BI-RADS v2025 Manual - Mammography.
Updated version
Laura Schijf¹ and Robin Smithuis²
¹Radiology department of University Medical Center Amsterdam and ²Alrijne Hospital, Leiden, the Netherlands
Publicationdate
This article summarizes the updated mammography section of the BI-RADS®, v2025 Manual.
We encourage all breast imaging professionals to consult the illustrated BI-RADS® Atlas for comprehensive understanding and correct application of the system.
Mammography Lexicon
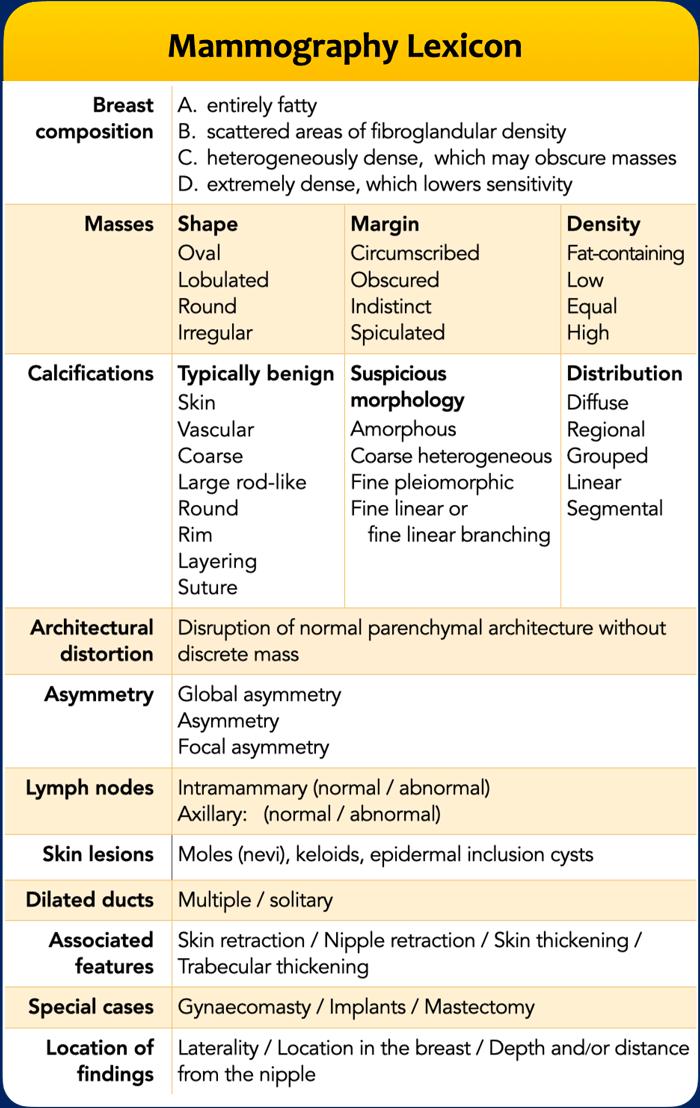
The BI-RADS (Breast Imaging Reporting and Data System) Mammography Lexicon is a standardized terminology developed by the American College of Radiology (ACR) to describe mammographic findings consistently.
It is widely used in radiology reports to ensure clear communication between radiologists and referring physicians.
Purpose of BI-RADS Lexicon
- Standardizes reporting
- Facilitates communication
- Guides management recommendations
- Enables data collection and research
The table summarizes breast density and the description of significant findings, which are the key elements used to determine the final assessment category of the breast examination.
These topics will be addressed in detail in the subsequent chapters.
The updated BI-RADS® v2025 Manual, provides a highly detailed description with numerous mammographic examples.
In this article, we limit our discussion to a concise summary.
Standard Reporting
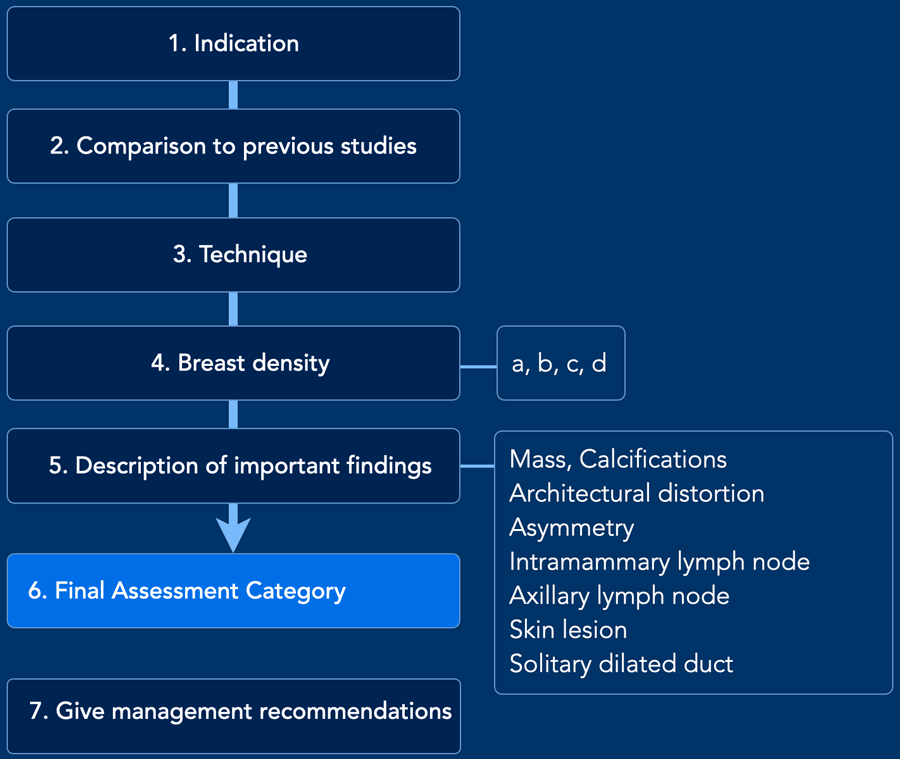
- Indication
Asymptomatic screening
(Subcategory: elevated risk, dense breasts)
(Relevant history: Gene mutation, prior breast cancer)
Diagnostic work up
(Subcategory: clinical findings, follow up category 3, follow up after biopsy, implant assessment)
Diagnostic current cancer
(Extent of disease before treatment, response to neoadjuvent therapy) - Comparison
Mention the dates of comparison examinations. First mammogram is called "baseline". - Technique
Digital mammography (DM), Digital breast tomosynthesis (DBT), supplemental tools used (CAD or AI), CEM. - Density
- Findings
- Final assessment
- Mangement recommendations
Category 0 include suggestions for next course of action
Category 1-2 continue or resume screening at appropriate interval
Category 3 recommend follow up
Category 4-5 biopsy. Include recommended method of tissue diagnosis, (e.g., stereotactic, ultrasound or MR guided biopsy)
Breast density
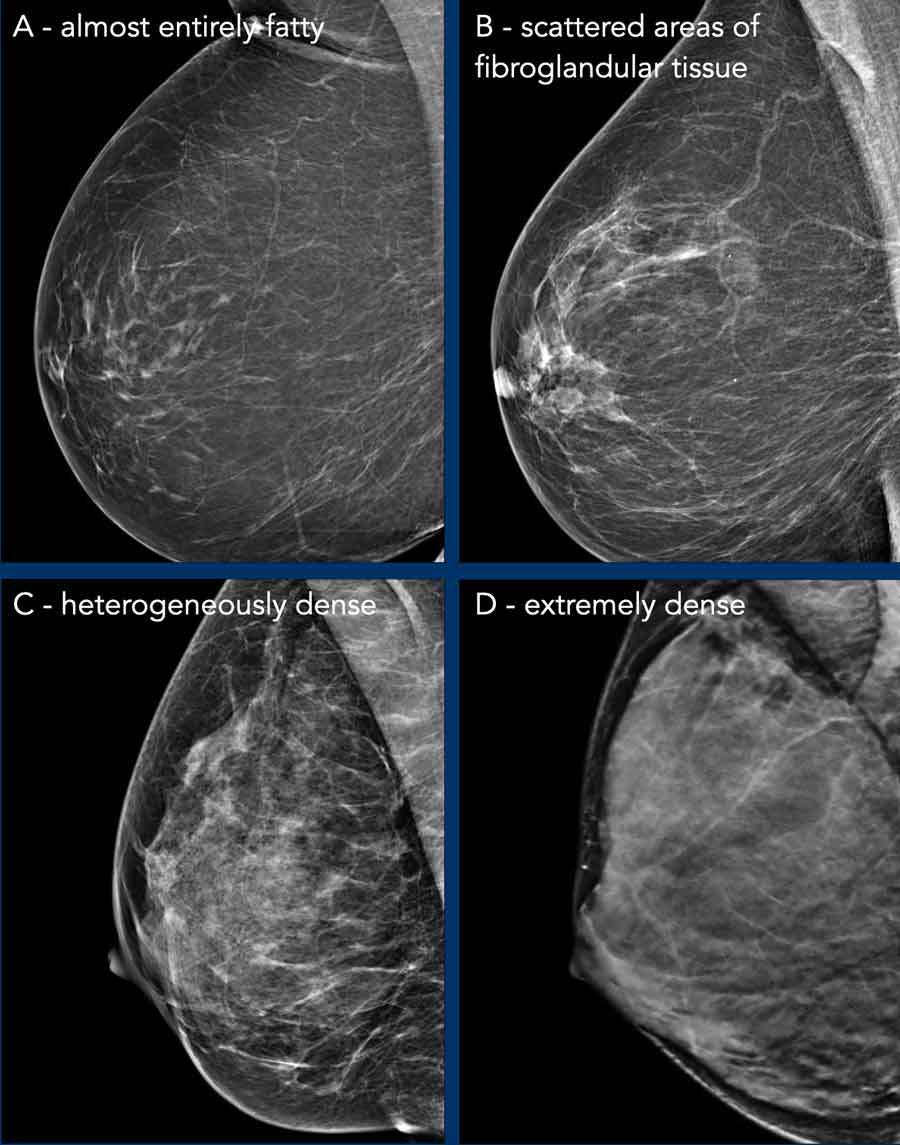
Breast density is classified into four categories (A–D), each accompanied by a descriptive summary (if breasts differ in density, the higher category is recorded):
- A. Almost entirely fatty: Mammography is highly sensitive in this setting.
- B. Scattered areas of fibroglandular density
- C. Heterogeneously dense: Some areas of the breasts are sufficiently dense to obscure small masses.
- D. Extremely dense: which lowers the sensitivity of mammography.
Breast density is clinically relevant for two reasons:
- Mammographic accuracy: Dense fibroglandular tissue reduces mammographic sensitivity due to masking effects.
- Breast cancer risk: High breast density is an independent risk factor for breast cancer. Compared to women with scattered fibroglandular density (category B), those with extremely dense breasts have an increased risk (odds ratio: 1.6), while predominantly fatty breasts are associated with a lower risk (odds ratio: 0.6). However, the masking effect caused by dense breast tissue has been reduced bij advances in technology, first with digital mammography, and more recently with DBT. In women with dense breasts, the cancer detection rate increased from 4,5 per 1000 woman screened with DM to 5.8 per 1000 women screened with DBT.
The European Society of Breast Imaging (EUSOBI) has recently stated that MRI should be considered instead of mammography for women with dense breasts.
Masses
A mass is defined as follows:
- 3-dimensional, space-occupying structure
- completely or partially convex margin
- when radiodense, appears denser in the center than at the periphery
- may be apparent on a single projection or when imaged on DBT
Characteristics of a Mass:
- Shape: Oval, lobulated, round or irregular.
- Margins: Circumscribed, obscured, indistinct or spiculated.
- Density: Fat-containing, low, equal or high
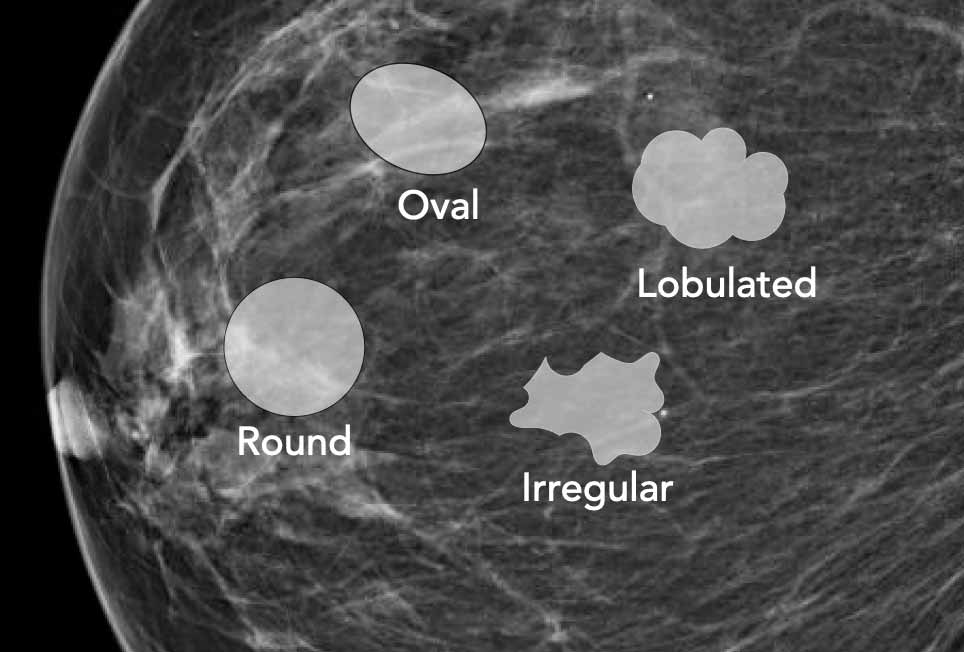
Shape
Oval
- Elliptical or egg-shaped, longer in one dimension.
- Typically benign (e.g., fibroadenomas, lymph nodes).
- Orientation parallel to the skin surface is more reassuring.
Lobulated (new descriptor)
- A lobulated mass exhibits one or more indentations, resulting in an undulating contour.
- Although usually benign, it is considered slightly more suspicious than an oval mass. This shape descriptor adds nuance to the assessment of mass morphology.
- Can be seen in both benign (e.g., fibroadenomas) and malignant lesions (e.g., invasive ductal carcinoma).
Round
- Spherical or circular.
- Most commonly benign (e.g., cysts, fibroadenomas).
- Rarely, some malignant lesions (e.g., medullary carcinoma) may also appear round.
Irregular
- Numerous angular or deep lobulations.
- Highly suspicious for malignancy. Often associated with spiculated margins and architectural distortion.
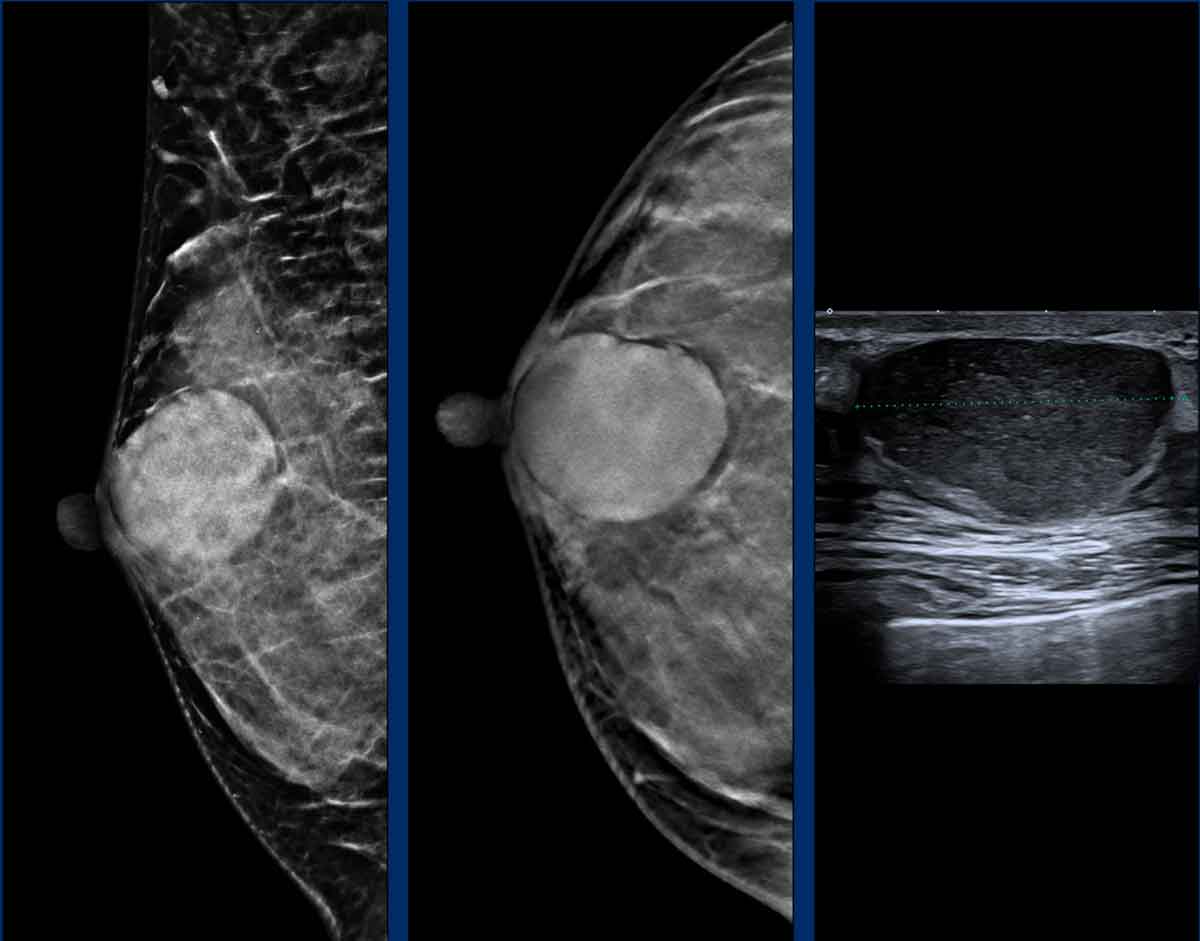
Imaging Example:
- Mammography (DM, DBT): Oval, circumscribed, high-density mass.
- Ultrasound: Oval, parallel, circumscribed mass.
Pathology Diagnosis: Fibroadenoma
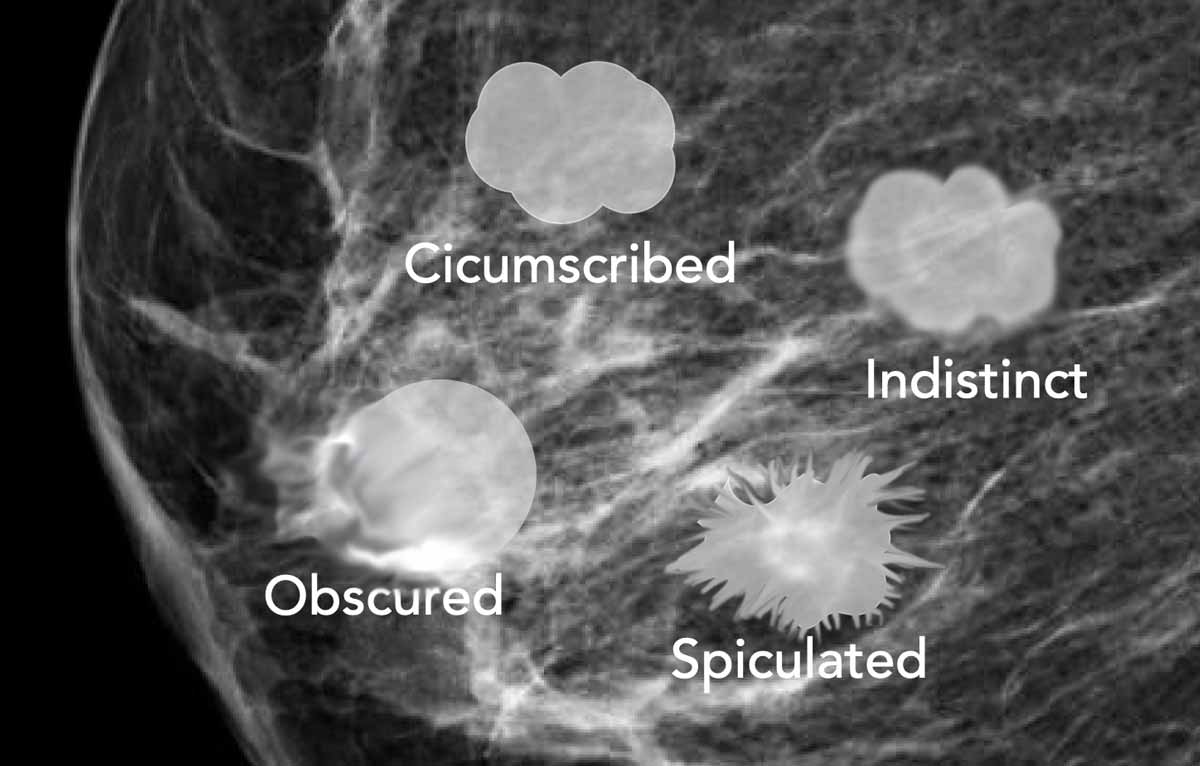
Margin
When possible, the margin of a mass should be characterized on breast tomosynthesis due to reduced tissue superposition compared to mammography.
Circumscribed (Well-Defined)
- Sharp, distinct borders, abrupt transition between mass and surrounding tissue. If part of the margin is obscured, but at least 75% circumscribed, the margin is described as circumscribed. If any part of the margin is indistinct or spiculated, it is described as indistinct or spiculated.
- Typically associated with benign lesions (e.g., cysts, fibroadenomas).
- Some malignant lesions (e.g., invasive ductal carcinoma, medullary carcinoma) may also present with circumscribed margins.
Obscured
- Partially hidden by surrounding dense fibroglandular tissue.
- Requires further evaluation (e.g., additional imaging with spot
compression views, DBT, ultrasound) to clarify the lesion’s nature.
Indistinct
- Poorly defined, blending into surrounding tissue. Suspicious; may indicate infiltrative growth patterns.
Spiculated
- Radiating lines from the lesion. Highly suggestive of malignancy (e.g., invasive ductal carcinoma, tubular carcinoma).
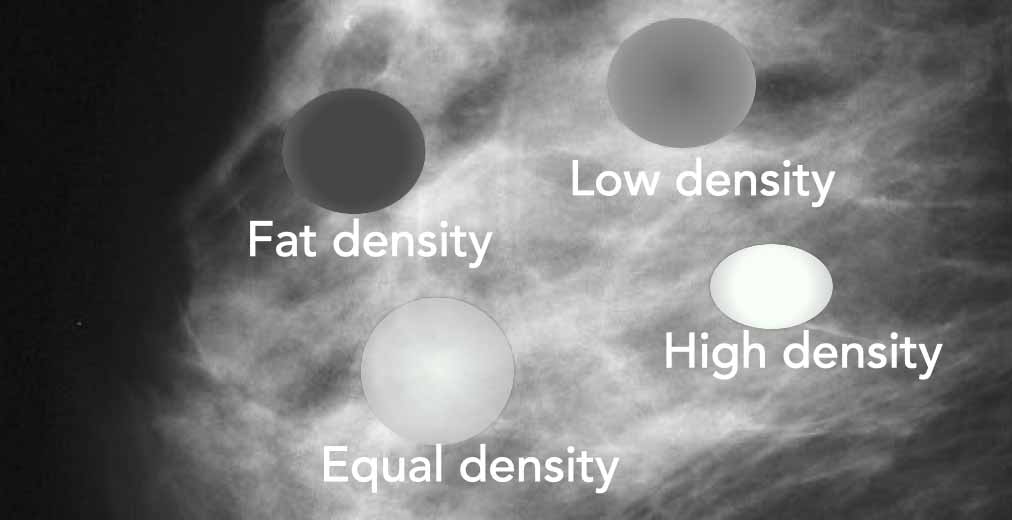
Density
The density of a mass is compared to surrounded normal fibroglandular tissue.
- Fat-containing
Most fat-containing masses are benign (lipoma, oilcyst and hamartoma). Fat within malignant lesions is rare and is the result of entrapped fat. - Low-density
- Equal density
Equal to surrounded fibroglandular tissue. - High density
High density masses have a high likelihood of malignancy (70%).
Example
Multiple round, circumscribed, low-density masses are present in the right breast.
These findings are consistent with prior lipofilling, which refers to autologous fat grafting of the breast.
Classification
BI-RADS 2
 Click on image to enlarge
Click on image to enlarge
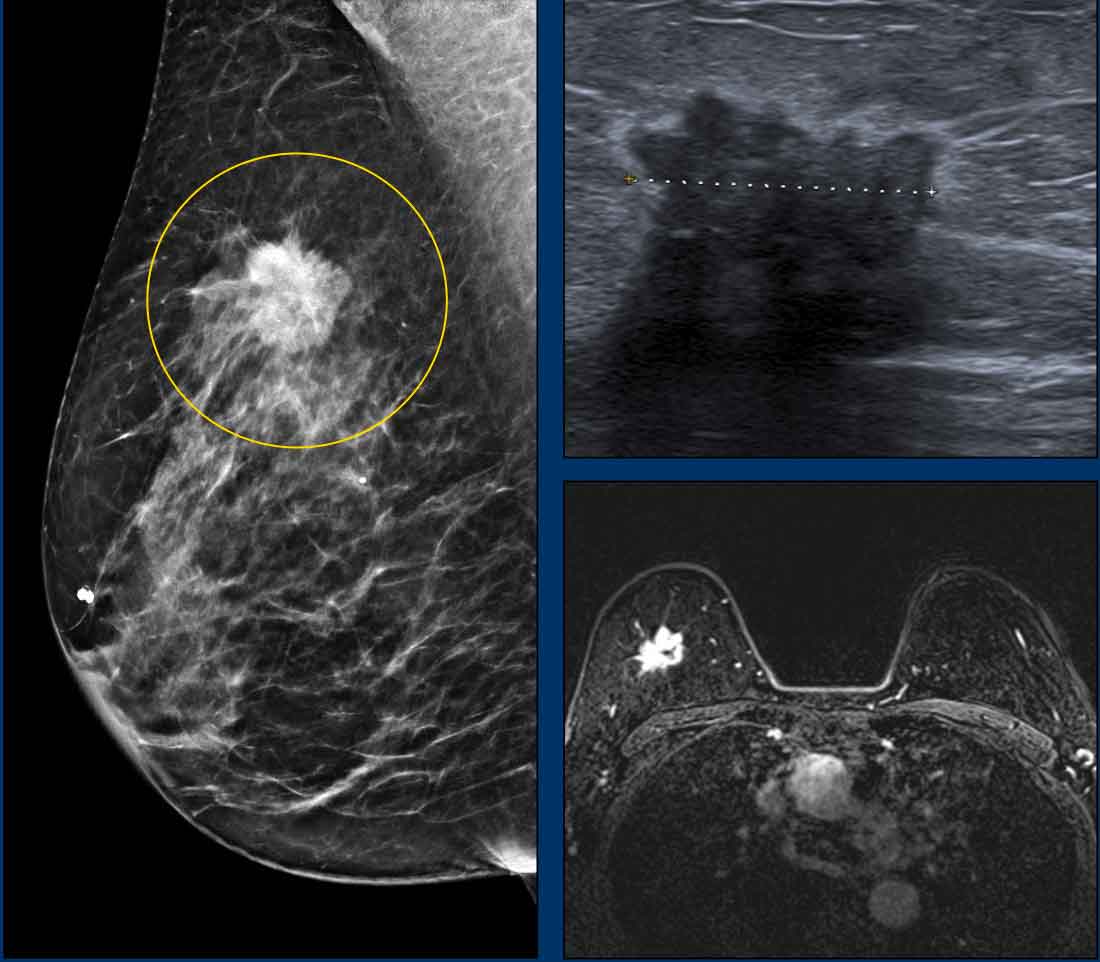
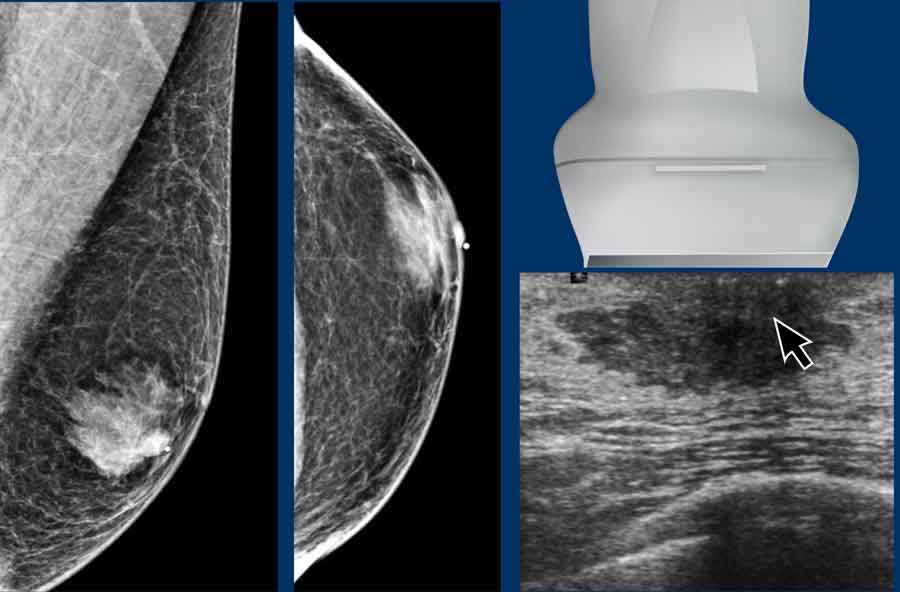
Example
Mammography
- High density mass
- Shape: irregular
- Margin: spiculated (enlarge image to see the spiculae)
- BI-RADS 4
Ultrasound
- Hypoechoic mass with echogenic rim
- Shape: irregular
- Posterior shadowing
- Horizontal orientation
MRI
- Fat-suppressed early post-contrast T1W image.
Irregular, spiculated, heterogeneous mass.
Pathology
Invasive ductal carcinoma
Calcifications

Intralobular Calcifications
- Found within the lobules (the milk-producing glands) of the breast.
- Often appear as small, round, or punctate calcifications, sometimes clustered in a lobular distribution.
- Typically associated with benign conditions such as fibrocystic change, adenosis, or lobular carcinoma in situ (LCIS). However, they can occasionally be seen in invasive lobular carcinoma or ductal carcinoma in situ (DCIS) involving the lobules.
- Usually require correlation with clinical history and imaging findings. Biopsy may be recommended if suspicious features are present.
Intraductal Calcifications
- Located within the ducts of the breast, often following the ductal tree.
- Typically linear, branching, or casting in shape, reflecting the ductal anatomy. They may appear as fine, granular, or pleomorphic calcifications.
- Strongly associated with ductal carcinoma in situ (DCIS), especially when they are linear, branching, or clustered. These calcifications are often the earliest sign of DCIS.
- Stereotactic biopsy or surgical excision is usually recommended for definitive diagnosis.
 Click on image to enlarge
Click on image to enlarge
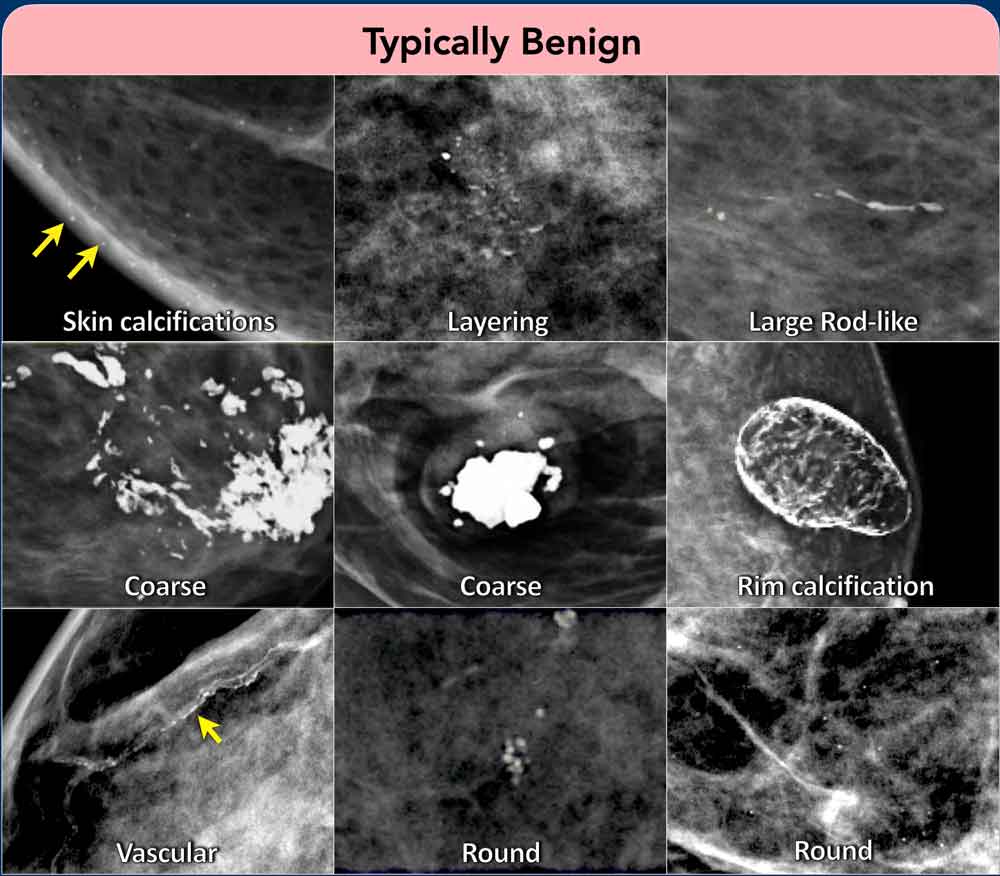
Typically benign calcifications
Benign calcifications are typically larger, coarser, rounder and more conspicuous than malignant calcifications.
Skin calcifications: Round or oval, lucent-centered (due to dermal location), superficial, and frequently clustered. No further intervention required.
Vascular calcifications: Linear or tubular, following the course of vessel walls; associated with atherosclerosis.
Coarse calcifications: Large, irregular, flaky in appearance. Classic for involuting fibroadenomas and dystrophic calcifications. The term “popcorn-like” has been removed.
Round calcifications: Small (<0.5 mm), round, uniform dots. Benign; commonly seen in fibrocystic change or post-traumatic settings. The term punctate (< 0.5 mm) has been removed given the impractability to measure the size of individual calcifications).
Large Rod-like: Coarse, irregular, often rod-shaped or curvilinear; may exhibit lucent centers. Associated with fat necrosis, surgery, or trauma.
Suture calcifications: Linear or tubular, aligned with surgical suture lines. Benign; related to prior surgery.
Layering (milk-of-calcium) calcifications: Semilunar or crescentic on medio-oblique or mediolateral views; often indistinct on craniocaudal views. Benign; classic for calcified debris within microcysts.
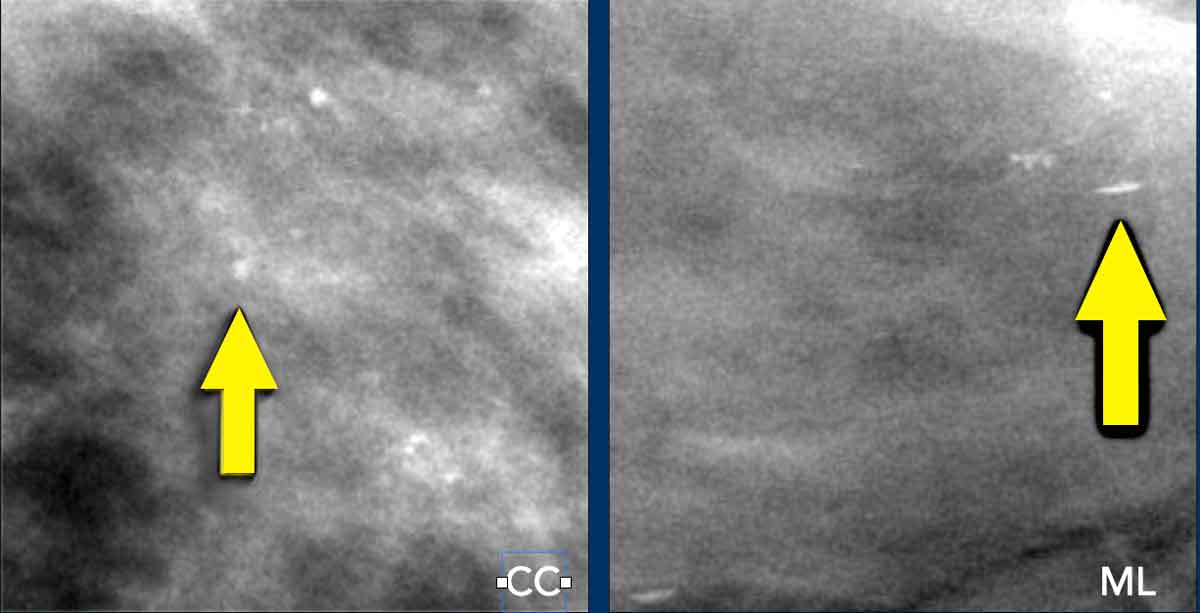
Example Layering calcifications
On the craniocaudal (CC) view, the calcifications appear as round, ill-defined, and less conspicuous deposits.
In the mediolateral (ML) view, characteristic layering is evident, forming semilunar or crescentic shapes.
This pattern is pathognomonic for calcified debris within microcysts.
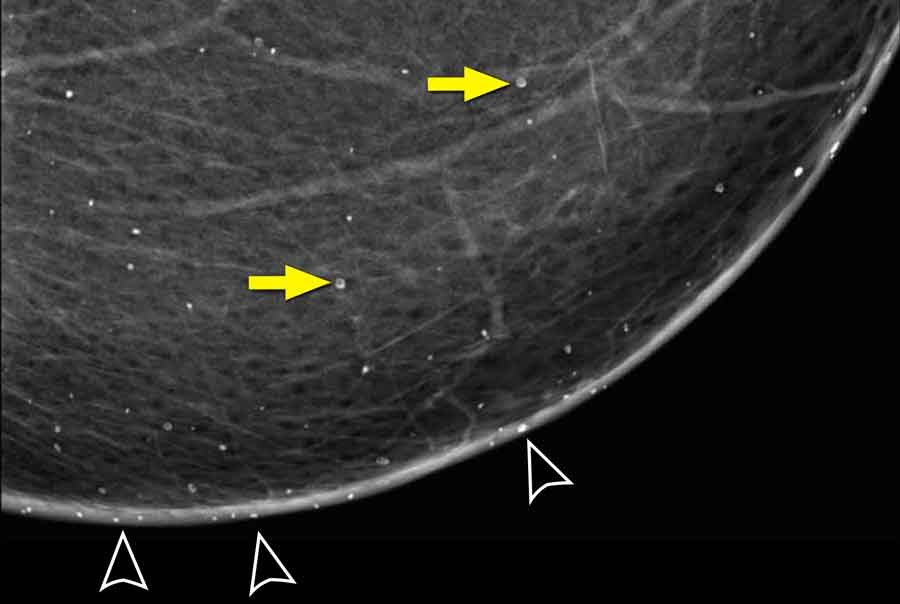
Example Skin calcifications
Whenever you consider the possibility of skin calcifications, always assess for calcifications that project tangentially within the skin plane (arrowheads).
Notice that the calcifications, that appear to be located within the breast, exhibit a lucent center (yellow arrows).
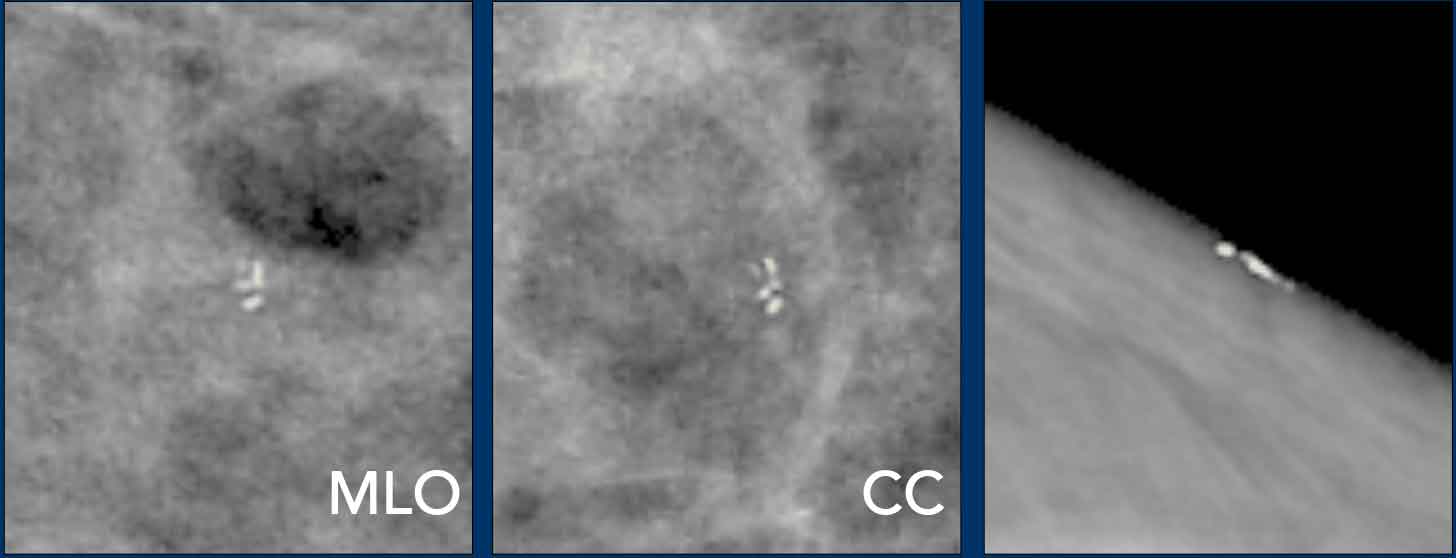
Example Skin calcifications - Tatoo sign
When calcifications are located within the breast tissue, their configuration should differ between the MLO or ML view and the CC view due to the change in projection angle.
However, if calcifications are located within the skin, their configuration remains unchanged across all views.
This can be compared to a tattoo of the number "5" on the skin: regardless of the viewing angle—from above or from the side—the tattoo will always appear as the number "5." This phenomenon is known as the "tattoo sign."
Image
It was observed that the configuration of the calcifications remained identical on both MLO and CC views. Additionally, a tangential view was obtained to confirm the dermal location of the calcifications.
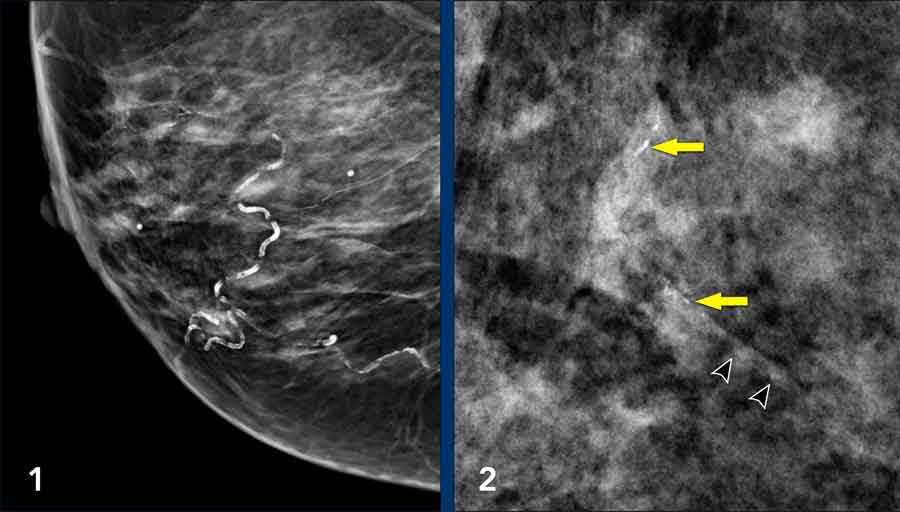
Example Vascular calcifications
Vascular calcifications present as parallel calcific tracks and are usually clearly associated with arteries.
Sometimes better depicted on DBT than DM.
Vascular calcifications are typically bilateral and seen in more than just one isolated area.
Breast arterial calcifications (BAC) is correlated with increased risk of cardiovascular disease.
Images
- Obvious vascular calcifications
- These linear calcifications could easily be described as fine linear. However if you look closely - you may have to enlarge the image - you will notice the vessel (arrowheads)
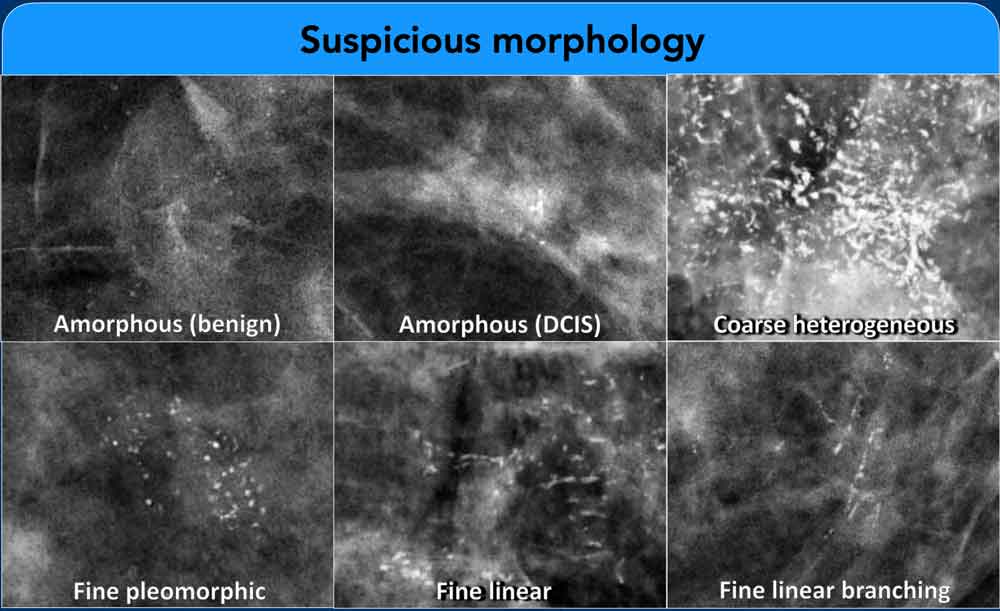
Suspicious calcifications
Amorphous calcifications: Indistinct, hazy, or ill-defined in appearance.
Their "formless" nature precludes assignment of a specific morphology.
Bilateral, diffuse amorphous calcifications are generally considered benign.
Coarse heterogeneous calcifications: Irregular in shape, typically 0.5–1.0 mm in size, with a tendency to coalesce.
They are smaller than typical benign coarse calcifications.
Numerous bilateral groups are usually regarded as benign.
Fine pleomorphic calcifications: Variable in size and shape, generally < 0.5 mm in diameter. These carry a higher likelihood of malignancy compared to amorphous or coarse heterogeneous calcifications.
Fine linear or fine-linear branching calcifications: Thin, irregular lines, often following ductal distributions and occasionally branching. These have the highest likelihood of malignancy.
Risk Stratification:
- Amorphous, coarse heterogeneous, and fine pleomorphic calcifications are associated with a lower risk of malignancy and are typically assigned to BI-RADS category 4B.
- Fine linear or fine-linear branching calcifications, due to their higher malignancy risk, are assigned to BI-RADS category 4C.
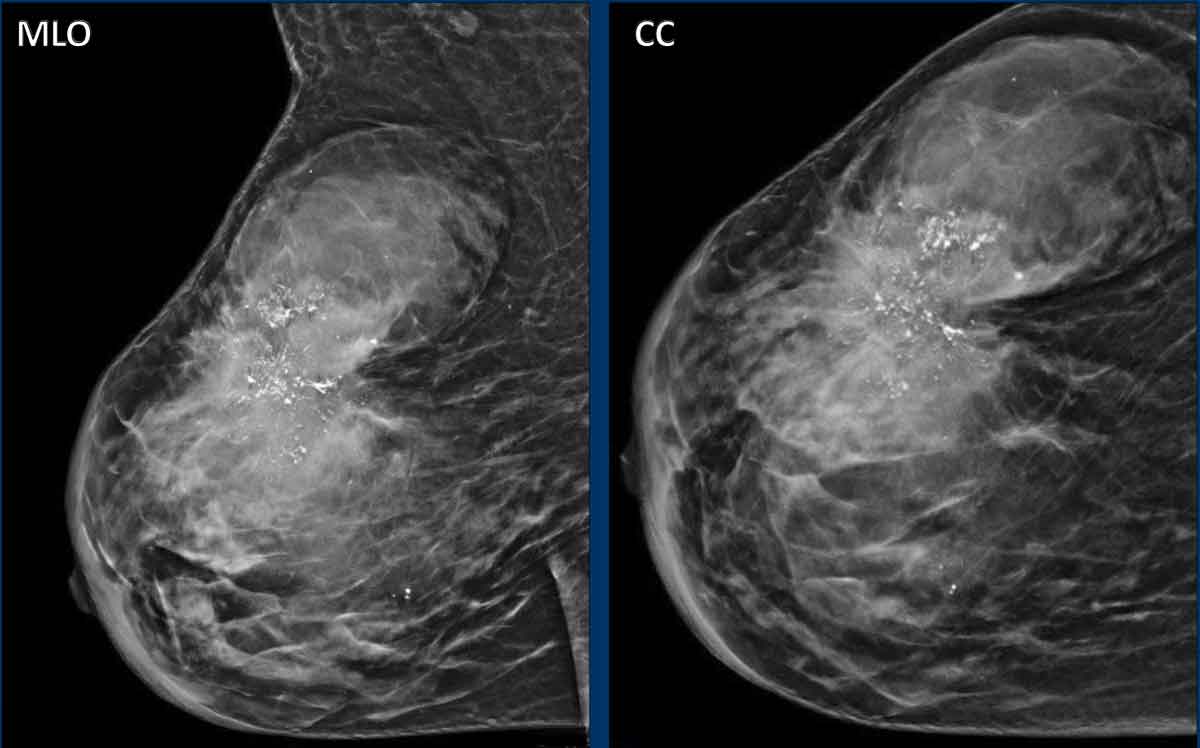
Example
- Irregulair indisctinct mass
- Fine pleomorf, fine lineair calcifications and also coarse heterogeneous calcifications
- Associated skin thickening and retraction of fibroglandular tissue
Pathology
Invasive
ductal carcinoma and DCIS grade 2.
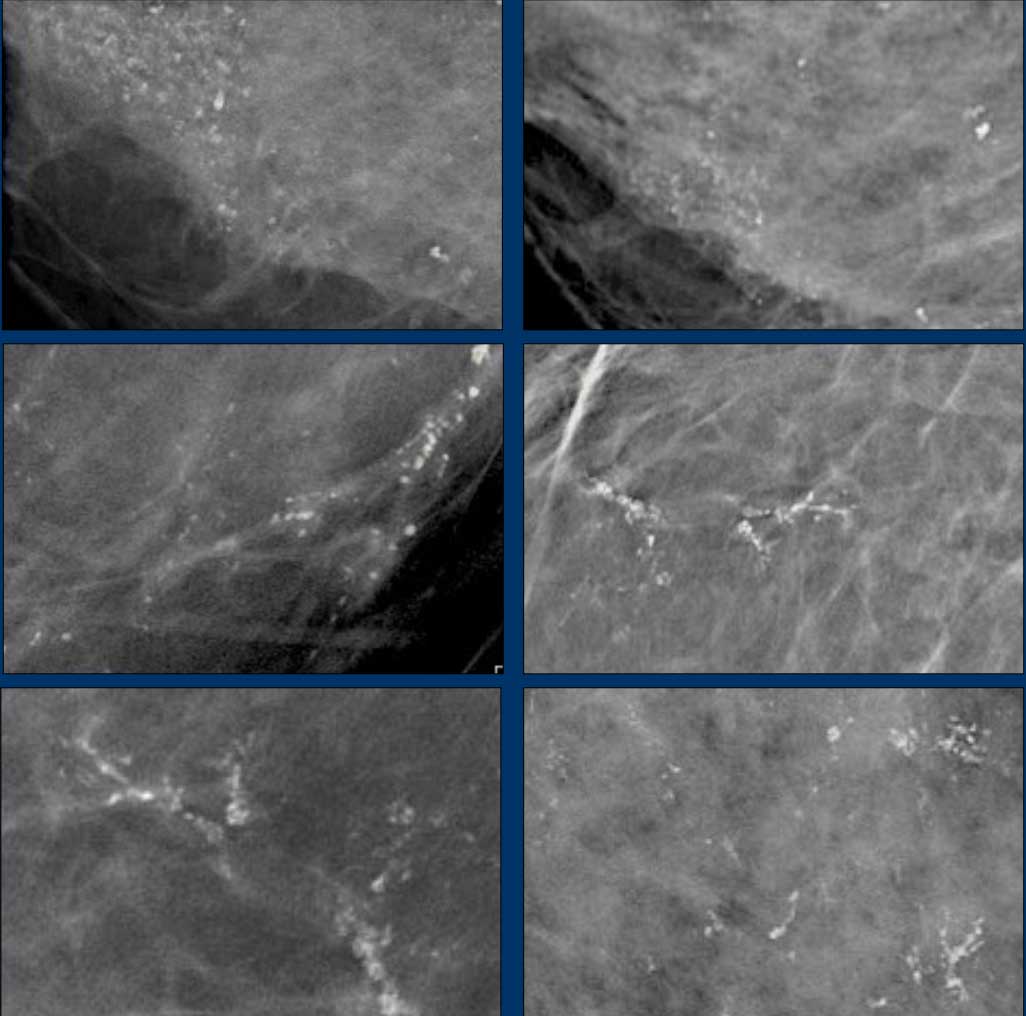
These images are from six different patients, all of whom were diagnosed with ductal carcinoma in situ (DCIS).
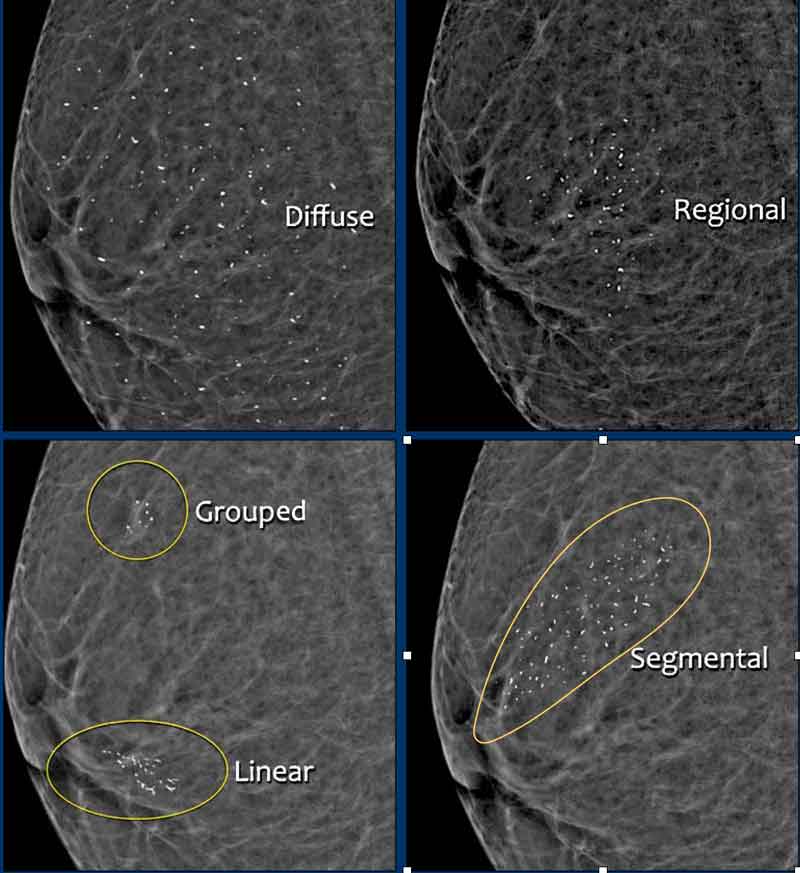
Distribution of calcifications
The distribution of calcifications is as important as their morphology.
Descriptors are organized according to malignancy risk:
- Diffuse: Calcifications are randomly distributed throughout the breast. Diffuse bilateral round and amorphous calcifications are almost always benign. Unilateral diffuse calcifications are uncommon and may be due to diffuse ductal carcinoma in situ (DCIS), particularly if the calcifications are coarse heterogeneous, fine pleomorphic, or fine linear branching.
- Regional: Calcifications occupy a large portion of breast tissue (greater than 2 cm in greatest dimension) but do not involve the entire breast, as seen with diffuse calcifications. The calcifications are randomly scattered within the region and do not conform to a ductal or segmental distribution. While malignancy is less likely, the level of suspicion is influenced by calcification morphology and laterality (unilateral vs. bilateral).
- Grouped (historically “clustered”): A small, discrete collection of calcifications, typically five or more within 1–2 cm, indicating a non-random distribution. Morphology is more significant than absolute number; biopsy should be considered even if fewer than five calcifications are present, provided they are suspicious.
- Linear: Calcifications are arranged in a line, suggesting deposition within a duct. This pattern carries a higher suspicion for malignancy and must be differentiated from vascular and large rod-like calcifications, which may also appear linear.
- Segmental: Calcifications are arranged in a triangular distribution with the apex pointing toward the nipple. This pattern is highly suspicious, as it suggests deposition within multiple ducts or duct branches, indicating possible extensive or multifocal breast cancer.
 Click on image for an enlarged view
Click on image for an enlarged view
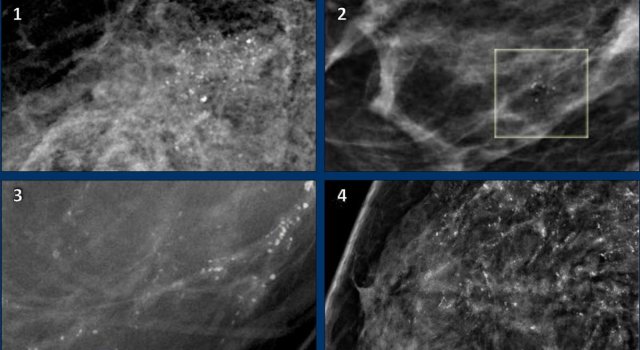
Examples
- Regional calcifications in an area > 2cm
- Grouped calcifications in an area < 2cm
- Linear distribution. PA:DCIS
- Diffuse distribution. The calcifications were distributed throughout the whole breast. They have a suspicious morphology (fine pleiomorphic).
PA: diffuse invasive ductal carcinoma
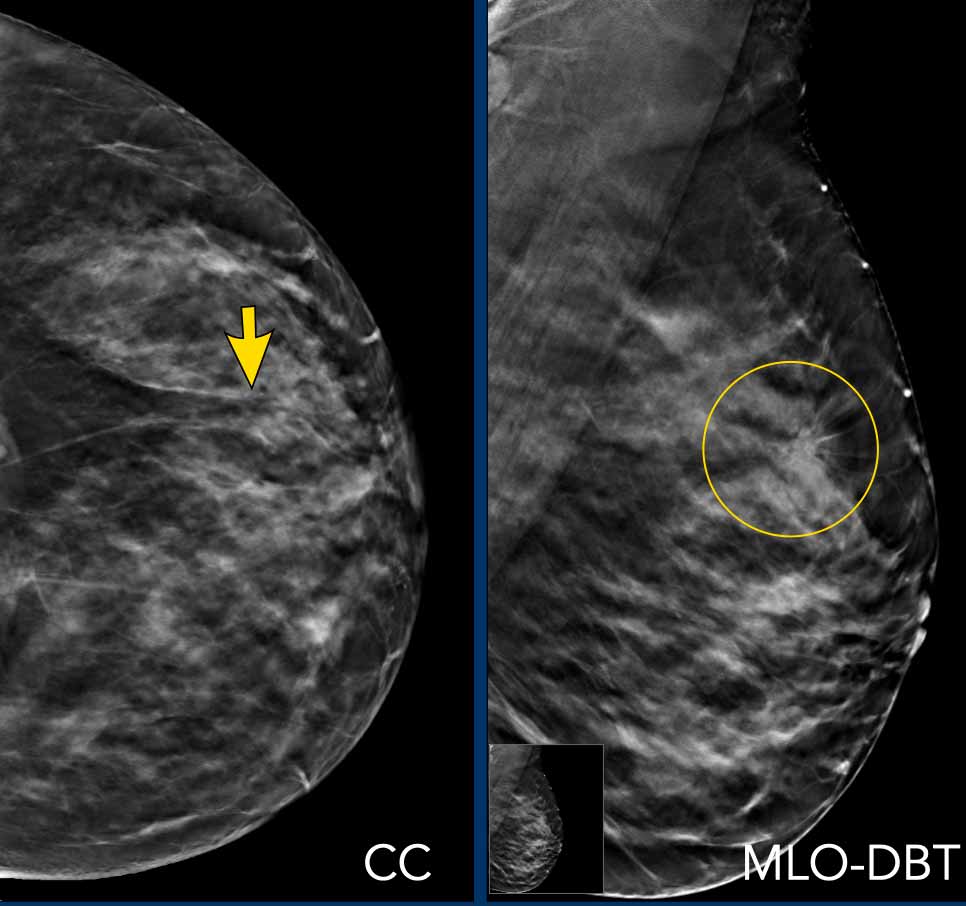
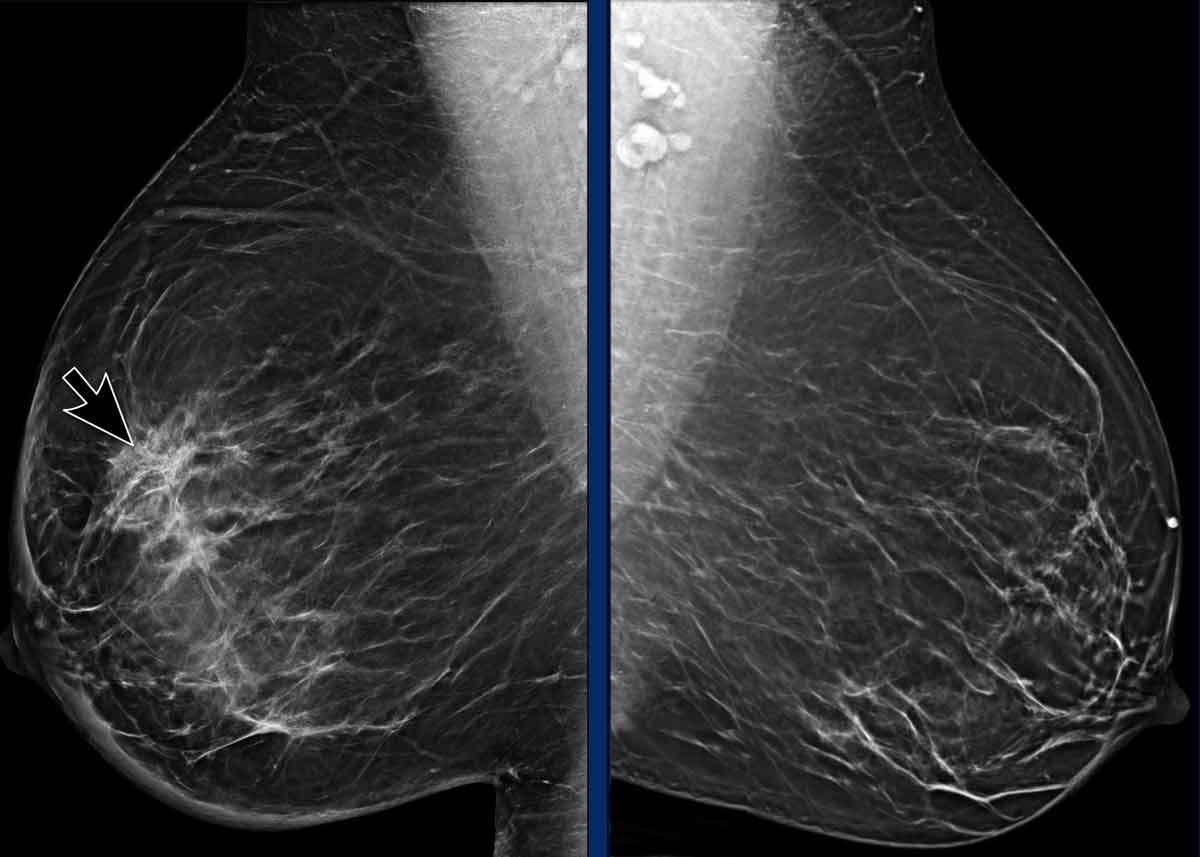
Architectural distortion
Architectural distortion refers to an abnormality in which the normal breast architecture is disrupted without a discrete mass.
This may present as thin, straight lines or spiculations radiating from a central point, as well as focal retraction, distortion, or straightening of the parenchymal margins.
While architectural distortion is more frequently detected on DBT than on DM, its positive predictive value is lower.
Nonetheless, architectural distortion that is clearly visible only on DBT—without a history of trauma or surgery—remains moderately predictive of malignancy.
Tissue diagnosis is therefore warranted, even in the absence of an ultrasound correlate.
Differential Diagnosis
- Post-surgical or post-traumatic scar tissue
- Carcinoma
- Radial scar
Clinical Note
Architectural distortion can also be an associated feature. When a mass is accompanied by architectural distortion, the likelihood of malignancy is higher compared to a mass without distortion.
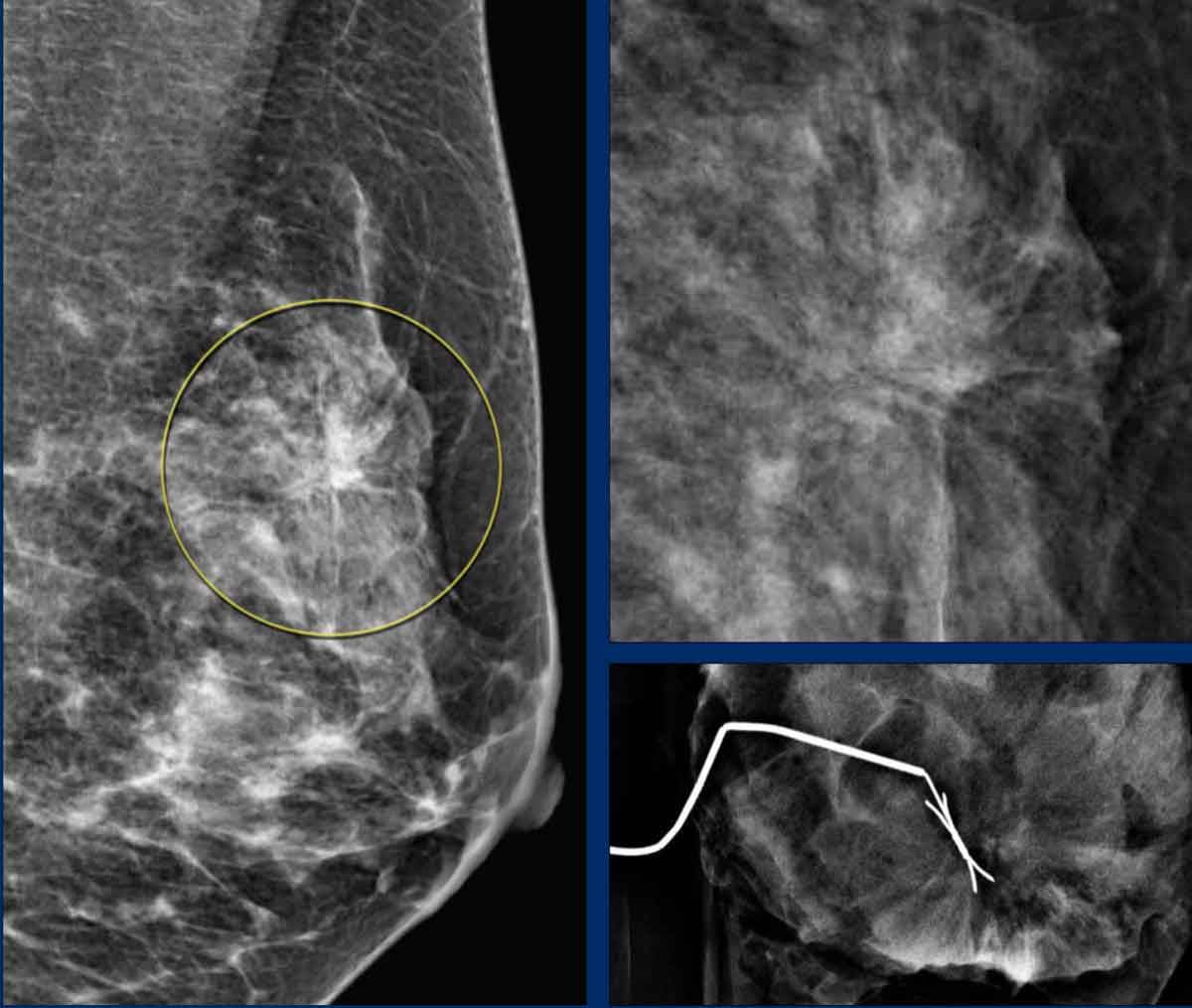
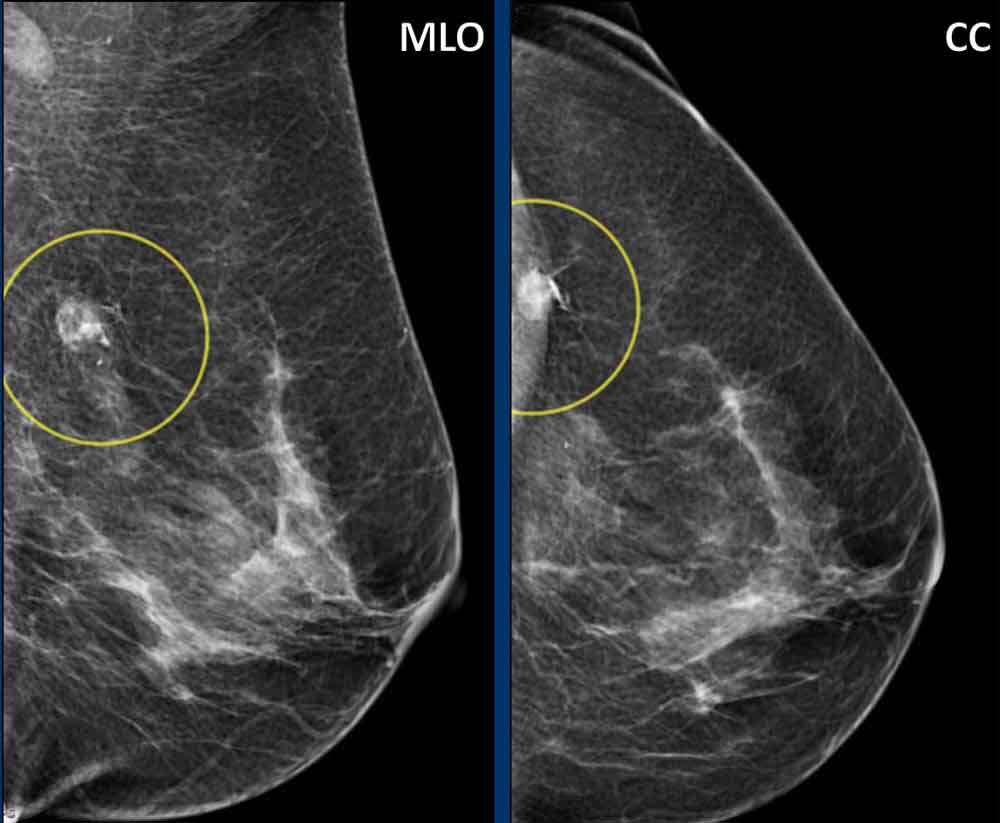
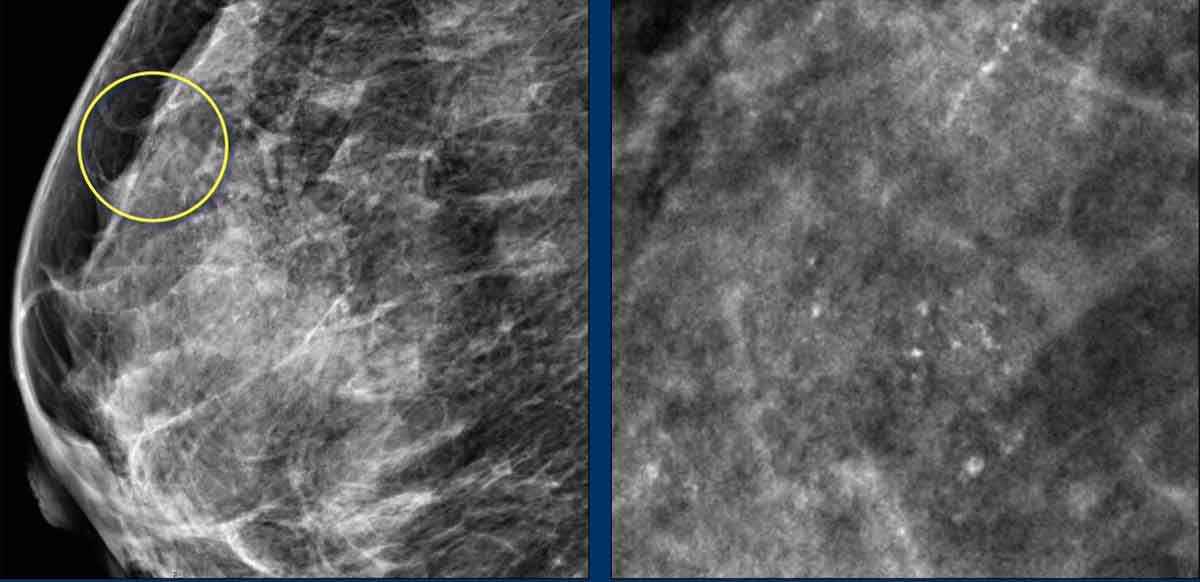
Image Example
Distortion of the normal breast architecture is visible on the mediolateral oblique (MLO) view (highlighted in the yellow circle) and on the magnification view.
Surgical resection revealed scar tissue on histopathology.
Architectural distortion seen on DM and DB.
Pathology
Radial scar
Architectural distortion seen on DM and DBT.
Pathology
Invasive ductal carcinoma
Asymmetry
Asymmetry is a focal area of breast tissue lacking a mirror image in the contralateral breast with concave contours and interspersed fat.
It does not meet mass criteria (radiodense center, convex contour).
Using DBT most asymmetries can be recognized to represent superimposition of normal breast structures and no further imaging is needed.
If a true lesion cannot be excluded, especially if seen on multiple consecutive DBT slices, stereotactic biopsy is needed.
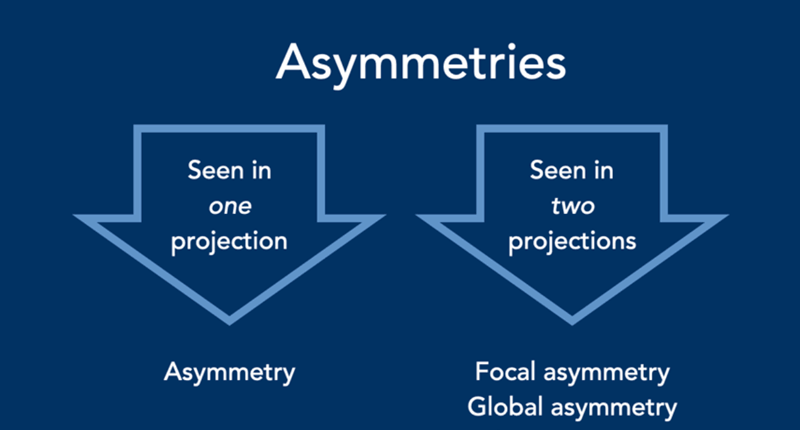
There are three types of asymmetries.
Asymmetry: visible on only one mammographic projection.
Focal asymmetry: seen in two projections, <1/4 of the breast.
Global asymmetry: seen in two projections, ⩾1/4 of the breast.
The term developing asymmetry descriptor has been removed.
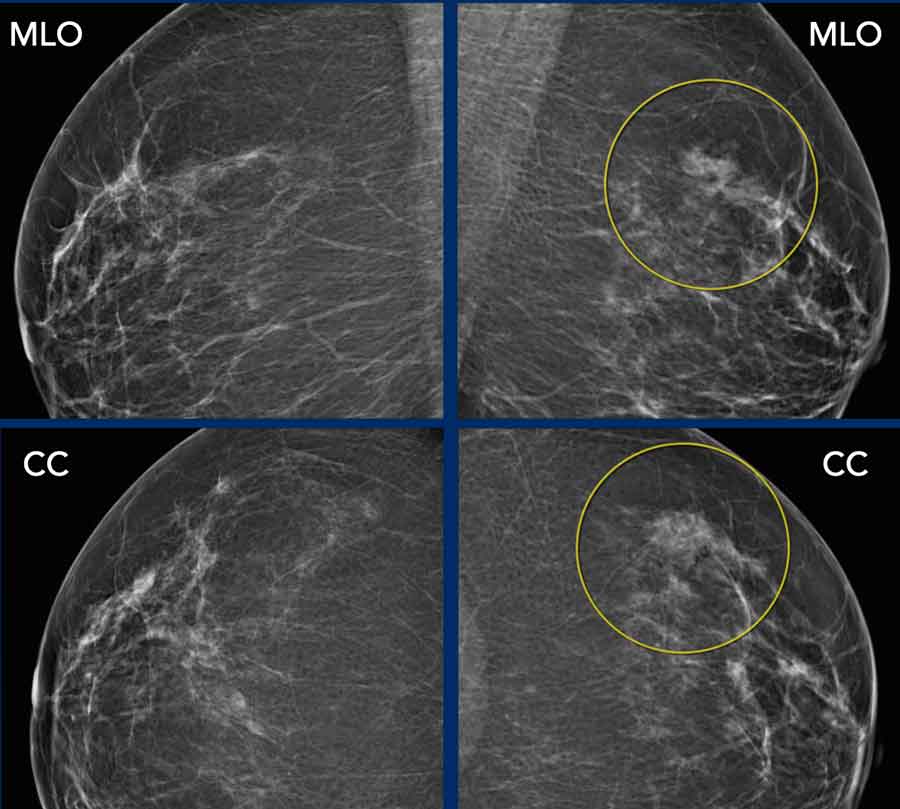
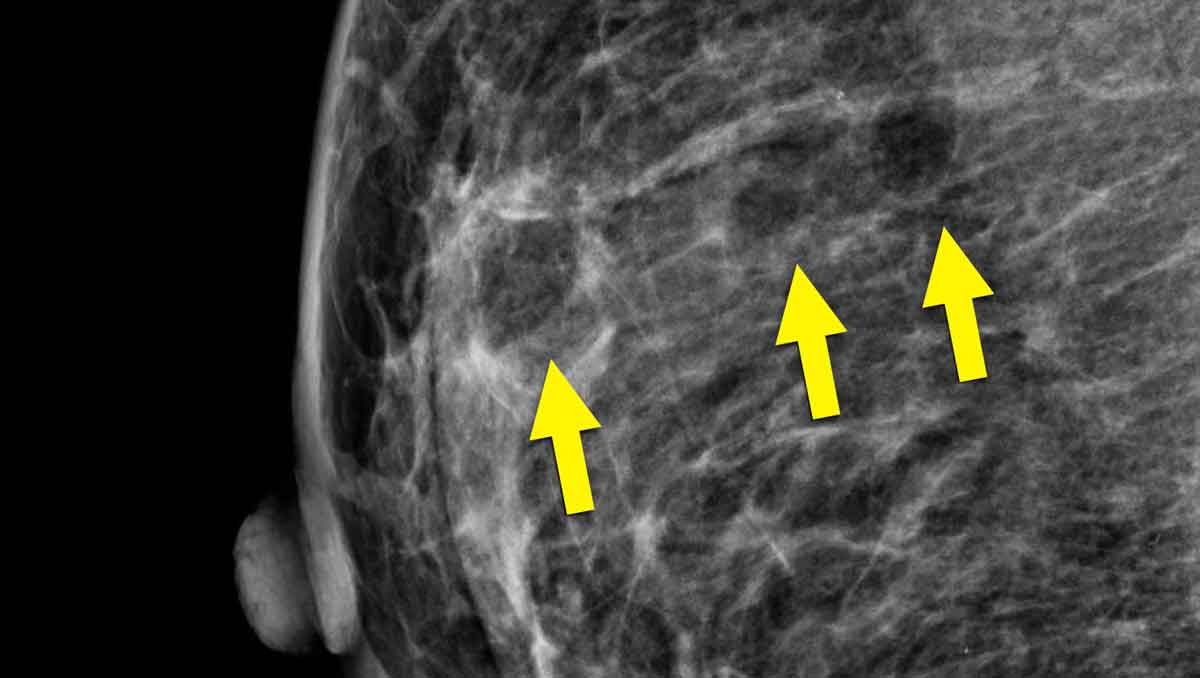
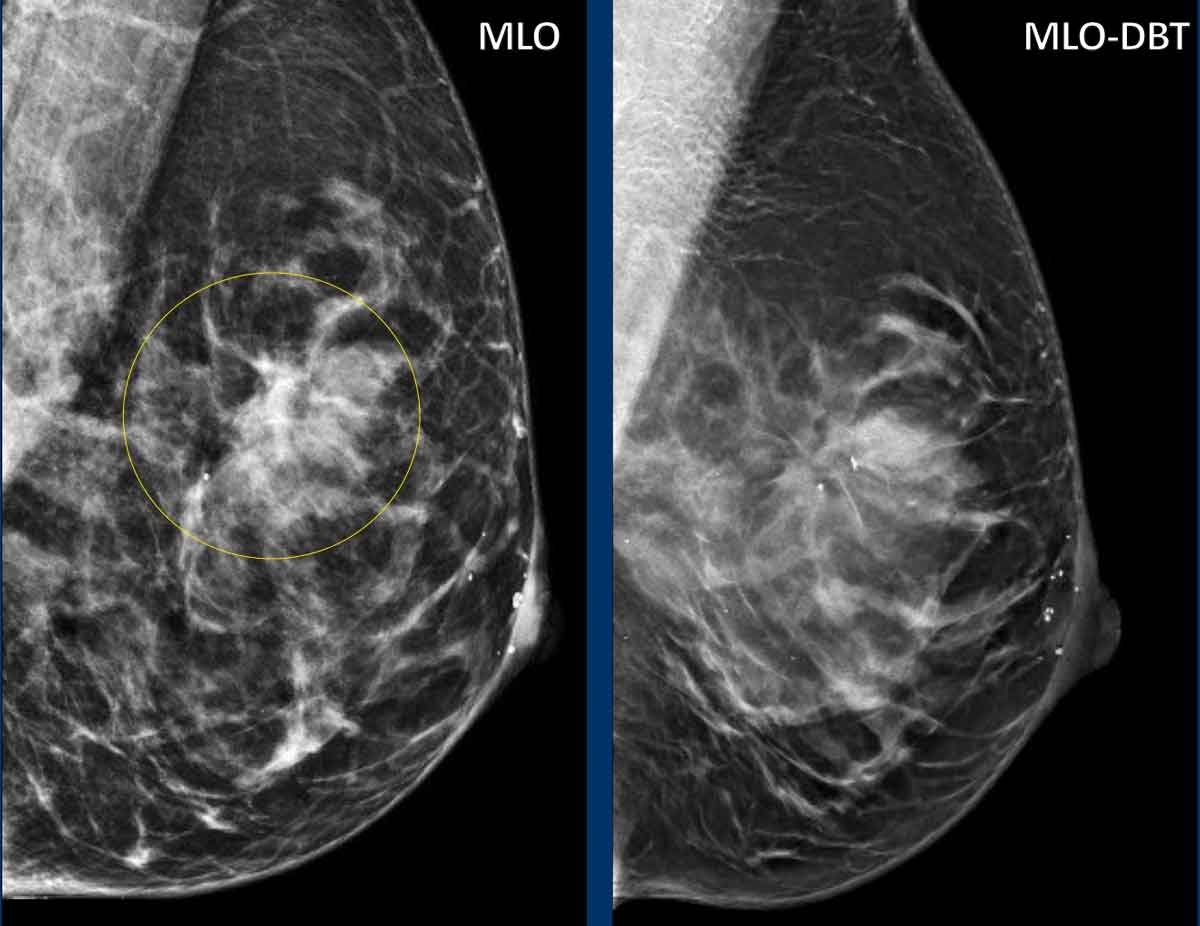
Focal asymmetry
A focal asymmetry is visible on both the MLO and CC)view.
Targeted compression views and breast ultrasound did not reveal a discrete mass.
The finding was interpreted as a focal accumulation of normal glandular tissue.
No change during follow up.
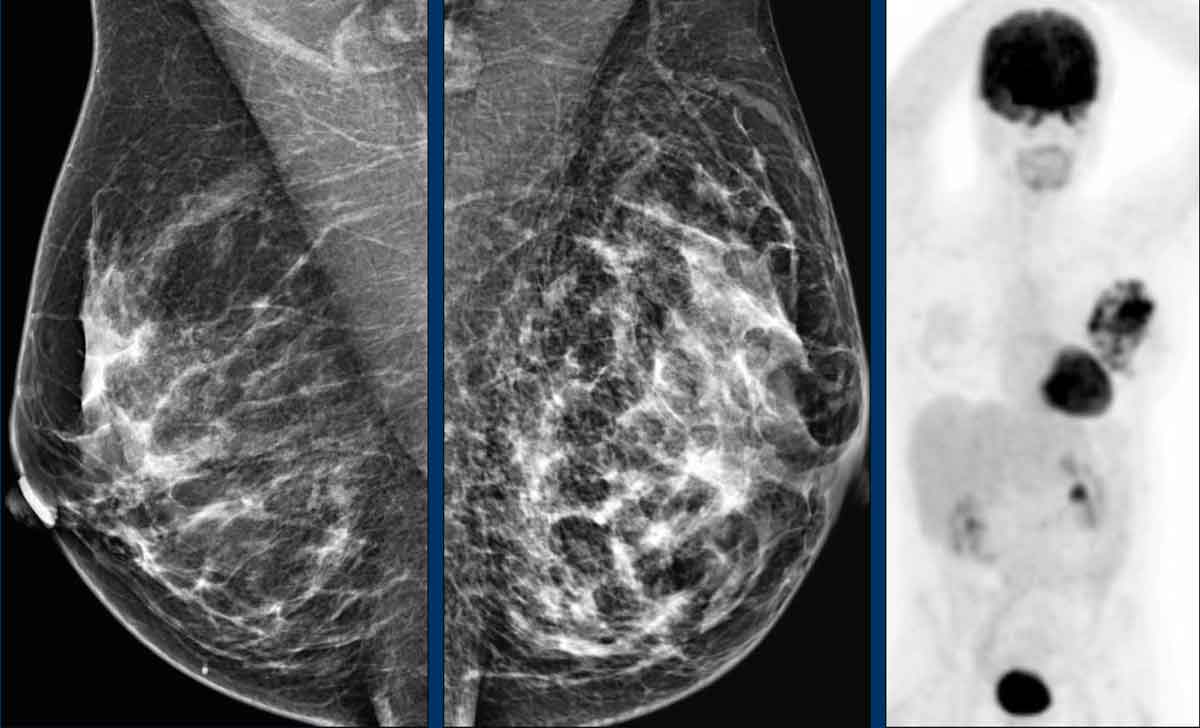
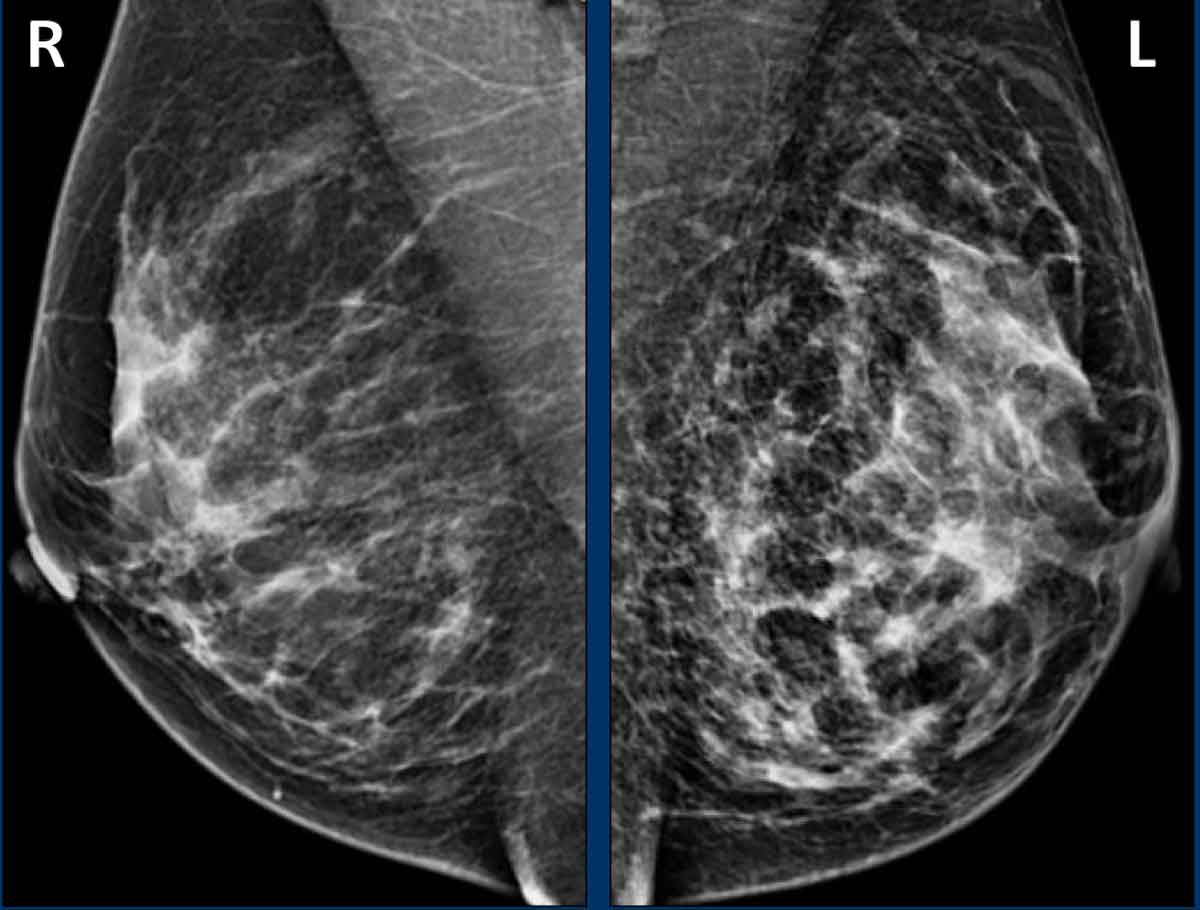
Global Asymmetry
This case demonstrates global asymmetry. In this patient, the asymmetry is not considered a normal variant, as it is associated with suspicious features suggestive of malignancy, including:
- Focal skin thickening
- Thickened trabecular septa
- Subtle nipple retraction
Imaging Findings
- Ultrasound (images not shown):
- Detected multiple small masses, subsequently histologically confirmed as adenocarcinoma.
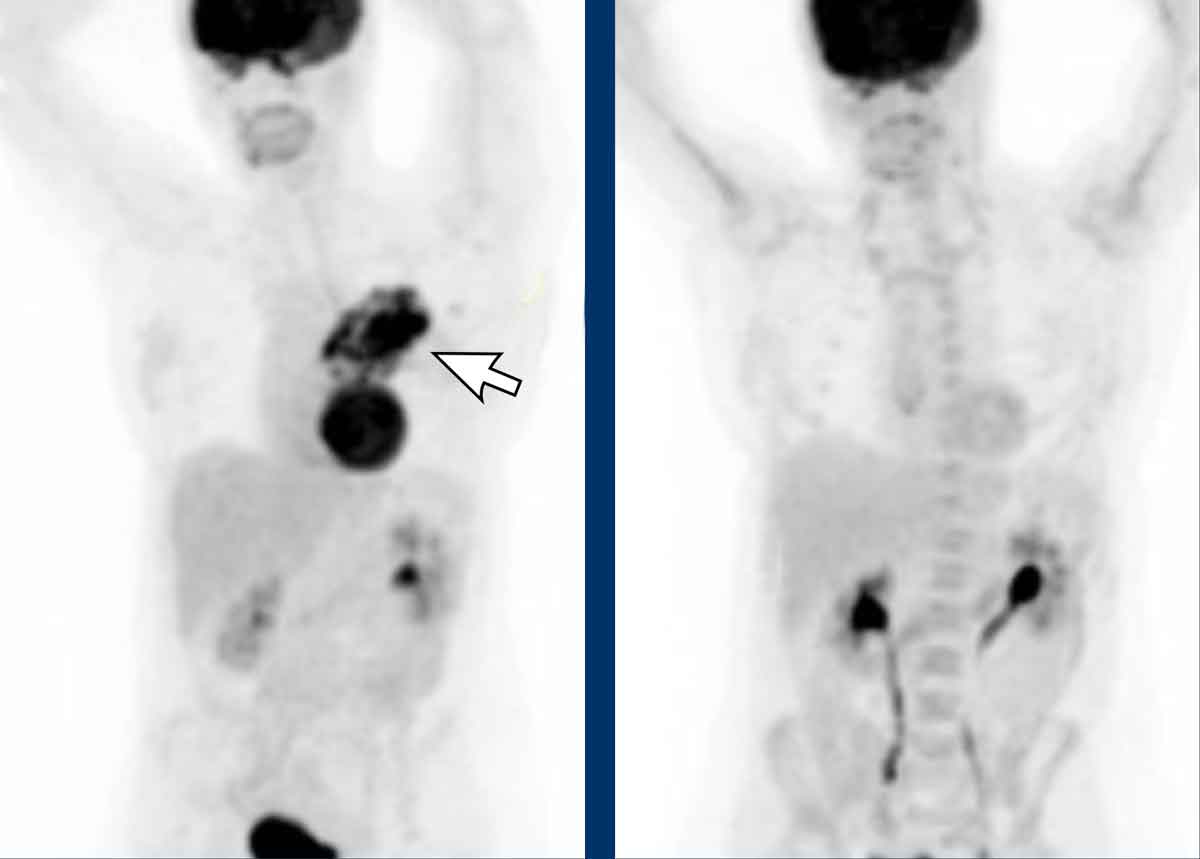
- PET-CT:
- Demonstrates diffuse infiltrating carcinoma.
Lymph nodes
Intramammary Lymph Nodes
Normal intramammary lymph nodes are most frequently located in the upper outer quadrant of the breast.
They typically exhibit a reniform (kidney-shaped) morphology and contain a fatty hilum, which is more clearly visualized on digital breast tomosynthesis (DBT) than on digital mammography (DM).
Abnormal intramammary lymph nodes may present with a rounded morphology and loss of the fatty hilum.
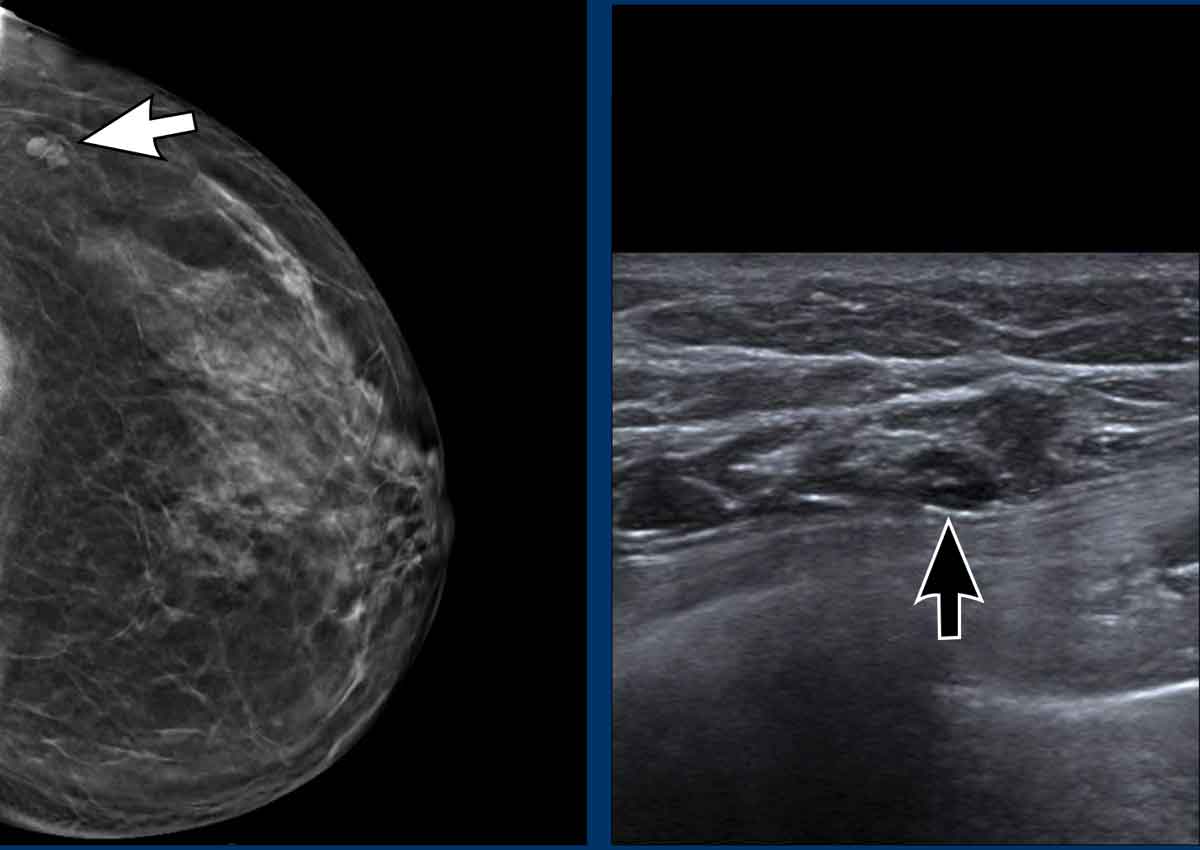
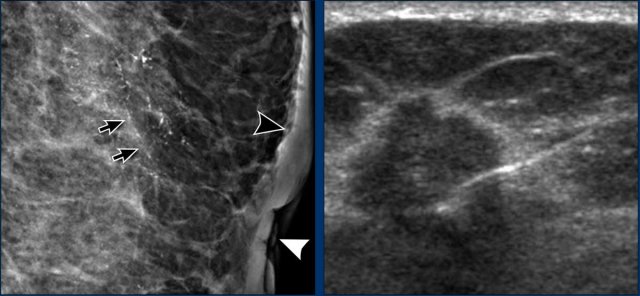
Example
Intramammary lymph node with kidney-shaped morphology (white arrow).
Notice the echogenic fatty hilum surrounded by the hypoechoic cortex on ultrasound (black arrow).
Axillary Lymph Nodes
Abnormal axillary lymph nodes may demonstrate the following features:
- Increased density
- Loss of the normal "fatty" or "reniform" appearance
- Irregular or indistinct margins
- Increased cortical thickness
- Presence of calcifications
- Enlargement compared to baseline
- Loss of the normal oval or bean shape
Bilateral adenopathy is more frequently associated with reactive or inflammatory etiologies than with malignant processes.
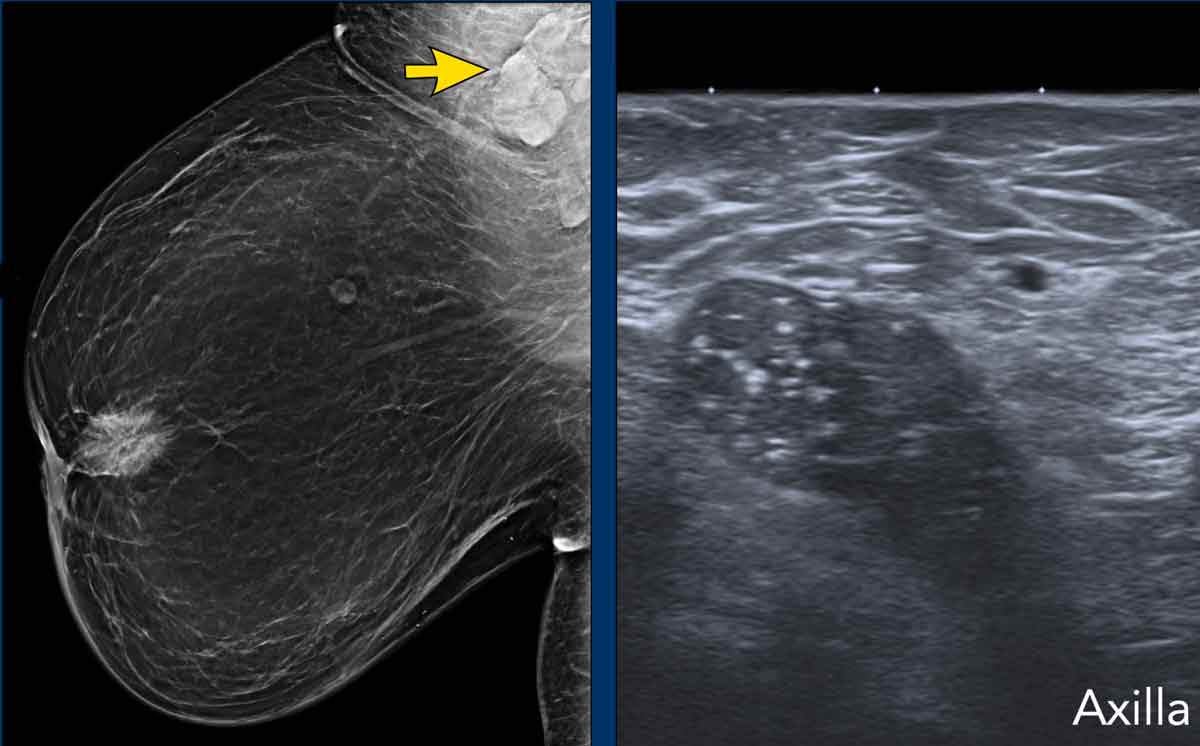
Example
The mammogram demonstrates a retroareolar mass accompanied by nipple retraction and cutaneous thickening.
Axillary lymphadenopathy is present, with barely visible calcifications (arrow).
Ultrasound evaluation reveals an enlarged lymph node exhibiting loss of the fatty hilum. The echogenic foci within the node represent small calcifications.
Example
Enlarges dense axillary lymph nodes in a patient with a large retromammillair cancer with nipple retraction.
Skin lesions
Skin lesions visible on mammography may include:
- Moles (nevi)
- Keloids
- Epidermal inclusion cysts
When identified on the skin surface, these lesions are often marked with a radiopaque skin marker for localization. They frequently exhibit a radiolucent halo, which is attributable to the presence of air surrounding the lesion’s base.
Skin lesions may be more readily characterized on DBT, particularly when located on the first or last tomosynthesis slices.
Dilated ducts
Multiple dilated ducts
Multiple dilated ducts are tubular structures, often greater than 5 mm in diameter, originating from the nipple that may be unilateral or bilateral. They are typically benign finding and are commonly seen in patients who are pregnant or lactating, When new, asymmetric or associated with clinical symptoms, or other mammographic abnormalities, further evaluation with diagnostic imaging may be warranted to exclude malignancy.
Solitary dilated duct
A solitary dilated duct is a unilateral single or branching tubular structure, often greater than 5 mm in diameter that is typically oriented towards the nipple. Solitary dilated ducts are a rare finding and may be the mammographic presentation for a patient with nipple discharge. While the fifth edition indicated that this finding should be considered a BI-RADS 4A finding, more recent publications, suggest that the malignancy rate is sufficiently low to consider it a benign assessment if there are no associated clinical or additional imaging findings or change over time.
Associated features
Associated features refer to secondary imaging findings described in conjunction with a primary breast abnormality.
These features may also serve as the initial presentation, prompting further diagnostic evaluation for an underlying primary lesion.
Associated features are:
- Skin retraction
- Nipple retraction
- Skin thickening
- Trabecular thickening
Skin Retraction
Focal or diffuse skin retraction may indicate underlying architectural distortion or malignancy.
Nipple Retraction
Nipple retraction raises suspicion for malignancy, particularly if:
- New in onset
- Unilateral
- Irreversible
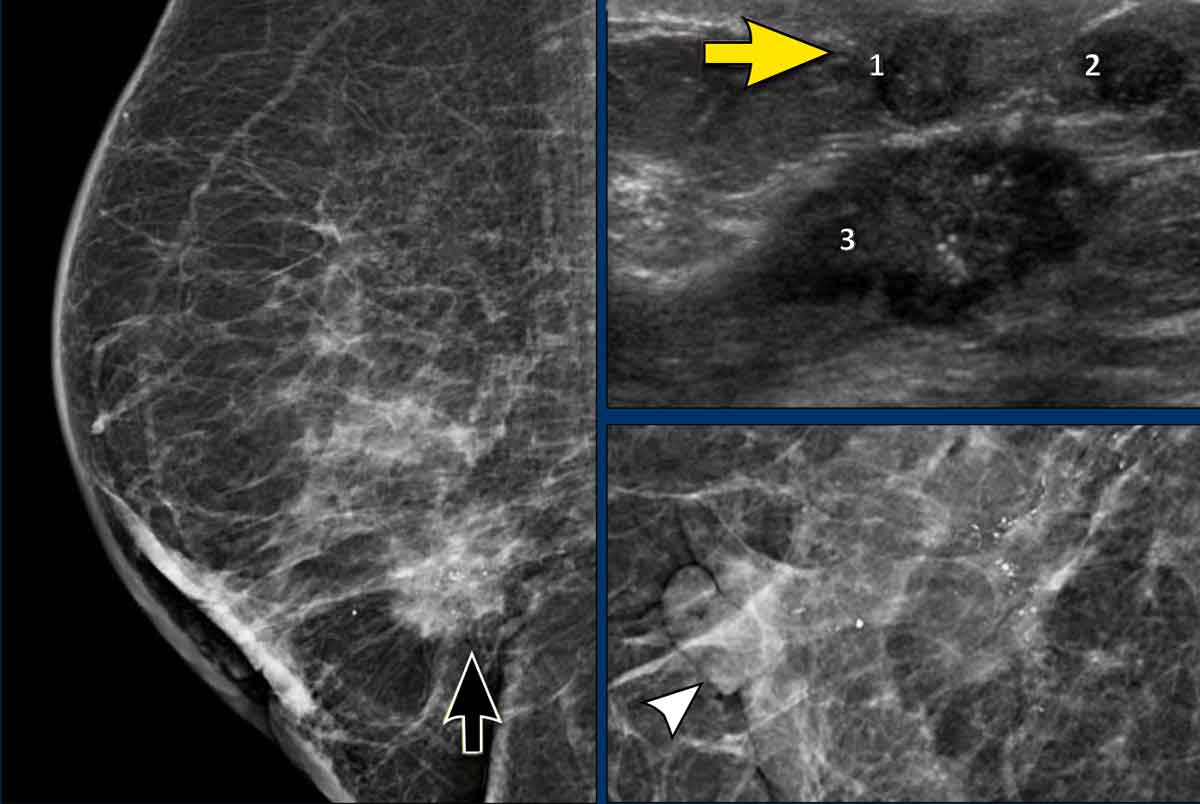
Example
Nipple retraction is observed, associated with an underlying high-density, irregular mass (black arrow).
On magnification view, the retracted nipple (white arrowhead) is seen and fine pleomorphic calcifications.
Ultrasound examination revealed three hypoechoic masses. Notably, calcifications are visualized as echogenic foci within mass nᵒ 3.
Pathology
Multifocal invasive ductal carcinoma.
Nipple inversion
Nipple inversion should be distinguished from nipple retraction, which is typically:
- Inconsistent or reversible
- Often bilateral
- Long-standing and stable
- Usually benign
Skin Thickening
- Skin thickening (>2 mm) may be focal or diffuse.
- Expected post-radiation therapy.
- Bilateral skin thickening is usually benign, often due to edema from systemic conditions (e.g., renal, hepatic, or cardiac failure).
- New, unilateral, or focal skin thickening is concerning for malignancy, unless attributable to a known infectious or benign inflammatory etiology.
Example
- Mammography: thickened skin (black arrowhead), nipple retraction (white arrowhead) and fine linear branching calcifications in a linear distribution (arrows)
- Ultrasound: irregular hypoechoic mass with an echogenic rim was detected deeper in the breast.
Notice the biopsy needle within the mass.
Pathology
Invasive ductal carcinoma.
Trabecular Thickening
Thickening of the fibrous (trabecular) septa within the breast may be observed in the following clinical contexts:
- Inflammatory breast carcinoma, resulting from tumoral infiltration and obstruction of lymphatic vessels
- Extensive axillary metastasis, due to lymphatic obstruction by tumor
- Systemic edema (e.g., secondary to congestive heart failure or renal disease)
- Lymphatic drainage impairment, such as following axillary lymph node dissection
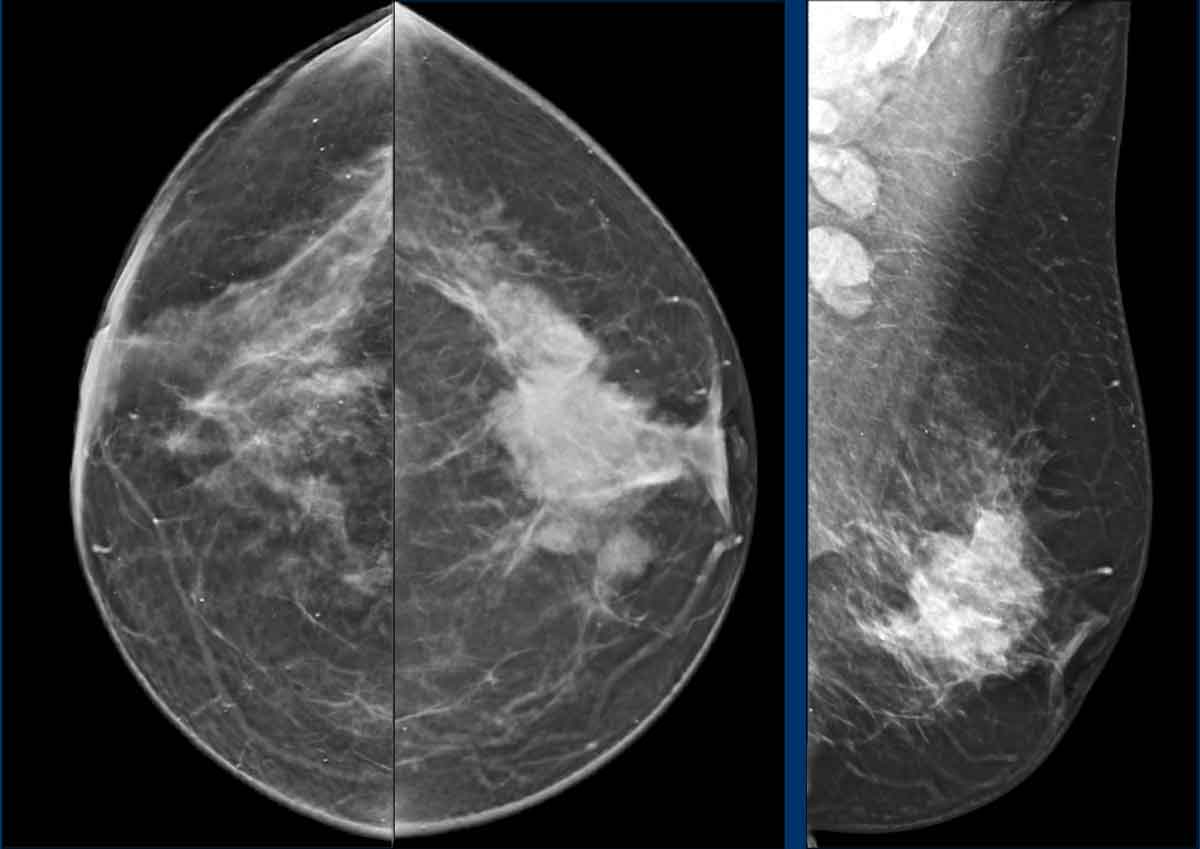
Example
Diffuse trabecular thickening in the left breast in a patient.
continue with PET-CT images...
PET-CT images pre- and post neoadjuvant chemotherapy.
Example
Trabecular thickening and skin thickening in a patient with mastitis carcinomatosa in the right breast.
Special cases
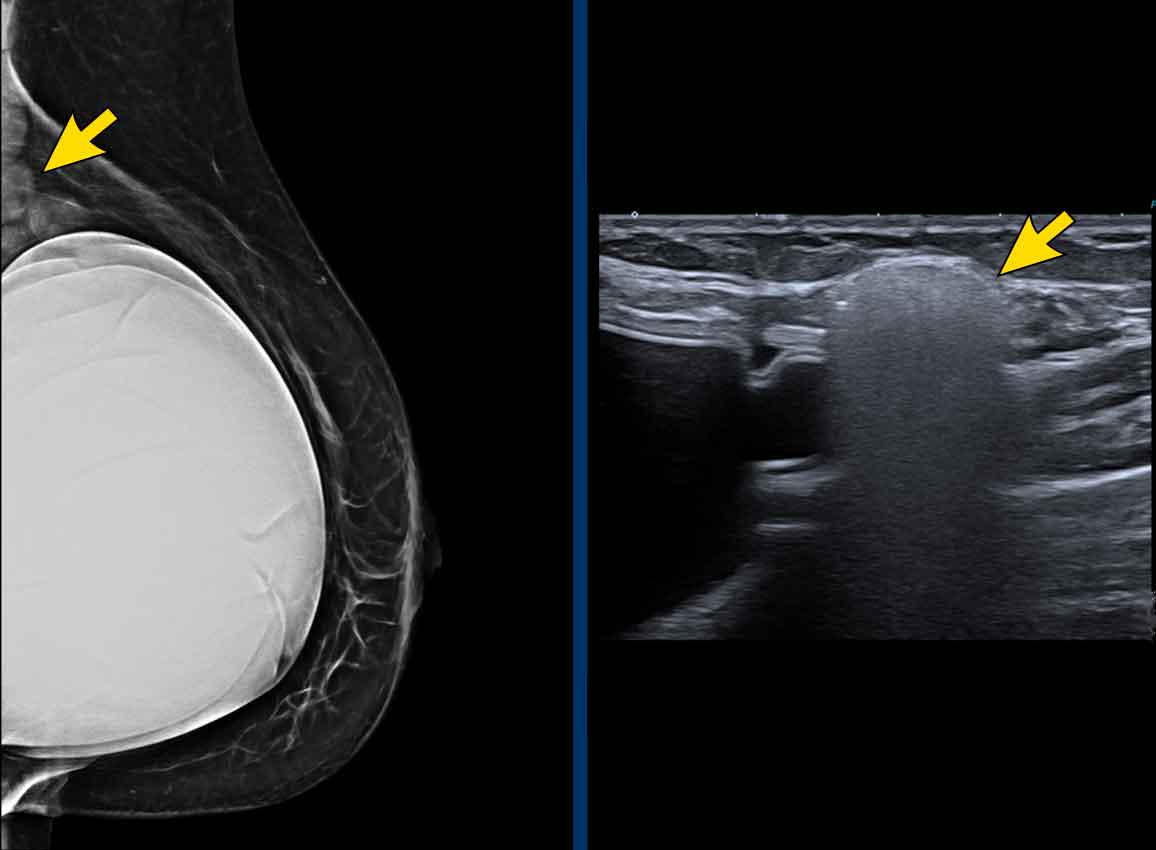
Gynecomastia
Gynecomastia refers to the benign proliferation of glandular breast tissue in male patients, which may be unilateral or bilateral.
On mammography, breast density in male patients should be documented using the same criteria as for female patients. Gynecomastia may present as:
- Nodular (focal)
- Diffuse (generalized)
Additional Findings: Any calcifications, masses, asymmetries, or architectural distortions should be carefully described, as these are not typical features of gynecomastia and warrant further diagnostic evaluation.
Images
This mammogram is of a male patient presenting with a palpable mass. Notably, the dense tissue is situated directly beneath the nipple (arrow), which is characteristic of gynecomastia.
On ultrasound, the typical appearance of nodular gynecomastia is a hypoechoic mass with lobulation or occasional spiculation. While such findings might be concerning in a female patient, in a male patient, this appearance is typical for gynecomastia, and the mammographic findings are reassuring.
Gynecomastia can result from diverse causes, including:
- Physiologic hormonal fluctuations (e.g., during adolescence or in older age)
- Medications: Antidepressants, Prostate cancer therapies, Anabolic steroids, Certain antibiotics, Chemotherapeutic agents
- Substance use: Marijuana, Methamphetamines, Alcohol, Heroin
- Systemic diseases: Liver failure, Chronic kidney disease, Lung cancer, Testicular cancer, Thyroid disorders
- Neoplasms: Adrenal tumors, Pituitary gland tumors
Breast Implants and Augmentation
Breast implants are frequently encountered during mammographic evaluation. The radiology report should include the following details:
- Type of implant:
- Saline
- Silicone
- Dual-lumen (combination of saline and silicone)
- Location of implant:
- Retropectoral (submuscular)
- Prepectoral (subglandular)
- Mammographic views obtained:
- Routine views or implant-displaced views
Direct Injection Augmentation
In some cases, materials such as free silicone, paraffin, or other substances may be directly injected into the breast tissue. These injections can produce characteristic mammographic findings, including:
- Fatty round deposits
- Dense deposits
- With or without rim calcifications
Mastectomy
While routine ipsilateral mammography after mastectomy is generally not indicated, imaging of the reconstructed breast or mastectomy site may be necessary to evaluate a clinical finding (e.g., a palpable lesion).
- Imaging post-mastectomy patients can be technically challenging due to the minimal residual breast tissue.
- As a result, only limited, targeted views of the area of concern may be feasible.
- These mammographic views are critical for accurate assessment, as fat necrosis—a common post-mastectomy finding—can mimic malignancy.
- On ultrasound, fat necrosis may present as an irregular, shadowing mass, potentially leading to unnecessary biopsy if correlative mammographic views are not obtained.
Location Descriptors for Breast Lesions
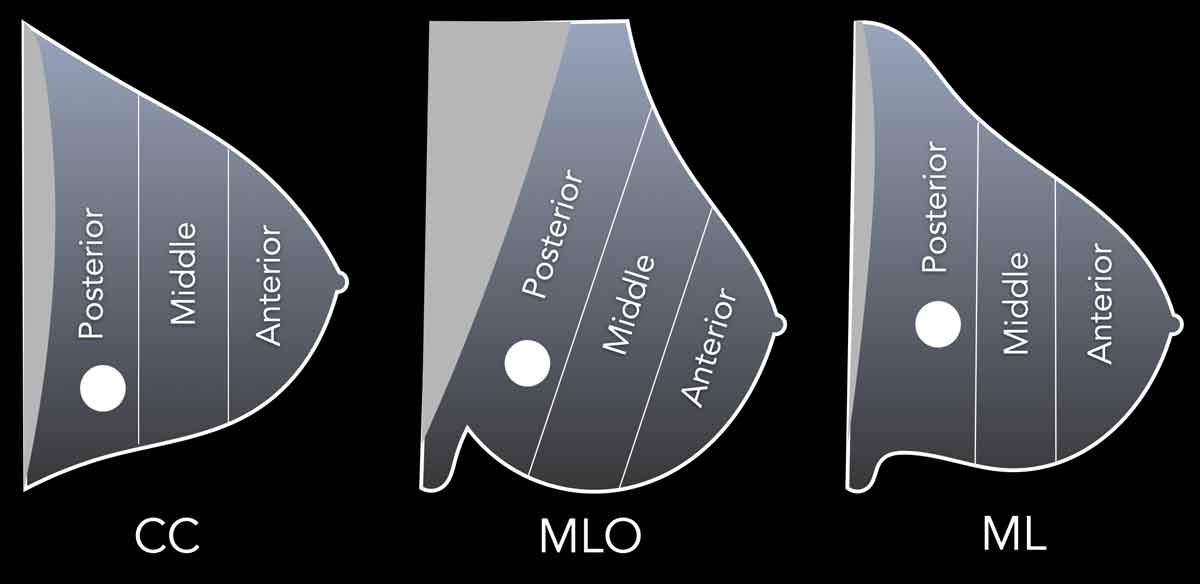
A complete set of lesion location descriptors should include the following:
- Designation of the breast: right or left.
- Anatomic location: quadrant and clock-face position (preferably both).
- Ultrasound documentation: the clock-face position and quadrant should be supplemented on the image with a body marker and indication of transducer orientation.
- Depth on MLO view is determined by using imaginary divisions that parallel the angle of the pectoralis major muscle. In this way findings that project over the axilla will always be considered at posterior depth.
- Distance from the nipple.
- For findings seen predominantly on DBT the slice number should be provided for all views to ensure that the findings can be accurately re-identified.
Lesion Correlation Across Imaging Modalities
When utilizing multiple imaging modalities, it is essential to confirm that the same lesion is being evaluated across all studies.
- A lesion identified on ultrasound (US) may not correspond to the mammographic or clinical (physical examination) finding.
- Repeated mammographic imaging with marker placement under ultrasound guidance can facilitate accurate correlation.
- Cysts may be aspirated or filled with air post-aspiration to confirm their mammographic appearance.
- For solid lesions, contrast injection or marker placement can be employed in diagnostically challenging cases.
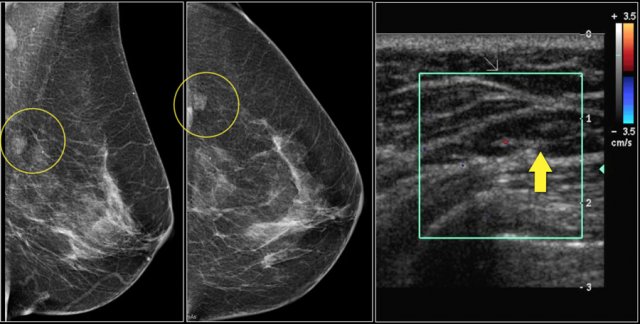
Case Presentation: New Lesion at Screening
The images provided are of a patient with a new lesion detected during screening.
- Ultrasound identified an intramammary lymph node, but correlation with the mammographic mass was uncertain.
- Contrast was injected into the node, and a repeat mammogram was performed.
Continue with the post-contrast images...
The mammographic mass contained contrast, confirming that the mass was due to the intramammary lymph node.
This patient presented with a tumor in the left breast.
In the right breast, a group of amorphous and fine pleomorphic calcifications was observed.
Continue with the ultrasound examination...
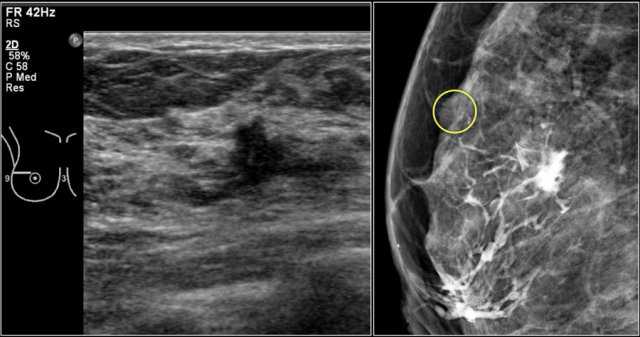
Ultrasound examination of the region demonstrated an irregular mass, which was confirmed as adenocarcinoma by fine needle aspiration (FNA).
- To determine if the mass was within the area of the calcifications, contrast was injected into the mass (nowadays we use markers).
- Result: The mass was located in a different region of the breast.
- Next Step: A vacuum-assisted biopsy of the calcifications is now indicated, as there may be ductal carcinoma in situ (DCIS) in one area and an invasive carcinoma in another.
Assessment Categories
Purpose of BI-RADS Assessment Categories:
- Standardized Reporting
- Provides a uniform language for radiologists to describe mammographic findings, reducing ambiguity and improving communication among healthcare providers.
- Risk Stratification
- Each category reflects the likelihood of malignancy, helping clinicians prioritize follow-up and management decisions.
- Clinical Decision-Making
- Guides next steps: routine screening, short-interval follow-up, additional imaging, or biopsy, based on the assigned category.
- Quality Assurance & Audit
- Enables tracking of outcomes and performance metrics, such as cancer detection rates and positive predictive values of biopsies.
- Patient Communication
- Facilitates clear, consistent explanations to patients about their results and recommended actions.
- Research & Data Collection
- Supports standardized data collection for research, clinical trials, and epidemiological studies.
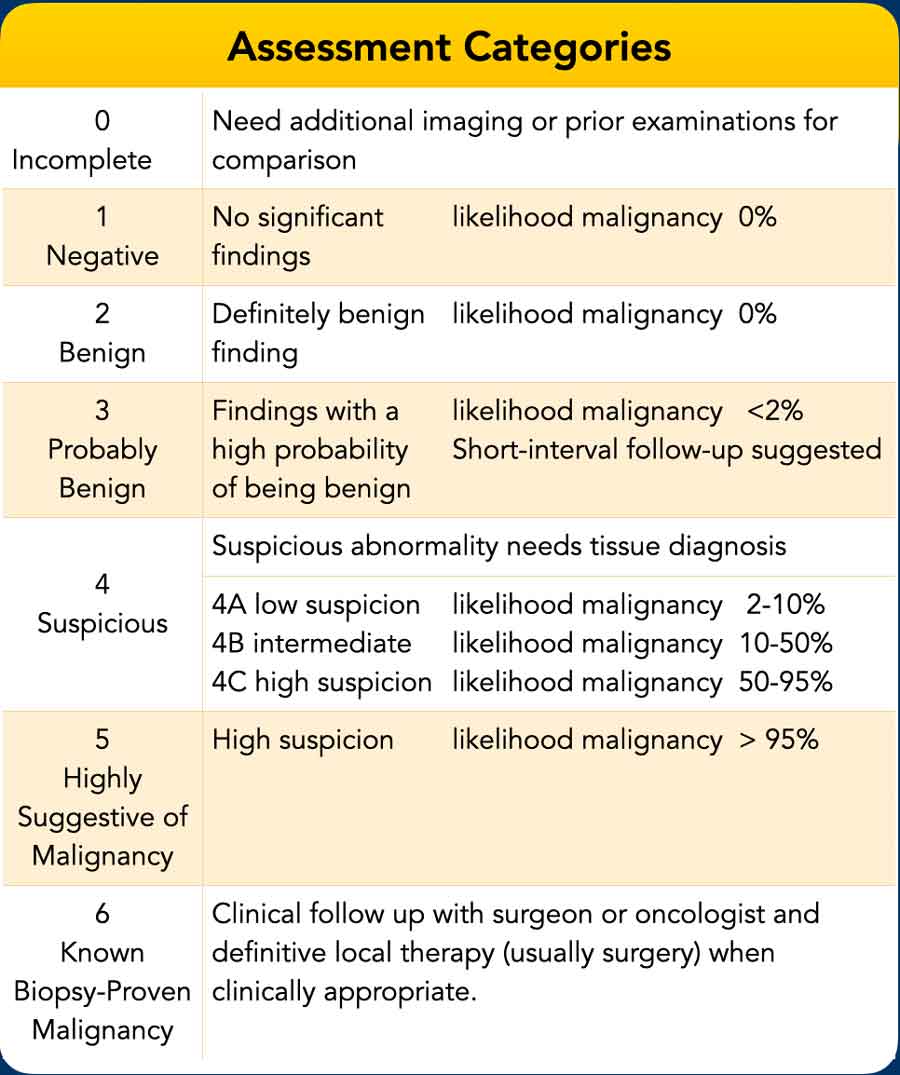
BI-RADS Category 0 – Incomplete
This category is assigned in a screening context to indicate that the examination is neither negative nor definitively benign, thus signifying the presence of an abnormality—even if suspicious—that requires a complete diagnostic workup.
BI-RADS Category 1 – Negative
No findings; normal examination.
BI-RADS Category 2 – Benign
Examples include calcified fibroadenoma, skin calcifications, surgical clips, and fat-containing masses.
BI-RADS Category 3 – Probably Benign
Assigned only after a complete diagnostic imaging evaluation.
Includes:
- A solitary, noncalcified, circumscribed solid mass
- Focal asymmetry without a corresponding ultrasound correlate
- A solitary group of round calcifications
Management: Short-interval follow-up imaging at 6, 12, and 24 months may be appropriate.
- If findings decrease in size or resolve during surveillance, the assessment may be downgraded to Category 2 or 1.
- If findings become more suspicious, the assessment should be upgraded, and biopsy is indicated.
- If the patient or referring clinician requests a biopsy, assign a Category 3 (probably benign) assessment with standard short-interval follow-up recommendations, but include a note stating that tissue diagnosis will proceed per patient/clinician preference.
BI-RADS Category 4 – Suspicious Abnormality
There is a suspicion for malignancy sufficient to warrant tissue diagnosis, but the findings are not pathognomonic for cancer.
BI-RADS Category 5 – Highly Suggestive of Malignancy
Examples include:
- Irregular, spiculated, high-density mass with associated microcalcifications
- New fine linear branching calcifications in a segmental distribution
Note: No single mammographic feature confers a >95% likelihood of malignancy; as with breast ultrasound and MRI, a combination of suspicious imaging features is required for a Category 5 assessment. A non-malignant percutaneous tissue diagnosis is typically considered discordant.
BI-RADS Category 6 – Known Biopsy-Proven Malignancy
Use Category 6 after tissue diagnosis of malignancy but prior to definitive therapy, when no additional mammographic abnormalities (beyond the known cancer) are present, or for second opinion review of previously biopsied malignant findings.
Additional indications:
- After attempted complete removal of the target lesion by percutaneous core biopsy, but before definitive local therapy or for monitoring response to neoadjuvant chemotherapy, even if all mammographic findings of cancer have resolved (since definitive local therapy has not yet been performed).
- After attempted complete surgical excision when pathology reports positive resection margins and mammography demonstrates at least one feature suggestive of residual tumor. The purpose of imaging is not to determine the need for re-excision, but to localize any suspicious area that should be included in the planned re-excision.

Charity
All the profits of the Radiology Assistant go to Medical Action Myanmar which is run by Dr. Nini Tun and Dr. Frank Smithuis sr, who is a professor at Oxford university and happens to be the brother of Robin Smithuis.
Click here to watch the video of Medical Action Myanmar and if you like the Radiology Assistant, please support Medical Action Myanmar with a gift.