Characterization of Adrenal lesions - Update
New threshold and no more Wash Out CT
Nanda Krak¹ and Robin Smithuis²
¹Radiology Department of Waikato Hospital, Hamilton, New Zealand and ²Alrijne Hospital in Leiden, the Netherlands
Publicationdate
Adrenal lesions are frequently encountered, being identified in approximately 5% of CT examinations [1].
These lesions are often detected during the evaluation of patients with known malignancy or endocrine disorders; however, the majority are discovered incidentally on imaging studies performed for unrelated indications—not as part of oncologic staging or due to suspected adrenal pathology.
Most such incidentalomas are benign, posing a clinical challenge to differentiate them from malignant masses without subjecting patients to unnecessary and burdensome further investigation.
This article will review specific adrenal tumors and discuss recommended updated guidelines for the management of incidentalomas.
With a strict definition of incidentaloma and endocrine evaluation for most adrenal lesions, the new proposed guidelines are:
- Discontinuation of adrenal washout CT in the assessment of adrenal incidentalomas.
- Elevation of the benignity threshold to ≤20 HU for lesions measuring <4 cm on noncontrast CT.
Adrenal Incidentaloma
 Courtesy of Seow et al. Washed up: the end of an era for adrenal incidentaloma CT
Courtesy of Seow et al. Washed up: the end of an era for adrenal incidentaloma CT
An adrenal incidentaloma (AI) is defined as a lesion of ≥ 1 cm that is detected on imaging not performed for suspected adrenal disease, and in a patient with no current or prior extra-adrenal malignancy [2,3].
Evidence shows that nearly all AIs are benign, with one of the largest
studies finding no malignancy in 1049 AIs, and the other finding a prevalence
of 0,1% in a cohort of 1506 AIs [1,4].
For a long time, adrenal incidentaloma (AI) assessment has relied on two key principles:
- a noncontrast CT (ncCT) attenuation threshold of ≤10 Hounsfield units (HU) to indicate benignity, and
- adrenal washout CT (AWCT) for lesions exceeding this cutoff.
However, recent evidence and a critical reappraisal of existing data suggest that neither approach remains valid in contemporary adrenal incidentaloma diagnostics as clearly demonstrated by Seow et al in their review article [2].
With a strict definition of incidentaloma and endocrine evaluation for most adrenal lesions, the new guidelines are:
- Discontinuing AWCT use in AI assessment, and
- Raising the benignity threshold to ≤20 HU for lesions <4 cm on ncCT.
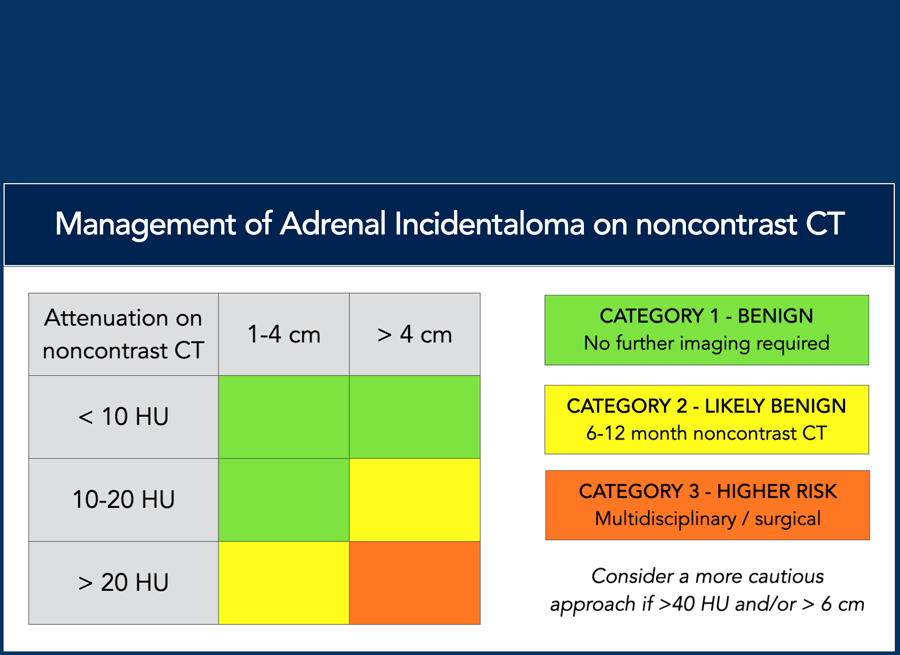
Seow et al. [2] have proposed recommendations as outlined in the table.
The figure in the next paragraph serves as an illustrative representation of these guidelines.
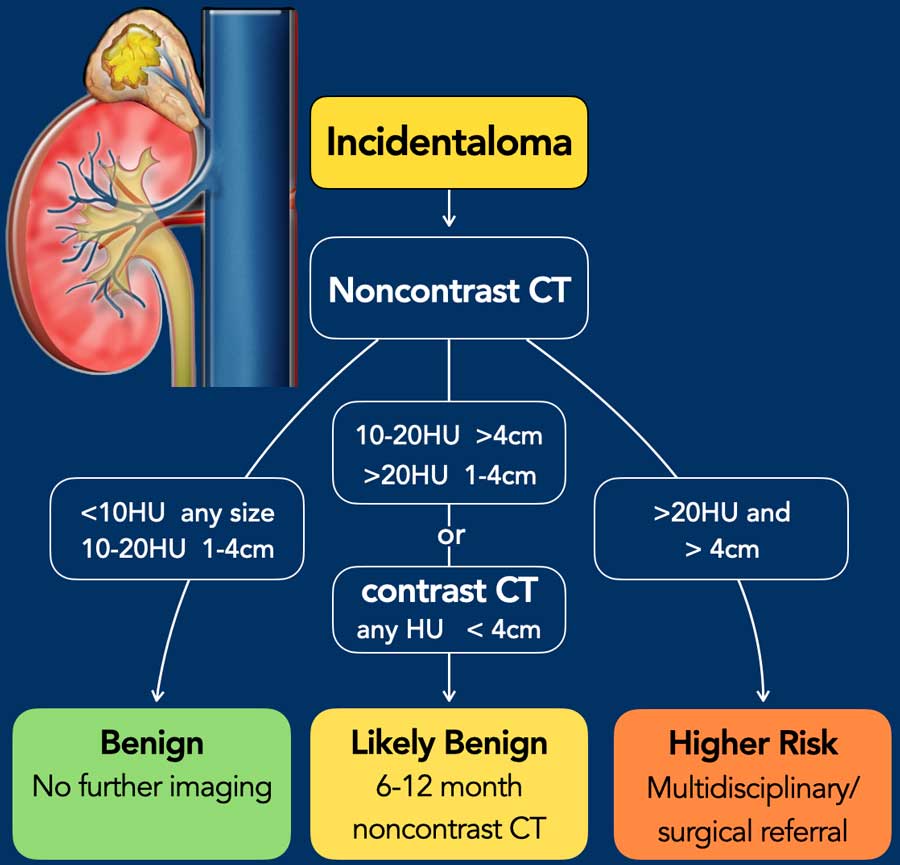 The figure is based on the guidelines given by Seow et al in the article entitled "Washed up: the end of an era for adrenal incidentaloma CT". We advise all to read this excellent article.
The figure is based on the guidelines given by Seow et al in the article entitled "Washed up: the end of an era for adrenal incidentaloma CT". We advise all to read this excellent article.
Systematic approach
Step 1 - Is it a true Adrenal Incidentaloma?
> 1cm, no endocrine/adrenal symptoms, no prior or current malignancy.
Step 2 - What is the density on a noncontrast CT and what is the size?
- Benign: < 10HU (any size) or 10-20HU (1-4 cm) and homogeneous.
No further imaging is needed. - Likely benign: 10-20HU (> 4cm) or > 20 HU (1-4 cm). Do a follow up scan at 6-12 months to look for growth. There is convincing evidence, that adrenal tumors under 4 cm with density 11-20 HU are virtually always benign [1] [2].
- Higher risk: > 20HU and > 4 cm. Heterogeneous. Discuss in multidisciplinary team/surgical referral.
Heterogeneity (due to necrosis/cystic change and/or haemorrhage), large size (in particular > 6 cm), significant growth and density > 40 HU are more consistent with a nonadenoma and/or with a nonbenign lesion [2, 5]. Significant growth is defined as size increase of > 20% of maximum diameter or ≥ 5 mm size increase over a period of 6-12 months [3].
Step 3 - Clinical and hormonal assessment is recommmended in all patients with an incidentaloma.
What if an adrenal lesion is not a true incidentaloma?
Adrenal tumours are frequently discovered on a cancer staging scan or in patients with a history of cancer. Primary cancers that most frequently metastasize to the adrenal glands are NSCLC, renal cell carcinoma, melanoma, breast and colon cancer.
Apply steps 2-3 in these patients: assess benign versus malignant imaging features and evaluate for hormonal activity. Because of the higher risk of malignancy an individualised approach is appropriate, including MDT discussion and likely FDG PET-CT [3].
Imaging techniques
 Lipid-rich adenoma
Lipid-rich adenoma
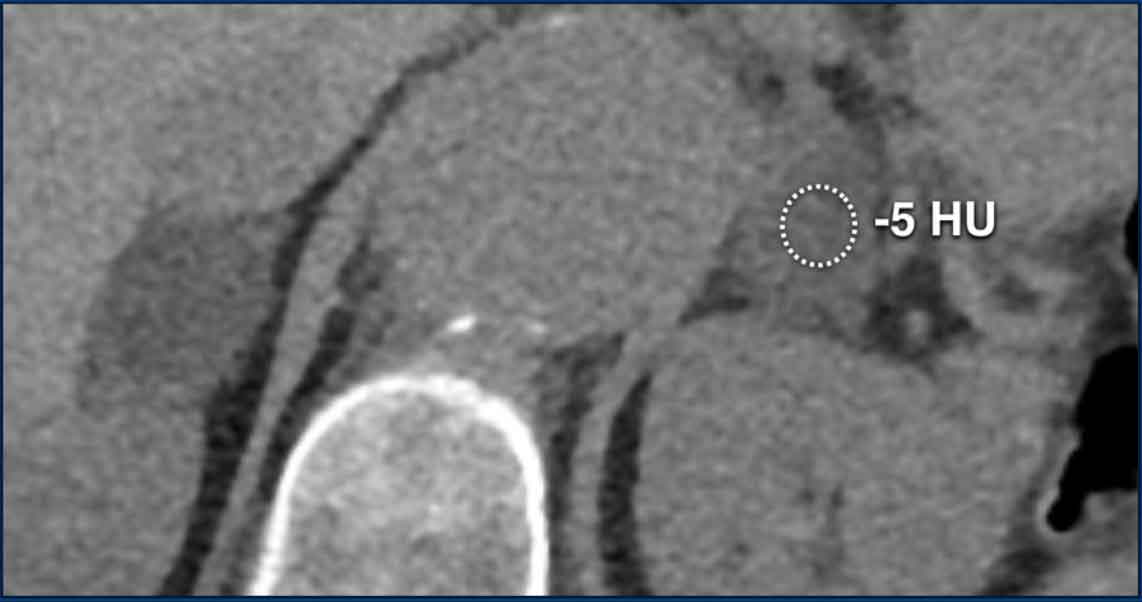
Unenhanced CT
The presence of microscopic fat strongly suggests a benign adrenal
lesion and helps distinguish adenomas from non-adenomas.
Approximately 70% of
adenomas are lipid-rich, due to high concentration of microscopic fat.
Unenhanced density of
10 HU or lower can
confidently diagnose such lesions as adenomas.
Note the following:
- an AI ≤ 4 cm with ncCT density 11-20 HU can be considered benign, and will usually be an adenoma (i.e. a lipid-poor adenoma).
- If ncCT density is 21- 30 HU chemical shift MRI is sometimes useful to help detect microscopic fat, see below.
- With unenhanced density above 30 HU other factors, like tumor size, heterogeneity, hormonal activity, clinical history and clinical context need to be taken into account to assess further steps [5].
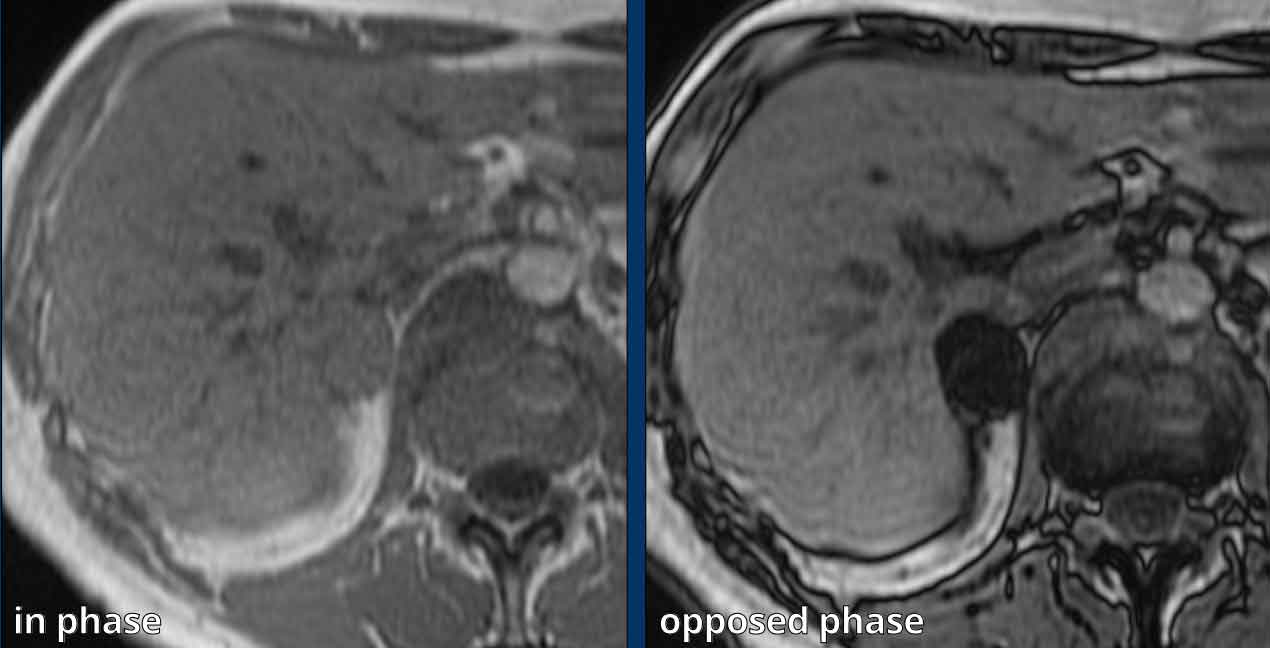
Chemical shift MRI
Chemical shift MRI can effectively demonstrate microscopic fat
within adrenal adenomas by showing diffuse or heterogeneous signal drop on
opposed-phase images relative to in-phase images.
This signal loss can be
calculated using the adrenal-to-spleen ratio or signal intensity index, but is
usually assessed visually.
An important known pitfall of Chemical shift MRI is that sensitivity to detect microscopic fat in lipid-poor adenomas declines with higher unenhanced CT density, in particular if higher than 30 HU [5].
Images
Well-defined, non-hormonally active indeterminate
2.9 cm right adrenal lesion initially found on a contrast-enhanced
staging CT for breast cancer.
Chemical shift MRI showed diffuse signal drop on
the opposed phase, in keeping with an adenoma.
Spectral CT
Dual-energy CT (DECT) and the newer photon-counting CT (PCCT) are distinct imaging techniques, but both can produce spectral images that enable the detection and quantification of lesion components such as fat, iodine, or calcium.
Numerous spectral parameters exist, with virtual non-contrast (VNC) imaging being the most widely recognized. While VNC density approximates true non-contrast CT (ncCT) density, it tends to consistently overestimate it. Published VNC density cut-offs for adenoma characterization range from ≤13 to 29 HU. In clinical practice, the diagnostic accuracy of spectral imaging improves when multiple spectral parameters are combined. Thresholds for PCCT are not yet well established.
The primary clinical advantage of DECT and PCCT is the potential to avoid additional unenhanced CT follow-up if an incidentaloma—initially detected on a post-contrast CT—can be characterized as an adenoma based on spectral parameters (see text and images below).
Images
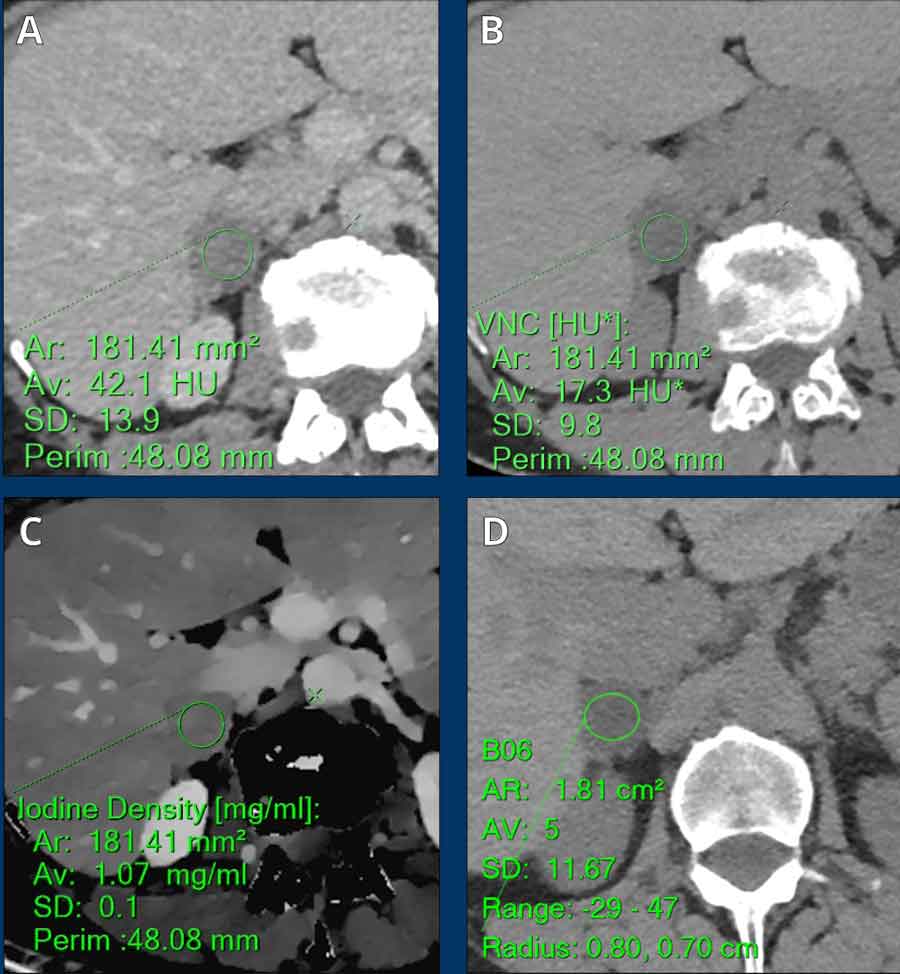
Incidentally found 3 cm lesion scanned on
a venous phase dual energy CT (A), not hormonally active.
Two spectral parameters are shown: VNC (B)
and iodine density (C), which can be combined into a ratio to increase accuracy.
VNC images (B) is 17 HU and the iodine density/VNC ratio is 6.2, both in keeping
with an adenoma.
A ncCT chest (D) performed 6 month later for unrelated reasons showed stable size of the lesion
and mean TNC density of 5 HU.
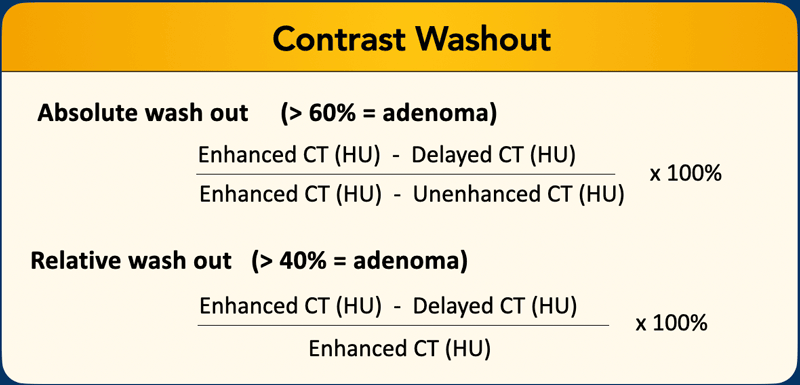 A region of interest (ROI) is placed encompassing at least 2/3 of the lesion (taking care to bypass areas with obvious haemorrhage, necrosis or calcifications). The density is measured during noncontrast, venous (60-90 sec) and delayed (15 min) phase, and washout calculated using the equation shown.
A region of interest (ROI) is placed encompassing at least 2/3 of the lesion (taking care to bypass areas with obvious haemorrhage, necrosis or calcifications). The density is measured during noncontrast, venous (60-90 sec) and delayed (15 min) phase, and washout calculated using the equation shown.
Washout CT - any remaining role in selected cases?
For decades, washout CT has been used to characterize indeterminate adrenal lesions, particularly to distinguish lipid-poor adenomas from non-adenomas. Adenomas typically demonstrate absolute washout ≥60% and relative washout ≥40%.
However, washout CT has limited sensitivity and specificity for differentiating lipid-poor adenomas from non-adenomas in a true incidentaloma population. Additionally, several tumors—such as pheochromocytomas, hypervascular metastases (e.g., from renal cell carcinoma or melanoma), and adrenocortical carcinoma—may exhibit similar washout percentages to adenomas.
Conclusion
Washout CT has no role in the workup of adrenal incidentalomas.
Limited Role of Washout CT
Washout CT may still have a limited role in the evaluation of non-incidentalomas, but only after hormonal assessment.
For example in cases of a hormonally inactive indeterminate adrenal lesion discovered during the workup of a hypovascular primary cancer, where MRI or FDG-PET are unavailable.
Specific Adrenal tumors
 Atypical lesions that prooved to be adenomas
Atypical lesions that prooved to be adenomas
Atypical adenomas
These lesions are typically not prospectively diagnosable as adenomas.
A hormonal workup is required, and multidisciplinary meeting discussion is often warranted.
While some lesions may be followed up, many are resected due to the inability to definitively exclude malignancy.
Atypical features are:
- Calcifications
- Heterogeneity (due to haemorrhage or cystic change)
- Large size > 4 cm
- Macroscopic fat
- Significant growth (≥ 5 mm/year) [5].
Images
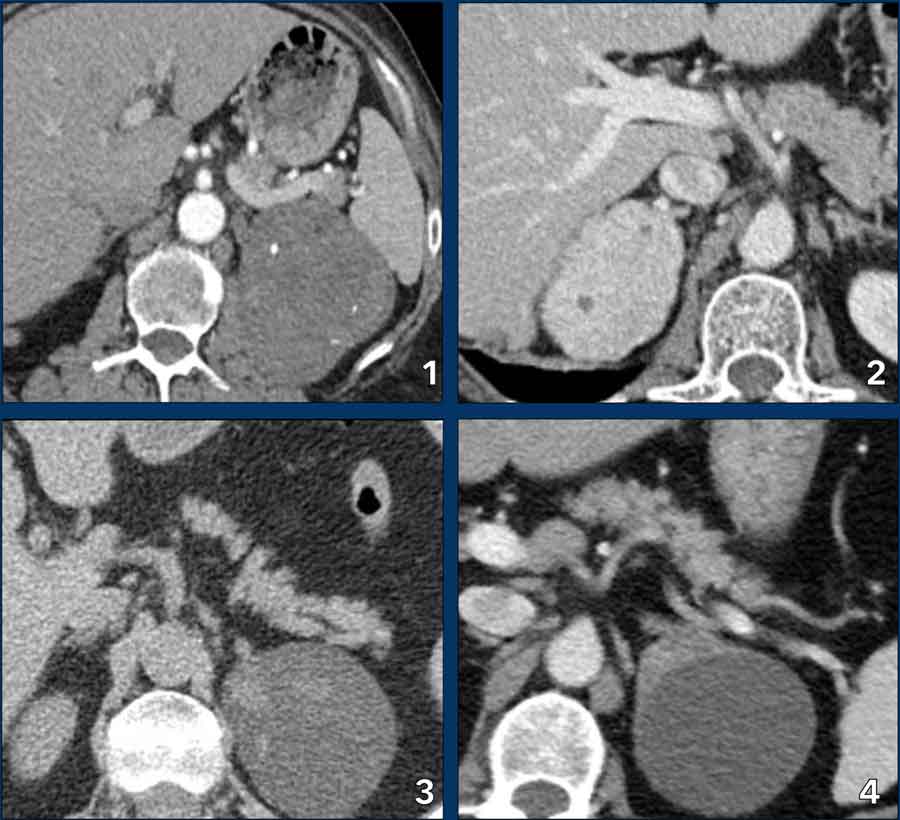
All of these lesions were resected due to large size, indeterminate radiological features, or interval growth. The histological diagnosis of adenoma was only confirmed post-resection.
- Large hyperenhancing lesion with small calcifications and cystic spots.
- Large hyperenhancing lesion with small cystic spots.
- Lesion with hyperdense strands as a result of internal bleeding.
- Left adrenal adenoma with an encapsulated post-haemorrhagic pseudocyst.
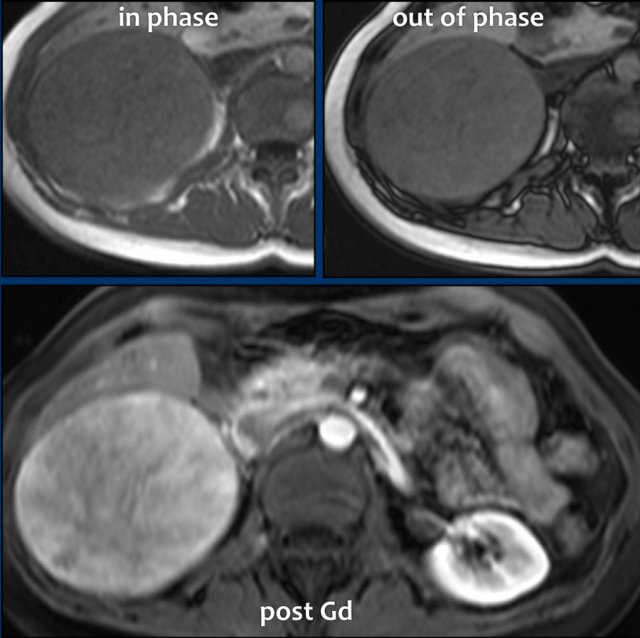
Atypical adenoma
The large adrenal lesion demonstrated no signal drop on the opposed-phase image and exhibited heterogeneous hyperenhancement post-contrast administration.
Following resection, the lesion was histologically confirmed as an adenoma.

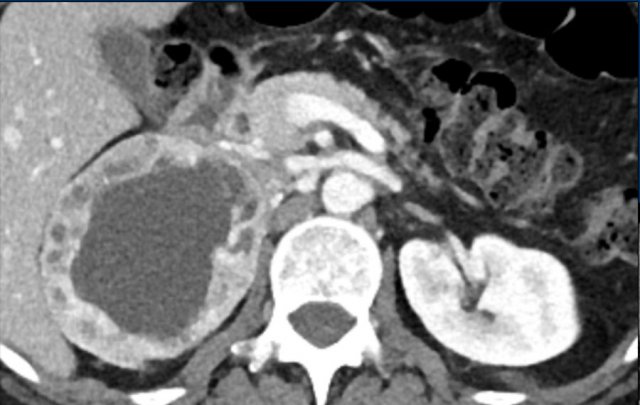
Cysts
Cysts are thin-walled, homogeneous, of water density and do not show any enhancement after contrast.
Images
Unenhanced and contrast-enhanced CT of a cyst.
Note that on unenhanced CT, an adrenal cyst may be indistinguishable from adenoma.
Calcifications
Most adrenal calcifications are asymptomatic and found
incidentally on imaging.
If bilateral and extensive, calcifications may indicate
chronic adrenal destruction (e.g., from TB or autoimmune disease), potentially leading to primary adrenal
insufficiency.
While rare, calcifications in the context of a mass may
prompt further evaluation.
Image
Coarse diffuse unilateral adrenal calcification with
no underlying tumor.
No cause was identified.
Image
Multiple coarse
punctate bilateral adrenal calcifications without an underlying tumor.
This patient had a history of granulomatous disease (TB).
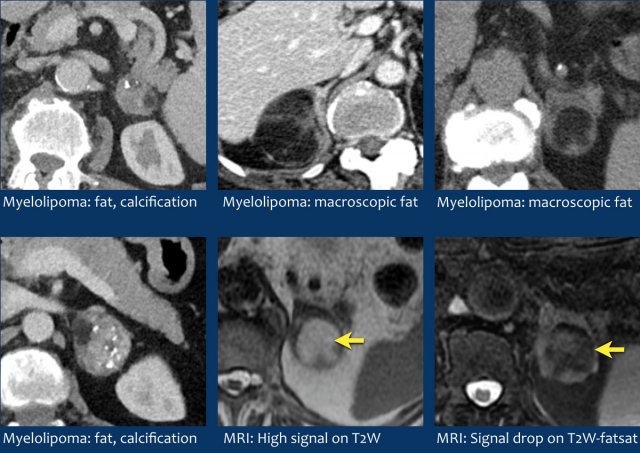
Myelolipomas
Adrenal myelolipomas are benign, uncommon adrenal tumors composed of variable proportions of hematopoietic bone marrow elements and mature adipose tissue.
These lesions are typically asymptomatic, though large myelolipomas may cause symptoms due to mass effect or spontaneous hemorrhage. The presence of macroscopic fat allows for straightforward identification on CT or MRI.
On non-contrast CT, attenuation values are characteristically <0 HU. Calcifications are observed in ~20% of cases.
On MRI, fatty components appear hyperintense on non–fat-saturated T1-weighted images and demonstrate signal dropout on fat-saturated T1- or T2-weighted sequences.
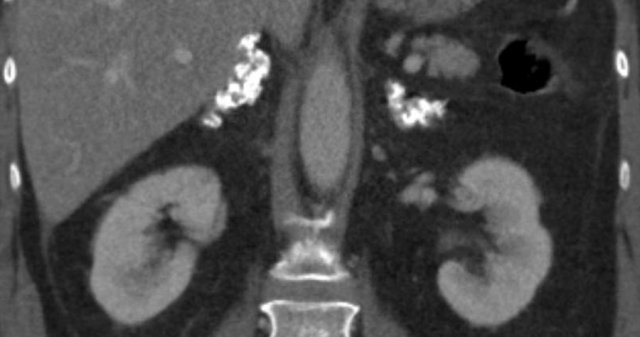
Myelolipoma
Bilateral adrenal myelolipomas with a
combination of macroscopic fat and soft tissue; on the right also containing
multiple coarse calcifications.
These were incidentally detected in an elderly
patient with macroscopic haematuria.

Myelolipoma
Unenhanced CT
image shows a large myelolipoma with bleeding and resorption of the hemorrhage
on the follow-up scan.
Pitfall fatty lesions
A diagnosis of adrenal myelolipoma can be confidently established if the macroscopic fat content is 50% or higher.
However, small amounts of macroscopic fat (usually < 5%) due to lipomatous and myelolipomatous change has rarely been described in adrenal adenomas, teratomas, metastatic clear cell renal cell carcinoma (RCC), pheochromocytomas, and adrenocortical carcinomas.
Conversely, metastases from fat-containing primary cancers, e.g. RCC or hepatocellular carcinoma may sometimes contain microscopic fat [5].
Images
Two large, fat-containing adrenal lesions
in 2 different patients.
Both lesions are well-demarcated and exhibit mixed
soft tissue, fatty components, and focal calcifications.
Due to their substantial size (32 cm and
13 cm, respectively) and indeterminate origin, surgical excision was performed.
Pathology
- Liposarcoma with osteosarcomatous differentiation
- Oncocytoma with fatty and myeloid metaplasia
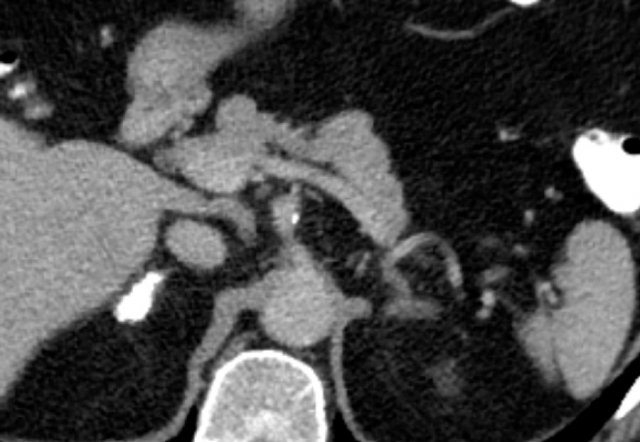
 Pheochromocytomas. All show strong enhancement, even in the smaller tumors. These cases were diagnosed by biochemical testing.
Pheochromocytomas. All show strong enhancement, even in the smaller tumors. These cases were diagnosed by biochemical testing.
Pheochromocytomas
Pheochromocytomas are rare catecholamine-secreting neuroendocrine tumors. Imaging cannot reliably distinguish benign from malignant pheochromocytomas unless there is local invasion or metastatic disease.
Clinical Presentation. Catecholamine excess typically causes sustained or paroxysmal hypertension, headache, profuse sweating and palpitations. However, 10–58% of pheochromocytomas are incidentally discovered in asymptomatic patients, with radiologists often being the first to suggest the diagnosis.
Diagnosis is usually made by biochemical testing (plasma free or urinary fractionated metanephrines) reliably confirms the diagnosis in ~100% of cases.
CT Characteristics
- Heterogeneous appearance due to necrosis, cystic change, or hemorrhage.
- Marked hypervascularity:
- Peak portal venous phase enhancement typically >85 HU
- Venous phase enhancement ≥130 HU (highly specific; but differential of hypervascular metastases, e.g. from HCC or RCC).
- Washout CT is unreliable: 30–50% may mimic adenoma washout patterns.
- Unenhanced CT density: Usually >10 HU (microscopic fat or lipomatous degeneration is extremely rare).
MRI Characteristics
- "Light bulb sign": High signal intensity on T2-weighted images (due to cystic change or necrosis) in ~65% of cases.
- T2 adrenal-to-muscle signal ratio ≥3.95 (1.5T) and ≥3.33 (3T) supports the diagnosis of pheochromocytoma.
- T1 signal: Variable; may be high in cases of necrosis or hemorrhage.
- DWI/ADC: Useful for detecting nodal or liver metastases in malignant cases.
Large pheochromocytomas are prone to hemorrhage and necrosis mimicking malignancy.
Image
Large pheochromocytoma with central necrosis.
Pheochromocytomas are associated with familial syndromes like multiple endocrine neoplasia (MEN), von Hippel-Lindau, neurofibromatosis type I, familial paraganglioma syndromes caused by SDH-gene mutations, Sturge-Weber syndrome and Carney triad.
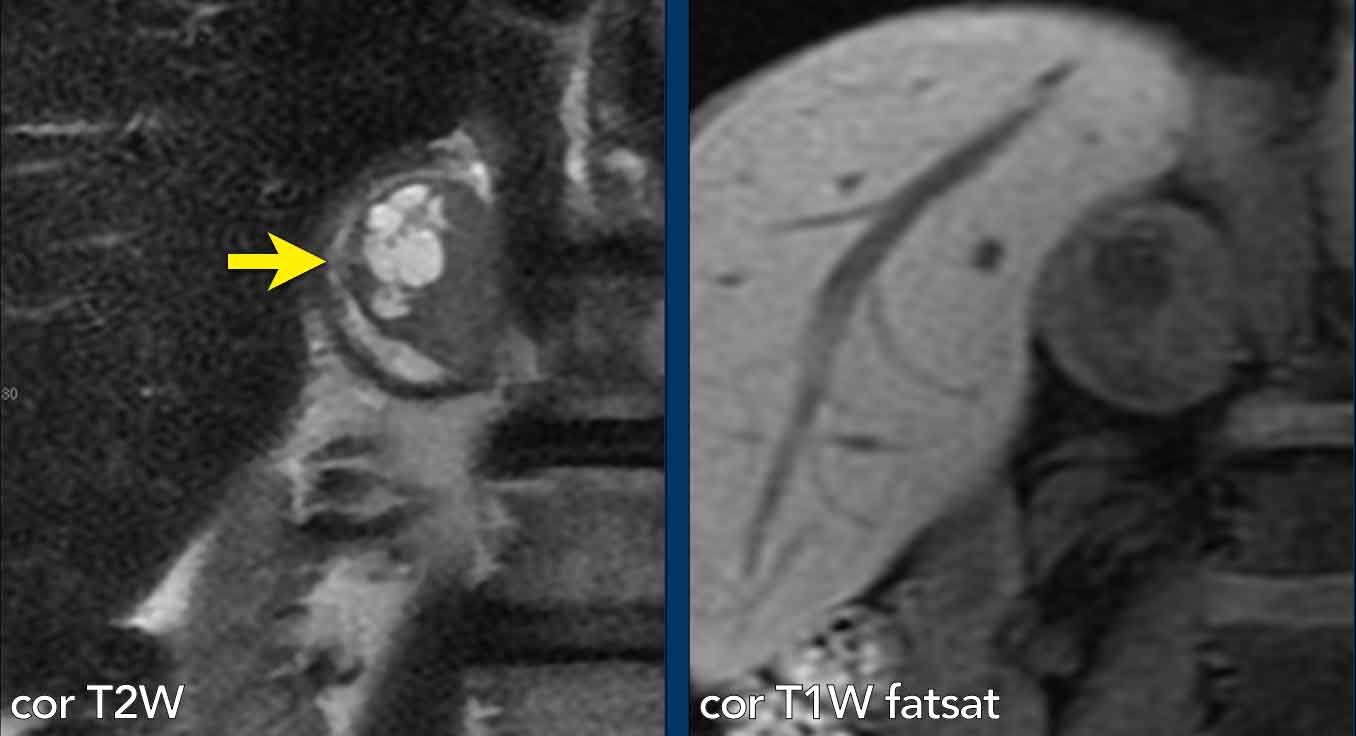
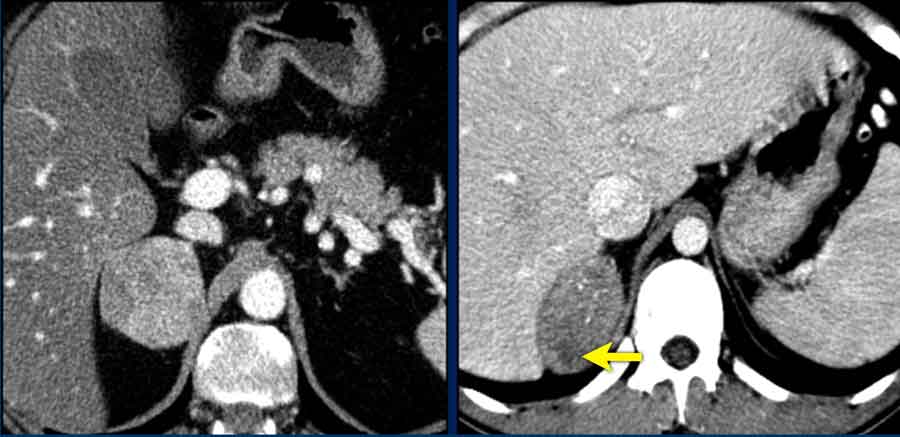
Case Presentation Pheochromocytoma
A 62-year-old male presented acutely with myocardial infarction and severe hypertension.
Imaging
MRI revealed an adrenal lesion with cystic portions (arrow).
Pheochromocytoma was diagnosed with biochemical testing.
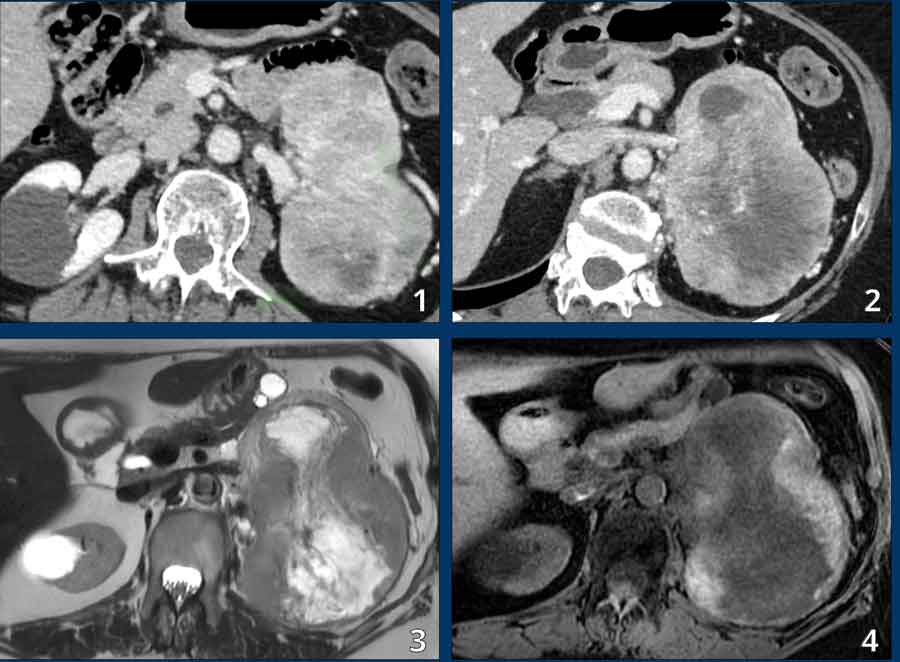
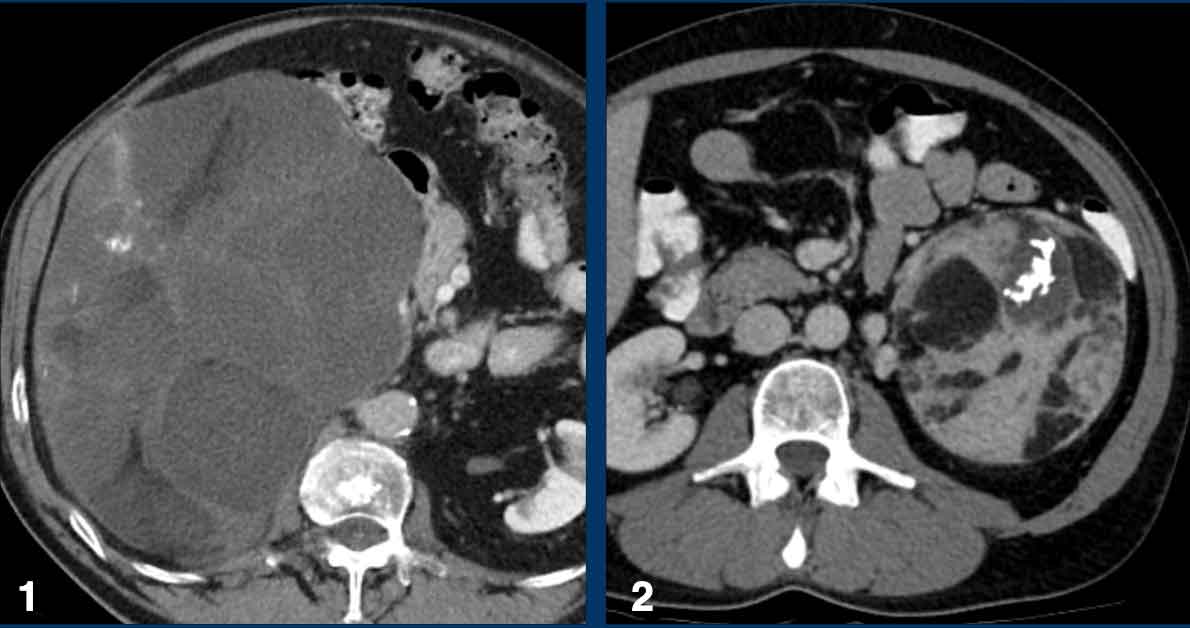
Case Presentation Pheochromocytoma
A 60-year-old woman presented with weight loss, left abdominal pain, and new-onset renal impairment.
CT scan:
- A very large (12 cm) left adrenal mass
- Heterogeneously hyperenhancing (density >130 HU)
- Large area of central necrosis
MRI:
- Heterogeneous tumor with:
- Peripheral hemorrhage
- Central necrosis
- "Light bulb bright" cystic components (image 3)
- No microscopic or macroscopic fat
Differential diagnosis
Included adrenocortical carcinoma vs. pheochromocytoma.
Final diagnosis
Biochemical analysis and pathology (post-adrenalectomy) confirmed pheochromocytoma.
Adrenocortical carcinoma
Adrenocortical carcinomas (ACCs) are rare, aggressive tumors with a variable clinical presentation:
- Functioning ACCs (~50–60% at diagnosis) may present with:
- Cushing’s syndrome
- Virilization
- Combined hormonal syndromes
- Non-functioning ACCs typically present with abdominal symptoms (e.g., nausea, vomiting, or abdominal fullness) due to large tumor size.
Imaging plays a critical role in staging, assessing resectability, and treatment planning:
- Localized disease (confined to the adrenal gland) has a 5-year survival rate of 58–68%.
- Stage III (locoregional node involvement, adjacent organ/fat invasion, or renal vein/IVC extension) has a 5-year survival of 40–55%.
- Stage IV (distant metastases) has a 5-year survival of 10–20%. Metastatic sites most commonly include the lung, liver, and bone.
Typical Imaging Features
- Unenhanced CT density: >30 HU
- Size: Usually >6 cm, with lobulated or round shape
- Internal characteristics:
- Stellate or irregular central necrosis
- Hemorrhage
- Calcifications
- Enhancement: Heterogeneous, with rim enhancement in ~2/3 of cases
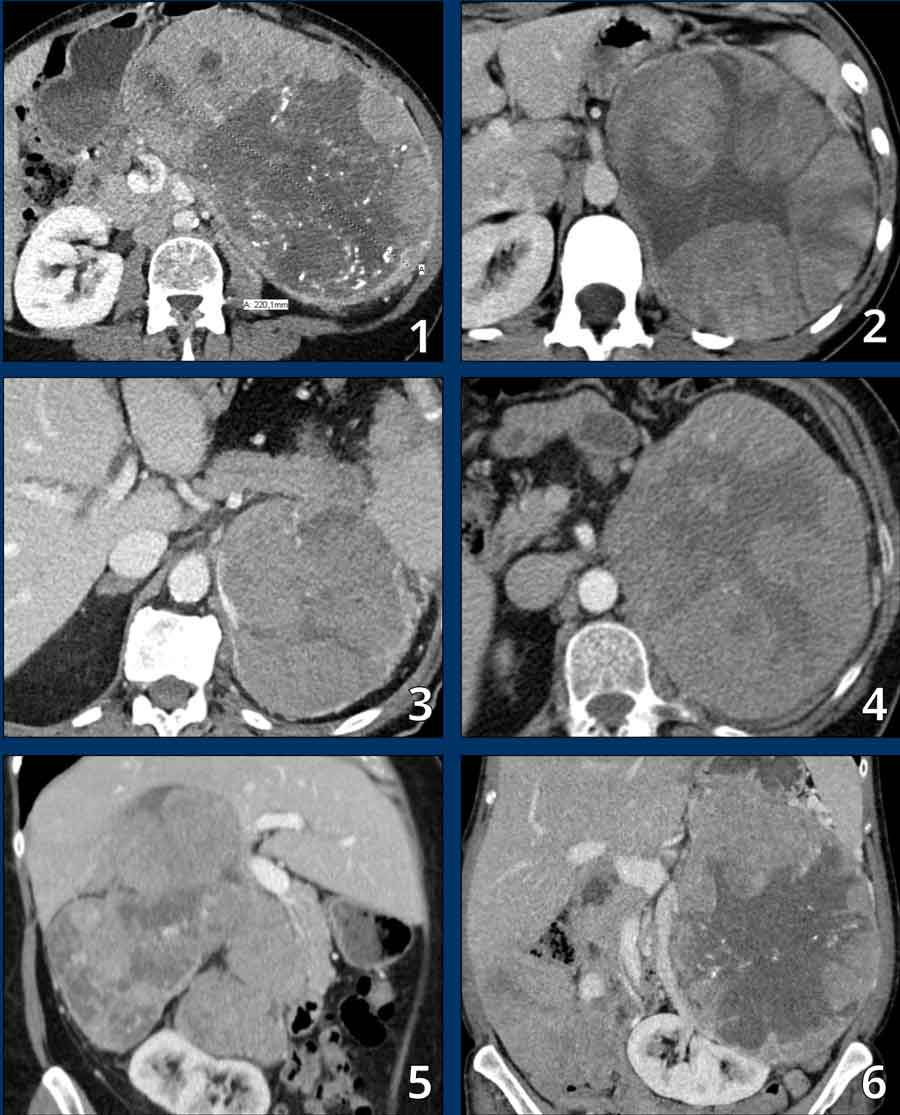
Images
These are typical examples of
adrenocortical carcinoma in 6 different patients.
The tumors are bulky, larger than 10 cm, displacing nearby organs,
and show heterogeneous enhancement.
Note the stellate central scar like hypodensities due to necrosis and cystic
changes.
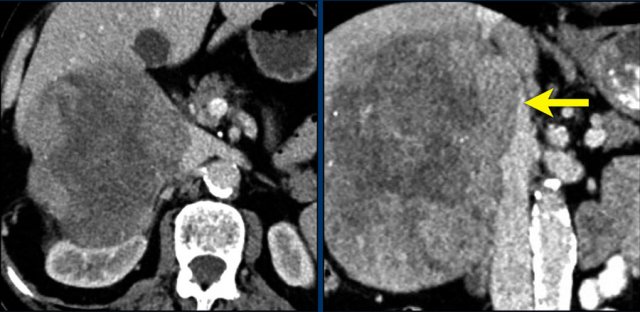
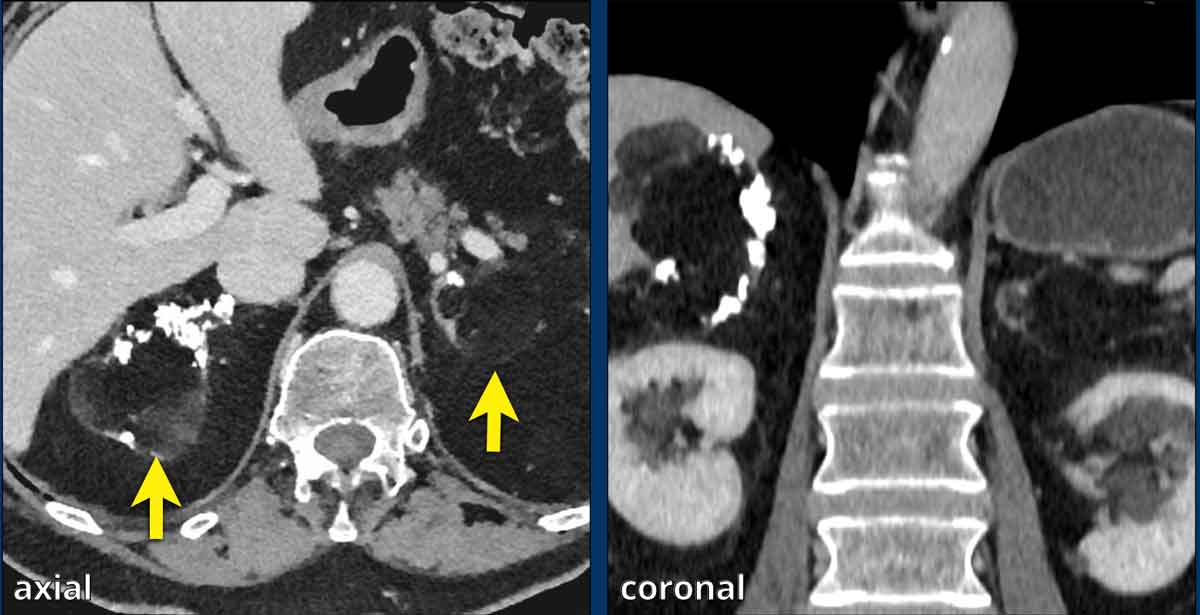
AAC Images
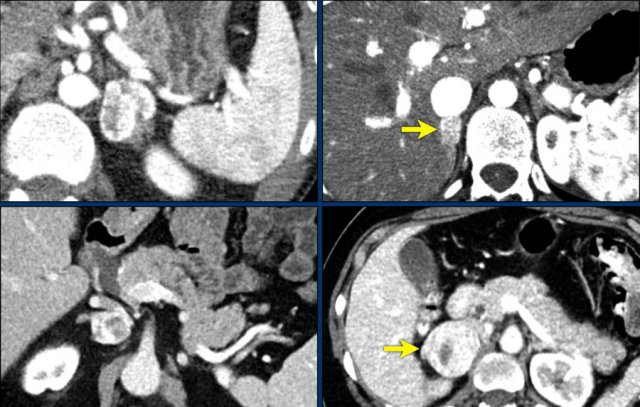
Axial and coronal CT images of a patient with an adrenal carcinoma with extensive IVC invasion (yellow arrow).
IVC and renal vein tumor invasion are seen in up to 20% of cases.
At diagnosis, over 50% of patients with adrenocortical carcinoma (ACC) present with stage III or IV disease, contributing to the poor prognosis associated with this malignancy.
Staging Evaluation
A comprehensive staging workup must include assessment for:
- Adjacent organ invasion
- Regional lymphadenopathy
- Distant metastases, most commonly involving the lungs, liver, and bones
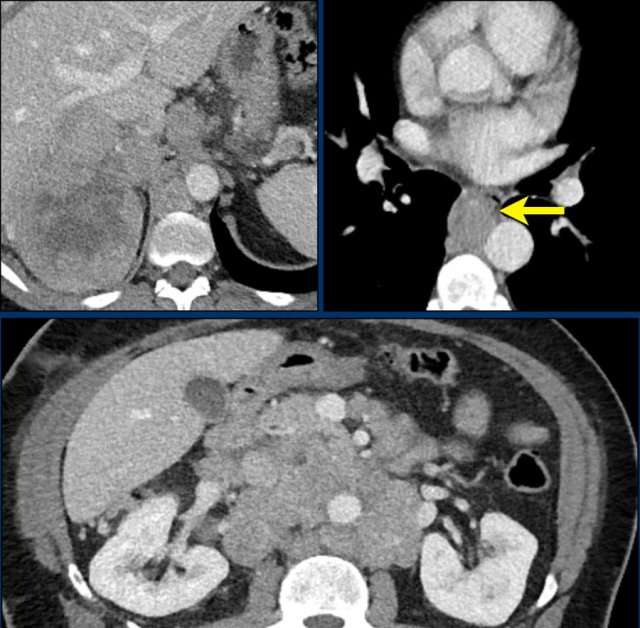
Imaging Example
Large right adrenal carcinoma with extensive abdominal and mediastinal para-aortic lymph node metastases (arrow).
Imaging Pitfall: Small Adrenocortical Carcinomas
Small adrenocortical carcinomas may exhibit less typical imaging features but still demonstrate heterogeneous enhancement.
Additional Findings are frequently dystrophic calcifications and areas of necrosis, despite the small size (arrow)
The tumors were resected following multidisciplinary meeting (MDM) discussion.
Bilateral Adrenal lesions
Causes of Bilateral Adrenal Lesions:
- Neoplastic:
Adenomas (most common); metastases (e.g., from lung, breast, melanoma, or renal cell carcinoma); lymphoma; bilateral pheochromocytomas. - Diffuse Enlargement:
Primary macronodular adrenocortical disease or secondary to ACTH- or CRH-dependent adrenocortical hyperplasia. - Infectious:
Tuberculosis, fungal infections, HIV-related infections. - Addison’s Disease:
Initial bilateral adrenal enlargement, followed by atrophy due to autoimmune destruction. - Bilateral Adrenal Hemorrhage:
Associated with sepsis, anticoagulation therapy, or trauma.
Suggested Approach:
Each lesion should be assessed individually, as with unilateral lesions, to classify as benign, likely benign, or higher risk. Clinical evaluation and hormonal workup (in collaboration with the Endocrinology department) are recommended, as specific workup or genetic analysis may be required.
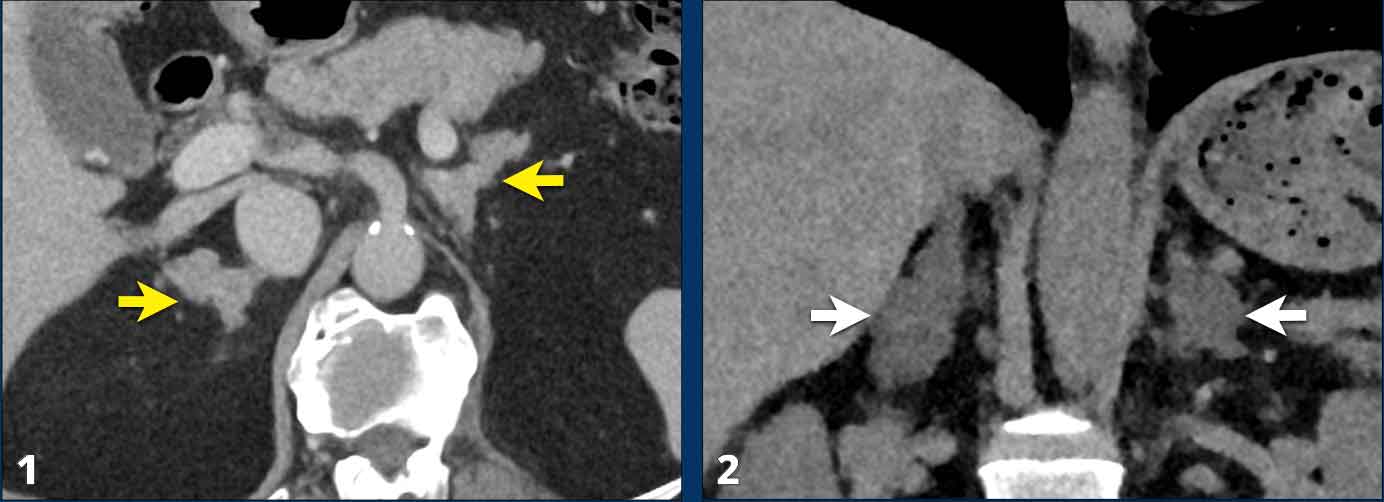
Case Presentation
- 78-year old male scanned for rectal bleeding. No other symptoms.
contrast-CT reveals bilateral macronodular enlargement, ultimately diagnosed as primary macronodular adrenocortical disease after endocrinological referral and workup. - 38-year old female suspected of appendicitis.
Non contrast CT reveals bilateral adrenal adenomas.
The lesions were not hormonally active.
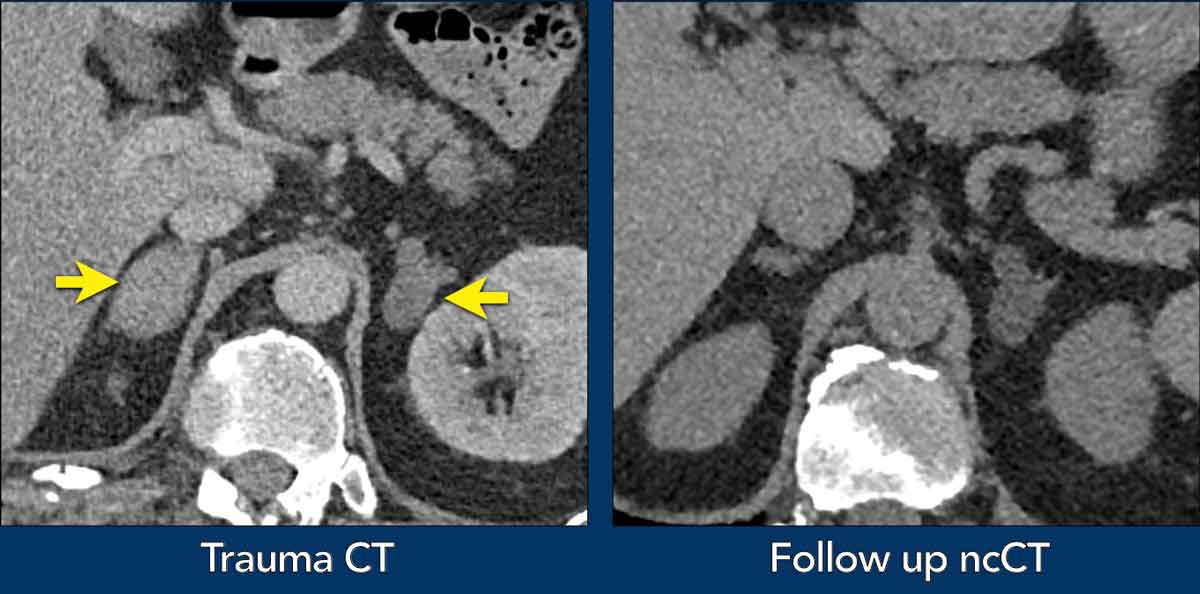
Case Presentation
A male patient presented after a motor vehicle accident.
- Contrast-enhanced trauma CT
Bilateral adrenal lesions.
Additional findings on the scan included a right-sided pneumothorax and rib fractures.
Hormonal workup was unremarkable - Follow-up: non-contrast CT (ncCT) performed 6 months later demonstrated resolution of the right adrenal hemorrhage with return to normal gland size and stable left adrenal adenoma (density: -11 HU)
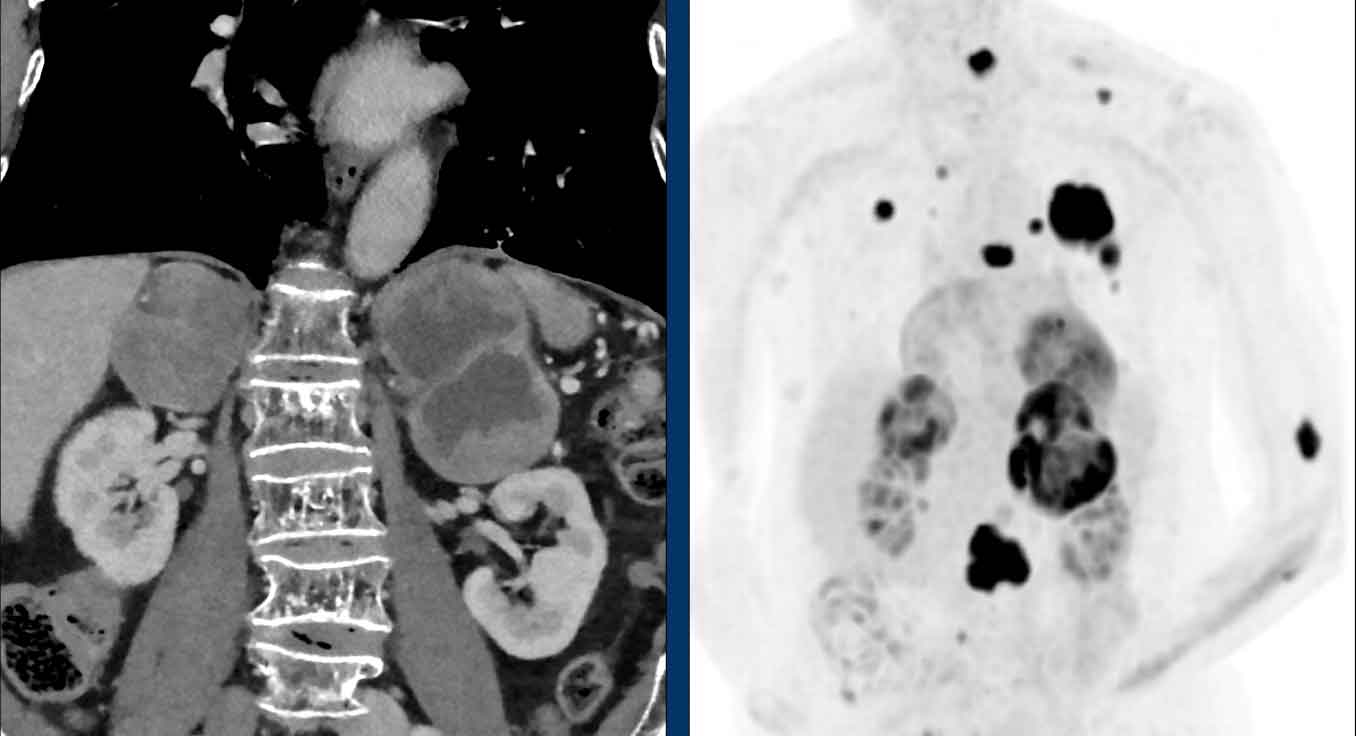
Case Presentation
A venous phase staging CT in an elderly male patient revealed bilateral large adrenal masses (6.3 cm and 8 cm) with heterogeneous enhancement and areas of central necrosis.
A subsequent FDG PET-CT demonstrated multiple markedly hypermetabolic lesions in the adrenal glands, lungs, skin, and bones.
Histopathology confirmed the primary tumor as melanoma.
Worrisome Features and Follow Up
Worrisome Features in Adrenal Tumors
- Heterogeneity
- Necrosis
- Irregular margins
- Signs of internal hemorrhage
- High density on non-contrast CT (particularly >40 HU)
- Size >4 cm (especially >6 cm)
- Significant interval growth:
- ≥5 mm in 6–12 months
- >20% increase in largest diameter in 12 months
Follow Up
Benign Adrenal Incidentalomas (No Further Imaging Follow-Up Required)
- Lipid-rich adenoma (~70% of adenomas; the remainder are lipid-poor adenomas with little or no microscopic fat).
- Myelolipoma.
- Cyst (well-defined, thin-walled; may contain calcifications).
Benign Adrenal Incidentalomas (Follow-Up Needed)
- Adrenal hemorrhage (if history supports: blunt trauma, anticoagulant use, or sepsis).
- If bilateral: Consider testing for adrenal insufficiency.
- Follow-up imaging: Recommended in 1–3 months to exclude an underlying tumor.
Malignant Adrenal Tumors
- Adrenocortical carcinoma
- Malignant pheochromocytoma
- Metastases
- Lymphoma (usually non-Hodgkin lymphoma; often bilateral)
- Collision tumor (rare; coexisting benign and malignant lesions in the same adrenal gland)