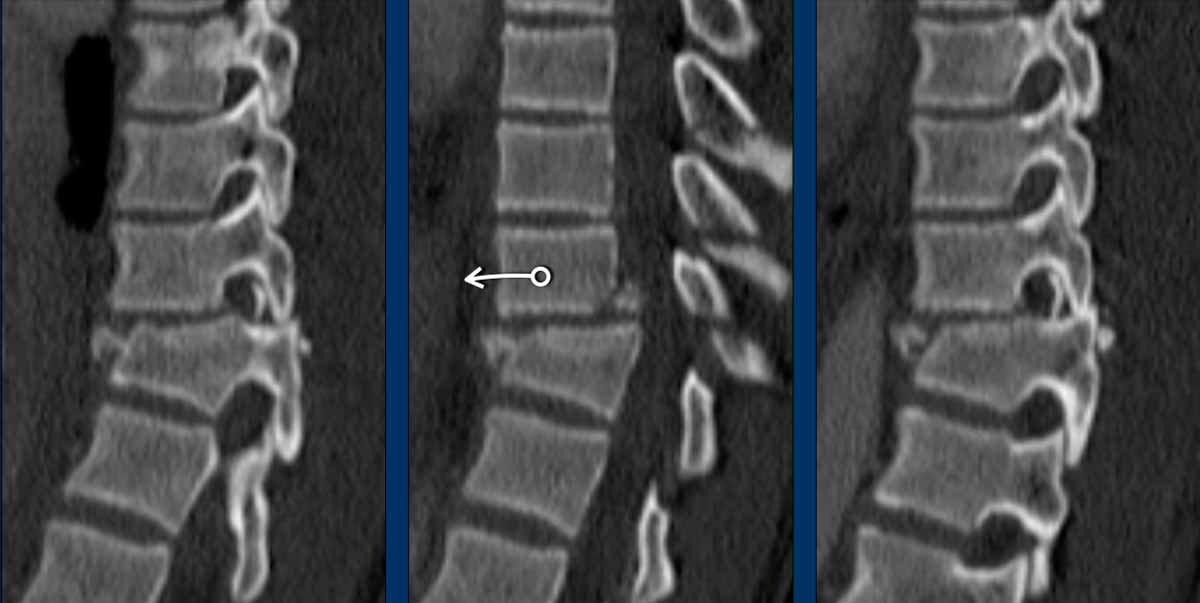
Findings
- Both facet joints are perched or displaced (black arrows).
The displacement of the vertebrae (white arrow) is not as striking as in previous cases. - There are fractures of the spinous processes on multiple levels.
This is a common feature in C injuries. - Pay attention to the chip fractures on the endplates.
Conclusion
Type C + A1 injury.
Scroll through the images
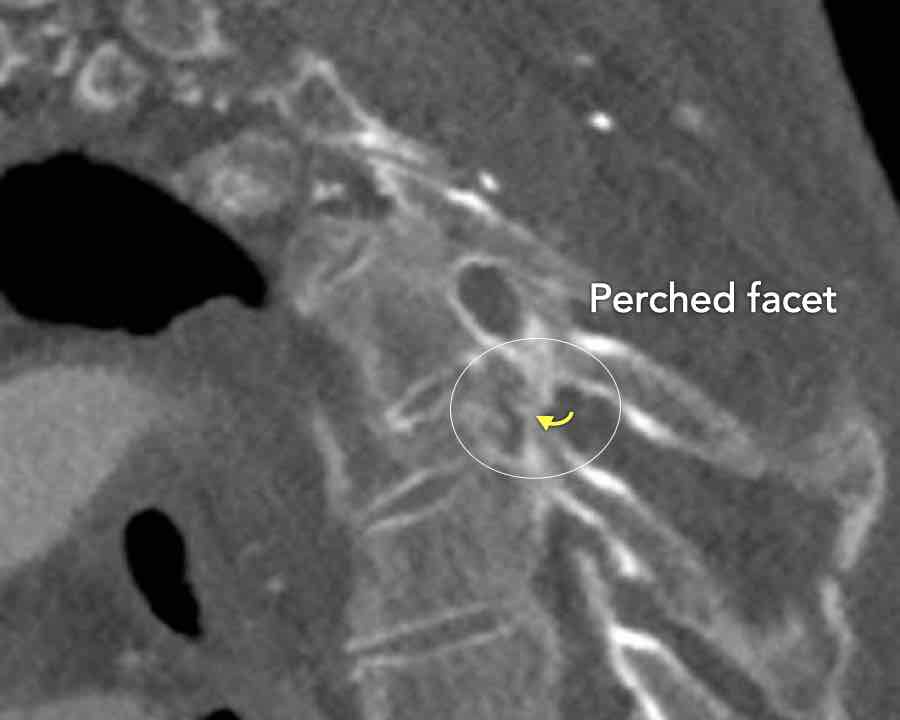
Findings:
- Perched facet joints (yellow curved arrows), so think of C injury.
- Posterior displacement of the vertebral bodies in the midline.
- Secondary A4 injury of the vertebral body.
Conclusion
Type C + A4 injury

Scroll through images.
What are the findings?
What is the highest AO-type of injury?
Findings
- At a first glance we see a oblique fracture of the vertebral body (A1).
- But as mentioned before, we have to start with the most severe type (C) and work from there.
- So ask yourself: Is there a dislocation in the transverse plane present (yes, look at the white lines) and is there a perched facet joint present (yes, unilaterally on the left side)
Conclusion
Type C + A1 (only upper endplate)

Scroll through the images.
What are the findings?
What is the highest AO-type of injury?
Findings
- Vertical fracture of the posterior border of the vertebral body. It looks a bit odd.
- Again we first have to look for the presence of a type C injury.
- Notice that there is a subtle posterior dislocation of the proximal levels. So this has to be C injury.
Conclusion
Injury type C + A3
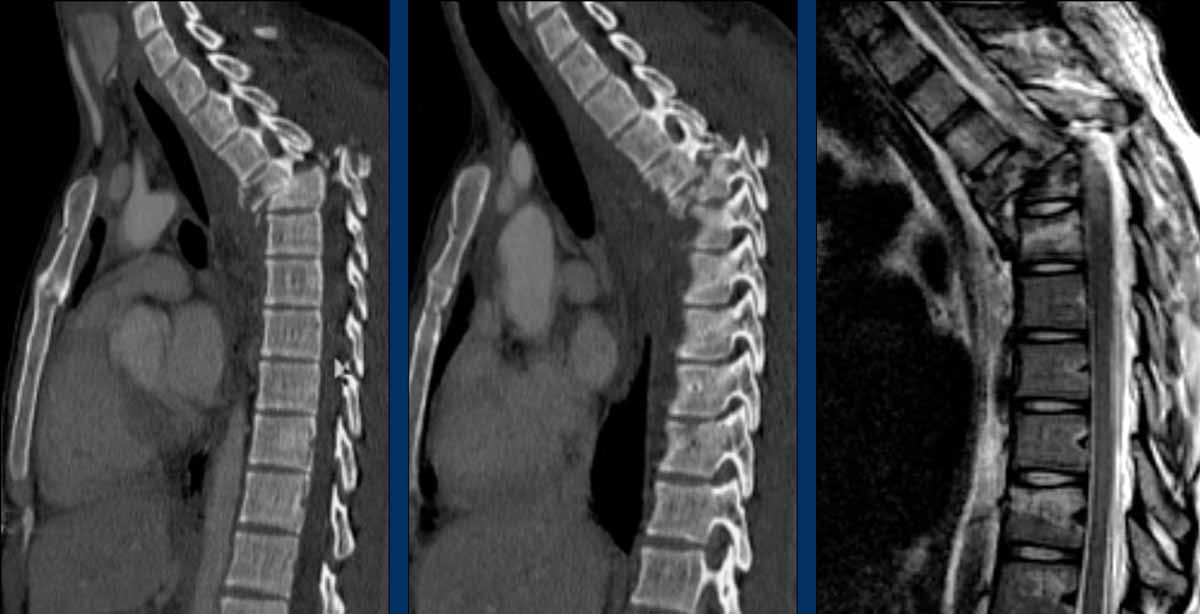
These images are of a 65 year-old woman who fell from her bike.
Scroll through the images.
What are the findings?
What is the highest AO-type of injury?
Findings
There is a type C injury.
In addition to the dislocation in the upper thoracic spine, there is also a sternum fracture, further increasing instability alongside the severe spinal injury.

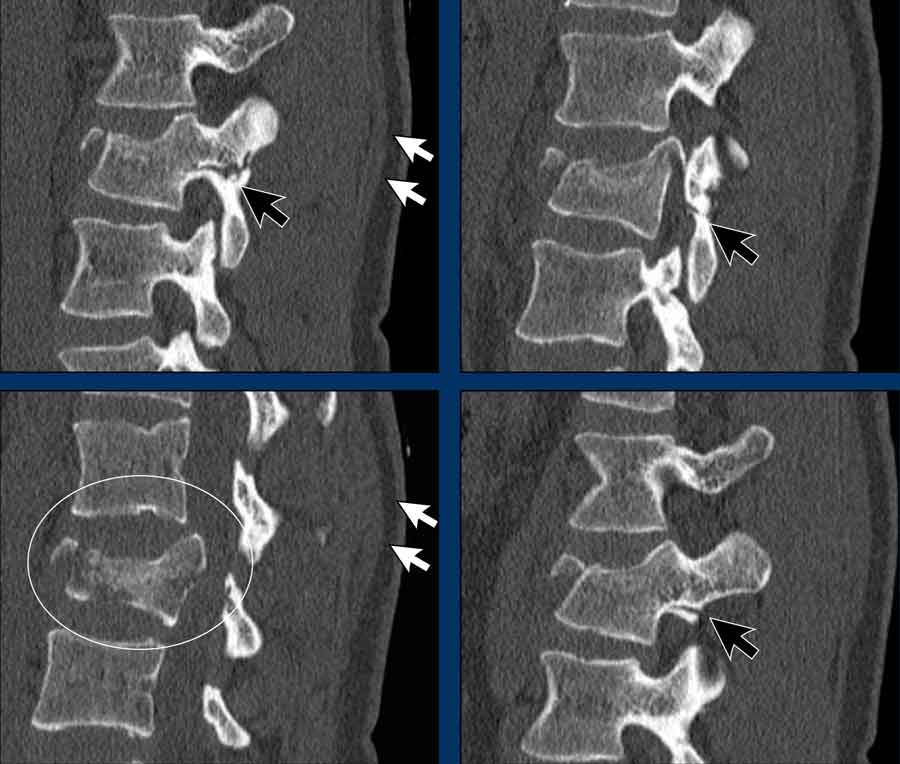
This is a difficult case with injuries at many levels.
What is the most severe level for classification.
Then continue with the second stack below for classification of other levels.
Findings
- The most severe level is L4/5 with dislocation (dotted lines)
- Facet fractures at L4 (arrows).
- A4 burst fracture (circle).
Conclusion:
Injury type C + A4 at L4/5.
Continue with the next stack of images to classify level L2...
Scroll through images.
What is the highest AO-level?
Findings
- No dislocation ( no C type).
- Mainly horizontal fractures of spinous processus at multiple levels (B-type).
- Split fracture L2 (type A2).
Conclusion
Injury type B2 + A2 at level L2.
The combination of these fractures make it difficult to comprehend what exactly has happened.
The AO spine classification is only designed to classify these injuries as simple as possible.
Type B / Distraction injuries
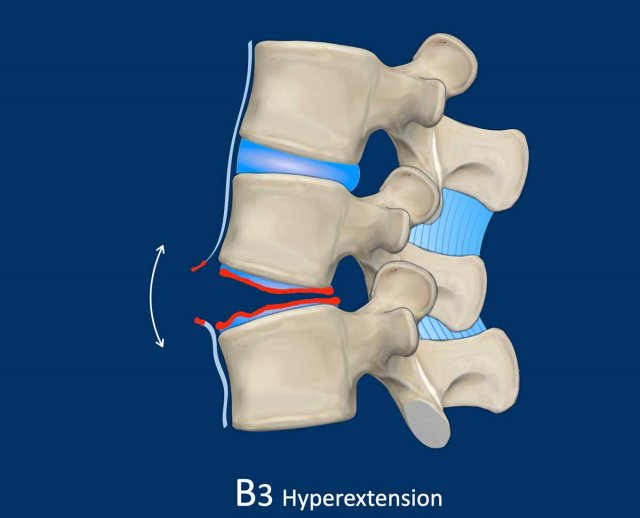
B3 Extension distraction injury
Hyperextension can result in distraction of the anterior tension band, which is formed by the vertebral bodies, the anterior and posterior longitudinal ligaments and the intervertebral disc.
These injuries can be difficult to detect since patients are scanned in the supine position laying on their back, which may obscure the anterior distraction.
However, these injuries mainly occur in patients with a rigid spine as a result of osteoarthritis, DISH or Ankylosing Spondylitis (SpA).
Stay persistent when examining a patient with a rigid spine until you have found the B3 injury.
Extension distraction is characterized by:
- Distraction of the tension band on the anterior side.
- Any horizontal or oblique fracture line through vertebral bodies anteriorly with separation on both sides.
- Widening of intervertebral disc space.

Scroll through images.
What are the findings?
Findings
- C injury? No.
- Signs of a rigid spine?
Yes, so be aware of potentially very subtle B3 injury. - A subtle fracture on the anterior vertebral body is seen (arrows).
Conclusion
Injury type B3.

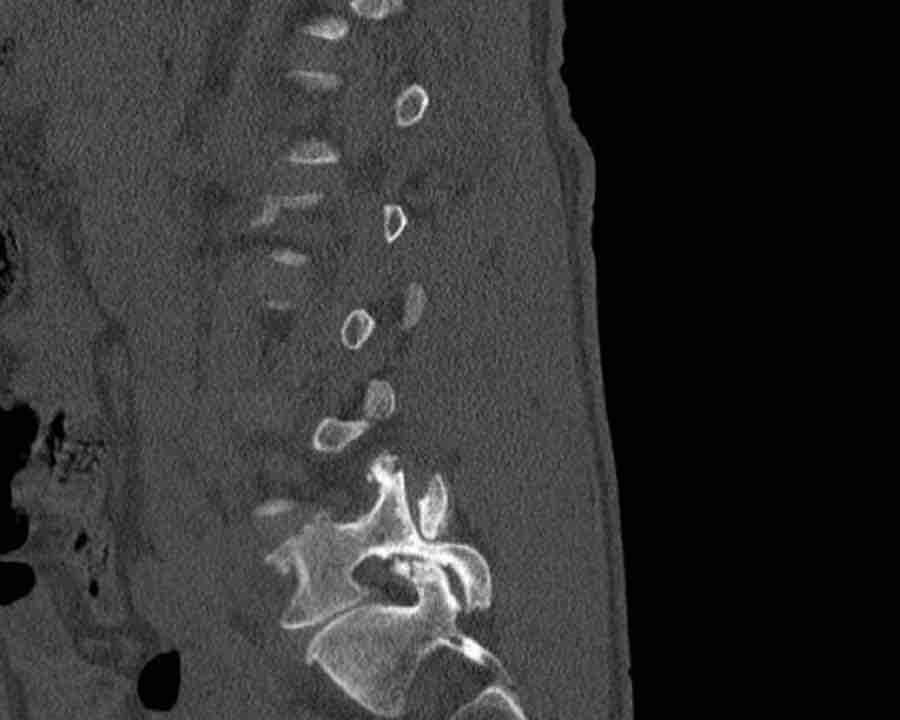
Scroll through images.
What are the findings?
Findings
- C injury? No.
- Signs of a rigid spine?
Yes, clear example of SpA so be aware of a B3 injury. - Horizontal fracture of vertebral body (white circle)
- Subtle separation anteriorly at the fracture level
Conclusion
injury type B3.

Scroll through images.
What are the findings?
Findings
- C injury? No.
- Signs of a rigid spine?
Yes (DISH), so a B3 injury is very likely. - A subtle fracture on the anterior vertebral body (arrows).
- No separation, probably due to positioning of patient in the scanner
Conclusion
Injury type B3.

Scroll through images.
What are the findings?
Findings
- C injury? No.
- Signs of a rigid spine?
Yes, a B3 injury is very likely. - A subtle fracture on the anterior vertebral body.
Conclusion
Injury type B3.

B1 and B2 Flexion distraction injury
Hyperflexion can lead to distraction of the posterior tension band, which is the term for the combined unit of bones and ligaments that together provide stability.
The posterior tension band is formed by:
- Osseous structures: pedicles, transverse processes, spinous processes.
- Non-osseous structures: ligamentum flavum, inter- and supraspinosum, and the facet joints.
When the posterior tension band is distracted in flexion distraction injury, it is classified as:
- B1 flexion injury, which is purely osseous.
This injury is a synonym for the previously called Chance fracture.
B1 injury is rare, since ligamentous structures are almost always involved. - B2 injury, which is a combination of osseous and non-osseous injury. Combination with type A injury is common, this is classified additionally.

Study the images.
What is the highest AO-type of injury?
Any additional findings?
Findings
- Fracture through spinous process indicating B2-flexion distraction injury.
- Fracture of both endplates (1+1 point) and posterior wall (2 points) of the vertebral body, i.e. A4 compression fracture.
Conclusion
injury type B2-A4

Scroll through the images.
What is the highest AO-type of injury?
Any additional findings?
Then continue with the next images...
Findings
- Black arrows: horizontal fractures through the pedicles as a result of flexion distraction trauma.
- White arrows: soft tissue swelling indicating injury to posterior ligaments.
- Circle: compression fracture of posterior wall (2 points) and two endplates (2 points)
Conclusion
Type B2-A4
Flexion distraction injury with separation on the posterior side and a secondary burst fracture involving both endplates and the posterior wall.
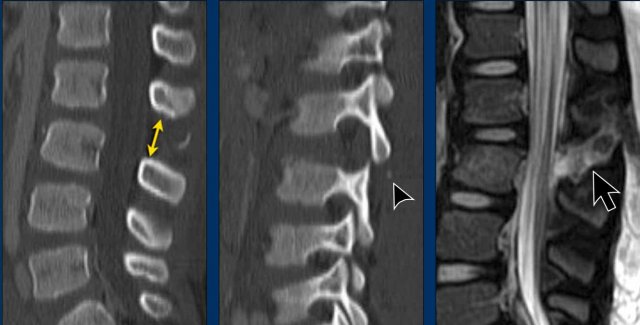
These images are of a young child with a spinal injury.
Findings
- Clear widening of the interspinous distance (yellow arrow)
- Black arrowhead: small avulsion fracture to the flexion distraction
- MRI better depicts the ligamentous injury, which was suspected on CT
Conclusion
Injury type B2

Scroll through the images.
What is the highest AO-type of injury?
Any additional findings?
Findings
- Subtle widening of the interspinous distance (white circle)
- Small avulsion fracture spinous process (yellow arrow)
- Compression fracture with involvement of one endplate and posterior wall (1+2 points)
Conclusion
Injury type B2 + A3
Type A / Compression injury

If it is not a type C or B injury, then the next question is, whether it is a type A compression injury.
Compression injuries are fractures of the vertebral bodies and are classified as:
- A1 fracture of one endplate.
- A2 split fracture where both endplates are involved.
- A3 incomplete burst fracture, where the posterior wall and one endplate are involved
- A4 complete burst fracture, where the posterior wall and both of the endplates are involved.
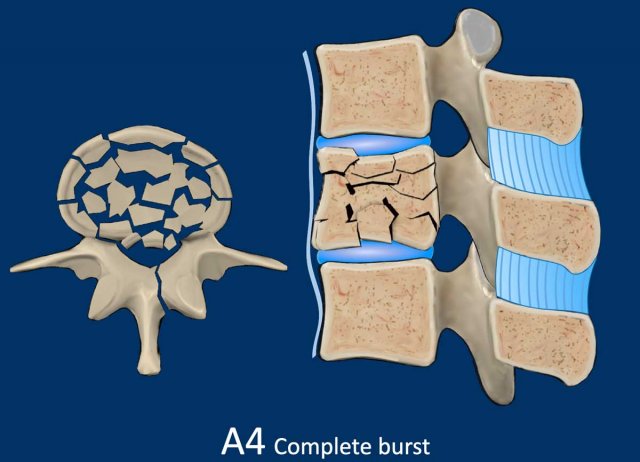
A4 Complete Burst fracture
Fracture with involvement of the posterior wall and both endplates.
A vertical fracture of the lamina can be present and does not constitute a tension band failure.
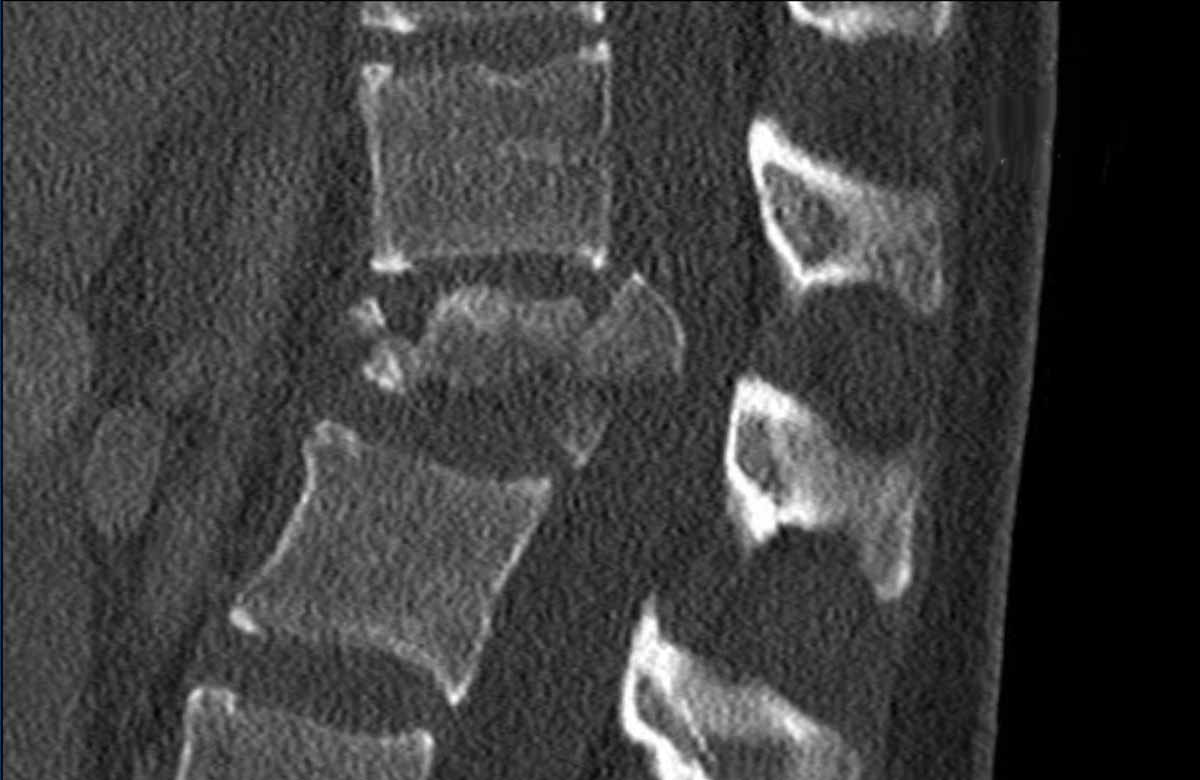
What is the highest AO-type of injury?
Findings:
- No C or B injury
- Fractures of the vertebral body with involvement of both endplates (1+1 points) and posterior wall (2 points)
Conclusion
Injury type A4

What is the highest AO-type of injury?
Findings
- This is a flexion distraction injury type B2.
- There is an additional compression fracture.
What type of A fracture do we have here?
Findings
- Compression fracture of posterior wall (2 points) and two endplates (2 points).
- This is the same case as in the B2 Flexion distraction injury.
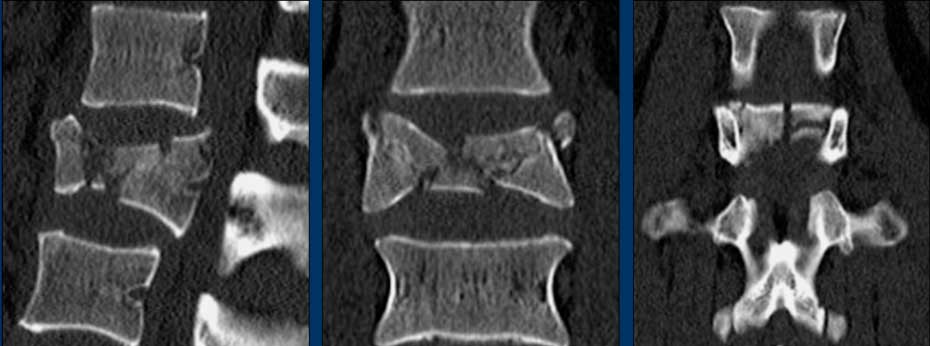
What is the highest AO-type of injury?
Findings
- No C or B injury.
- Fractures of the vertebral body with involvement of both endplates (1+1 points) and posterior wall (2 points).
- In the coronal plane, a sagittal course of the fracture is seen, which is common in burst fractures.
- Bulging of the posterior wall without any other signs of dislocation is the result of the burst fracture.
Therefore no C injury.
Conclusion
Injury type A4
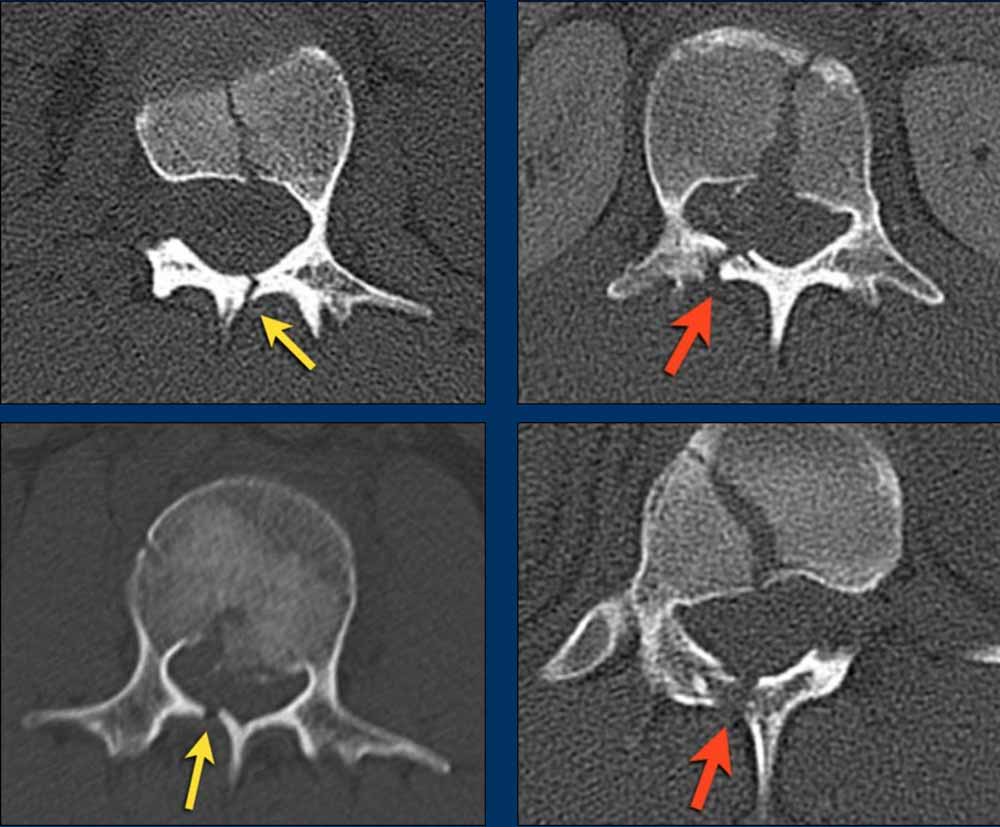
Here more examples of typical burst injuries.
Due to the axial force, the vertebral body is 'split in half', therefore a sagittal course of the fracture is common.
Therefore a fracture through the posterior osseous structures is possible in some type A injuries and should not always be regarded as a posterior distraction injury.
This can be confusing sometimes.
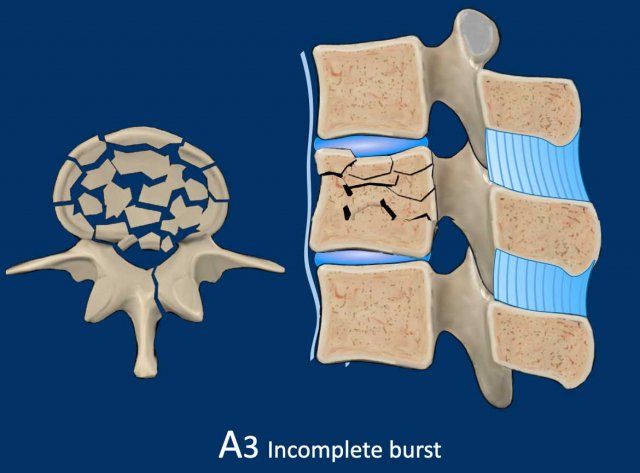
A3 Incomplete Burst fractures
Fracture with any involvement of the posterior wall; only a single endplate fractured.
A vertical fracture of the lamina is usually present and does not constitute a tension band failure.
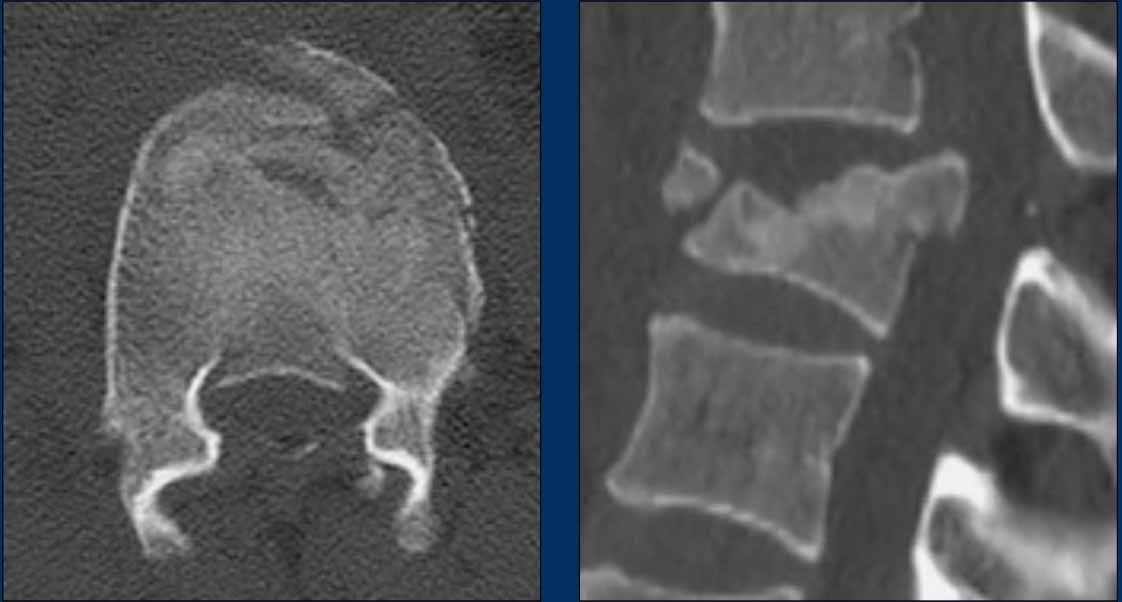
What is the AO-type of the vertebral body fracture based on only these two inages?
Findings:
- Fractures of the vertebral body with involvement of upper endplates (1 points) and posterior wall (2 points)
- Bulging of the posterior wall without any other signs of dislocation is the result of the burst fracture.
Therefore no C injury.
Conclusion
Injury type A3
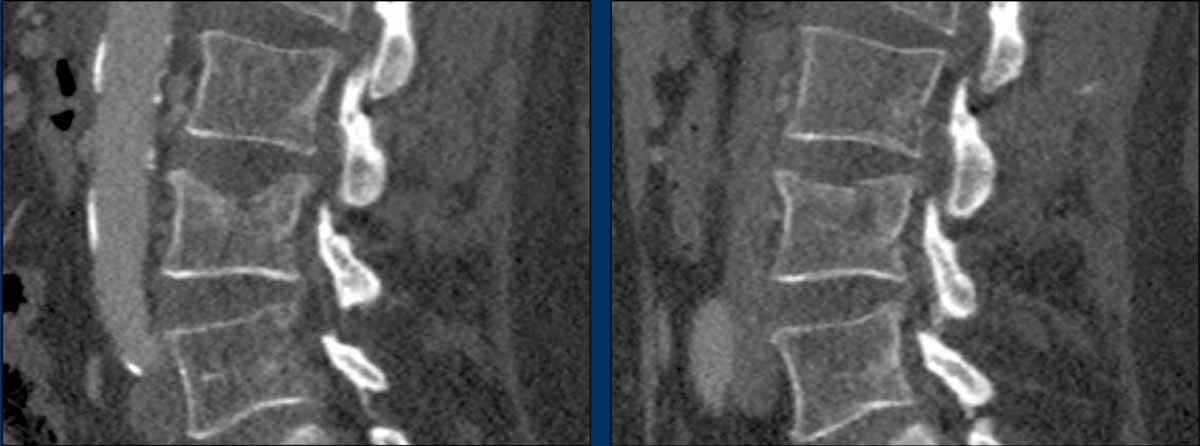
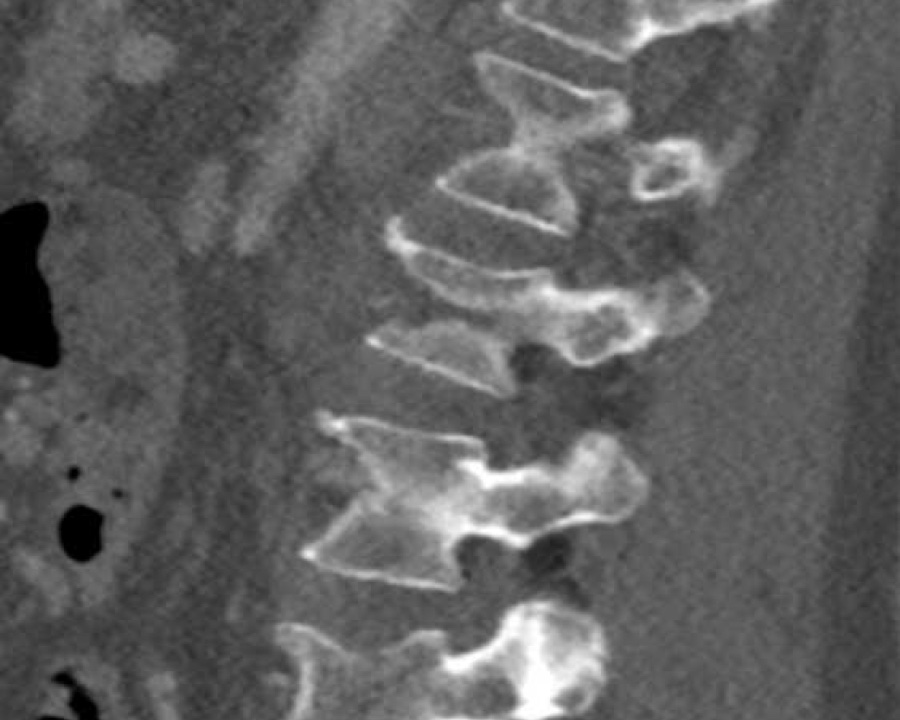
Findings:
- No C or B injury
- Fractures vertebral body with involvement of upper endplate (1 point) and posterior wall (2 points)
Conclusion
Injury type A3

A2 Split fracture
A2 is a fracture of both endplates without involvement of the posterior wall of the vertebral body.
What is the highest AO-type of injury?
Findings:
- No C or B injury
- Fracture of the vertebral body with involvement of both endplates (1+1 points), no posterior wall involvement
Conclusion
injury type A2
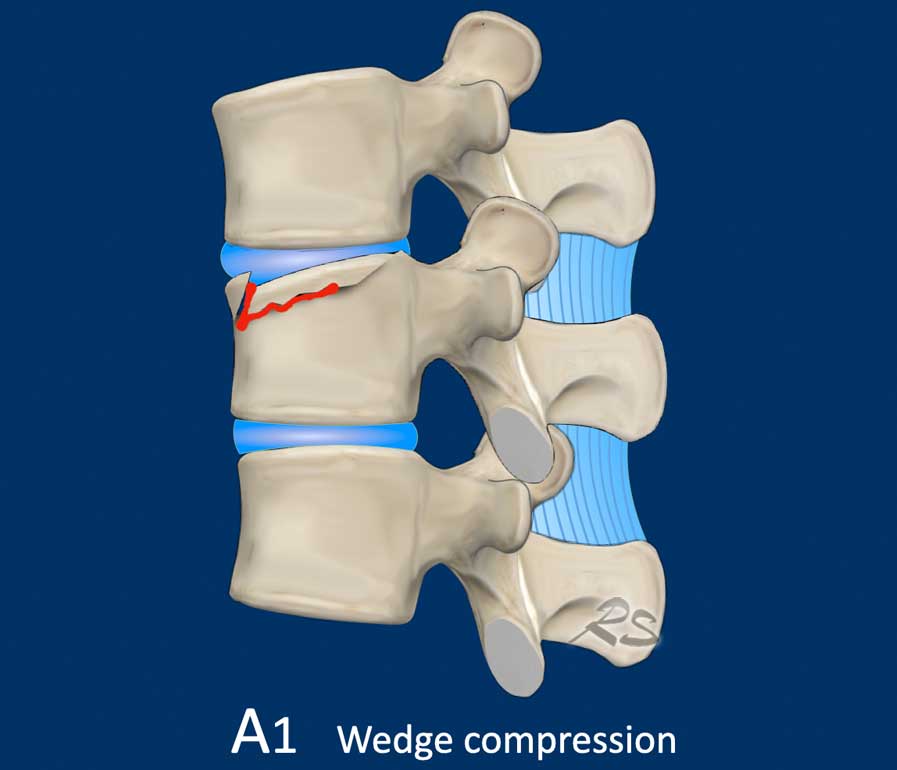
A1 Wedge fracture
Fracture of a single endplate without involvement of the posterior wall of the vertebral body.
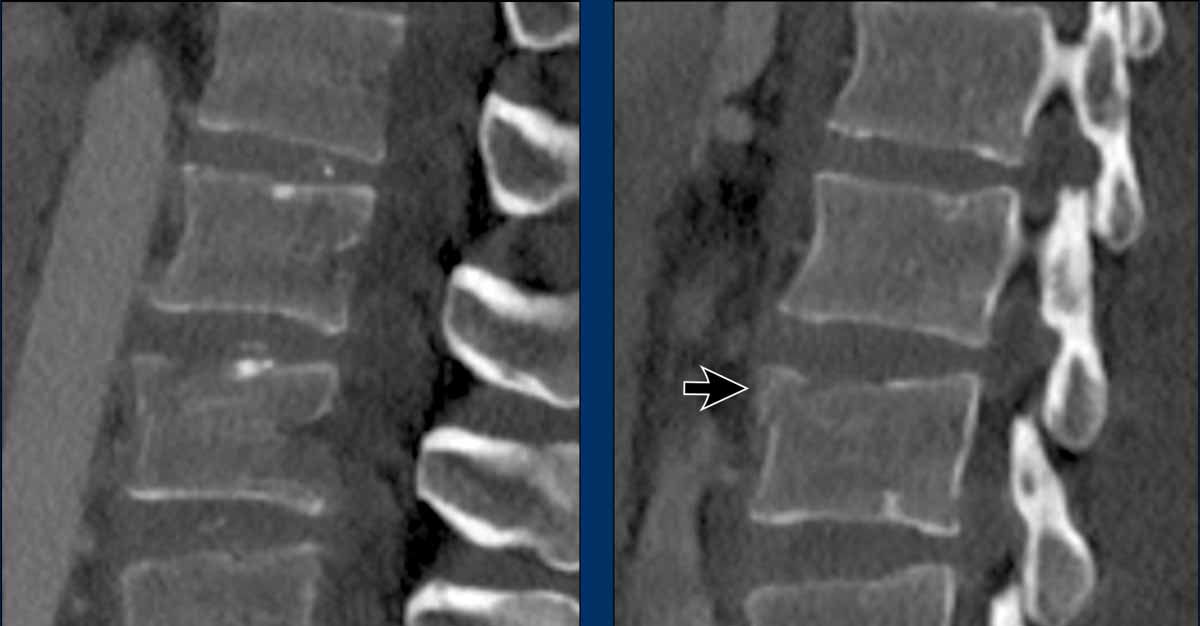
What is the type of the fracture of the vertebral body?
Findings:
- Fracture vertebral body with involvement of upper endplate (1 point), no posterior wall involvement
Conclusion
Injury type A1
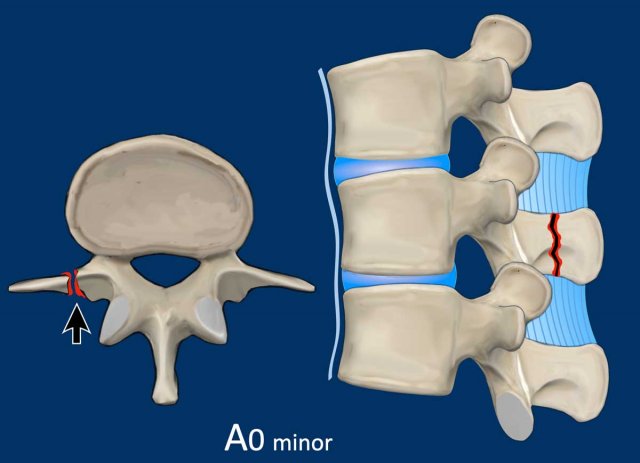
A0 Minor fracture
A0 is a minor non-structural fracture, that does not affect the stability of the spine.
A fracture of the transverse process or spinous process is regarded as an injury type A0.
Usually they are cause by direct trauma.
Modifiers
M1 modifier is when there is uncertainty concerning discoligamentous injury.
M2 modifier describes patient-specific comorbidity, which might argue
either for or against surgery for patients with relative surgical indications.
Example of an M2 modifier are ankylosing spondylitis and Osteoporosis