Suprahyoid Neck - Anatomy and Pathology
Marjorie van Kooten, Jeroen Vister, Marius Kok, Marjolein Lamers, Frank Pameijer and Robin Smithuis.
Radiology department of the University Medical Centre of Utrecht, the Rijnstate Hospital in Arnhem and the Alrijne hospital in Leiden, the Netherlands
Publicationdate
In this article we will focus on a 3-step approach on how to analyze pathology of the suprahyoid neck on cross-sectional imaging based on the anatomical spaces.
- Step 1. In which space is the lesion.
- Step 2. What is the normal contents of that space.
- Step 3. Which pathology can originate from these structures.
Finally assess whether the lesion demonstrates a characteristic imaging pattern on ultrasound (cystic or solid), CT (density, enhancement) or MRI (T1/T2 signal intensities, diffusion restriction) and evaluate if the imaging findings are consistent with the clinical presentation.
Introduction
Anatomy
The neck is divided into suprahyoid and infrahyoid compartments because most deep cervical spaces terminate at the hyoid level, and different pathologies predominate in each region.
The suprahyoid neck extends from the hyoid to the skull base, while the infrahyoid neck spans from the hyoid to the thoracic inlet.
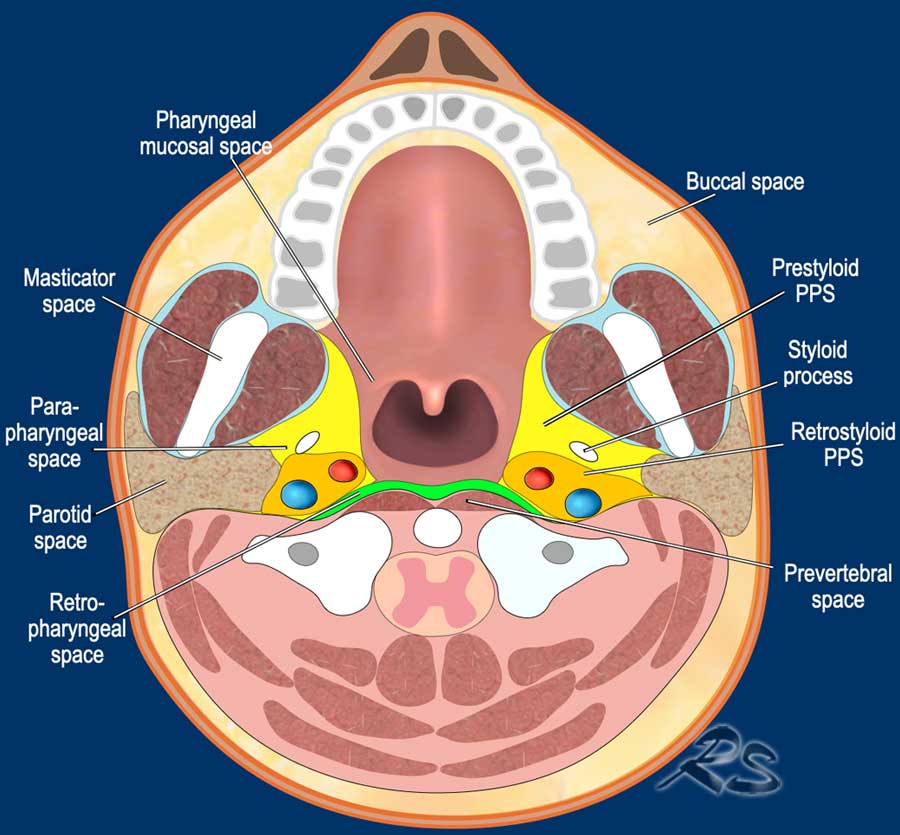
The suprahyoid neck is divided into 8 deep cervical spaces:
- Buccal space
- Masticator space
- Parotid space
- Parapharyngeal space
- Carotid space (or retrostyloid parapharyngeal space)
- Retropharyngeal space - a virtual space posterior to the pharyngeal mucosa extending from the skull base to the mediastinum.
- Perivertebral space - is part of the perivertebral space, which also includes paraspinal components.
The cervical neck spaces are delineated by surrounding fascial planes.
As a rule pathological processes are typically confined to a specific anatomical space, which aids in localizing disease, narrowing the differential diagnosis, and anticipating potential routes of spread.
Exceptions to this rule include:
- Pathology that may extend across fascial boundaries: venolymphatic malformations, squamous cell carcinoma, and infections.
- Multifocal disease: lymphatic metastases.
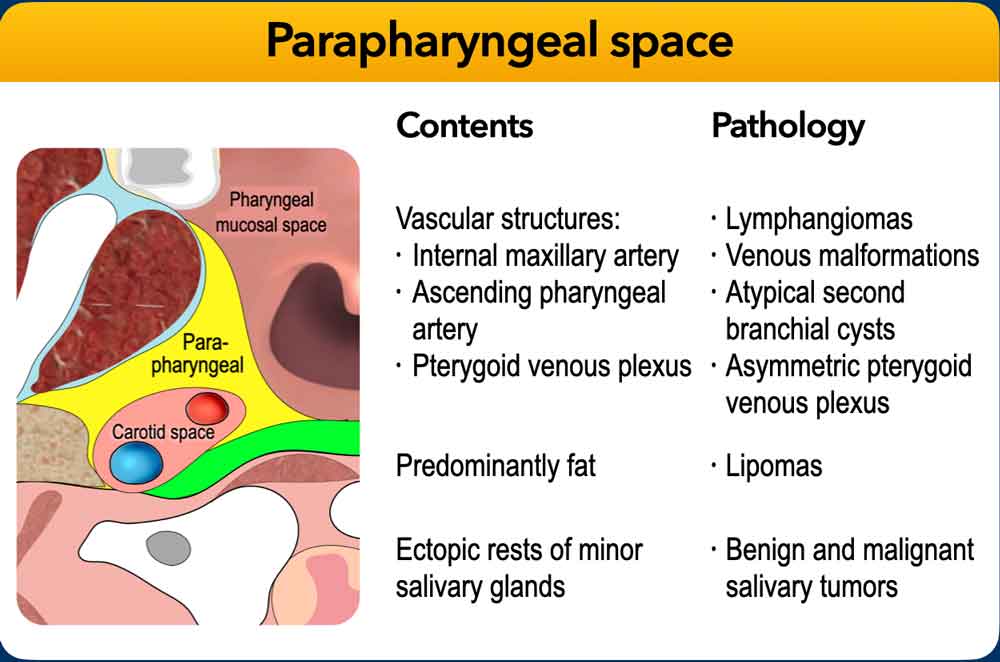
Parapharyngeal space
The parapharyngeal space needs our special attention as it is a key anatomical landmark for localizing neck pathology.
This fat-filled compartment is clearly visible on both CT and MRI.
Due to its central location on each side of the neck, it is often involved or compressed by lesions from adjacent spaces.
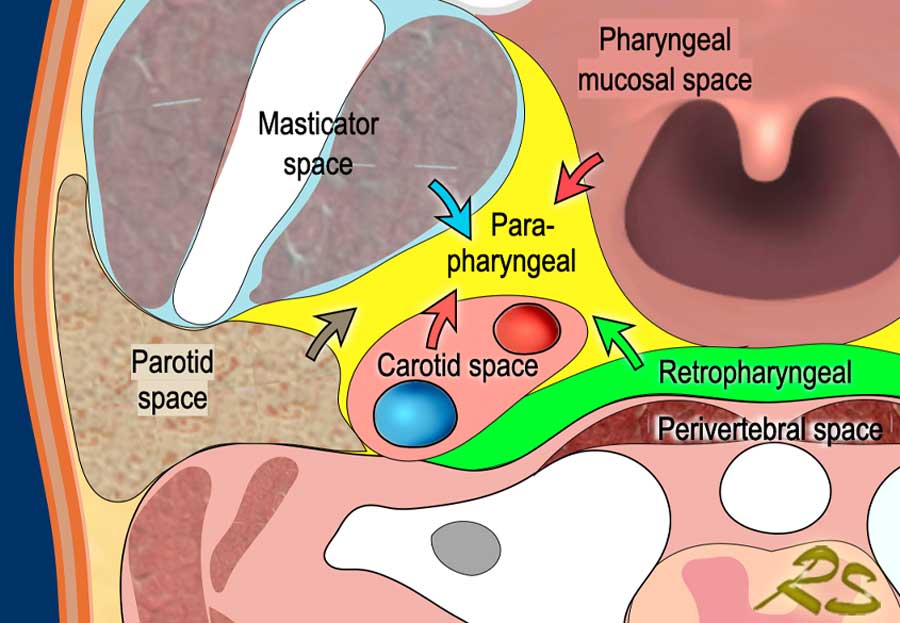
The pattern of parapharyngeal fat displacement helps determine the origin of a mass (figure).
Examples
- Retropharyngeal lesions typically displace fat anterolaterally (green arrow).
- Masticator space lesions displace fat posteromedially (blue arrow).
- Parotid space lesions displace fat medially/anteromedially (brown arrow).
- Carotid space lesions displace fat anteriorly/anteromedially (red arrow).
- Pharyngeal mucosal space lesions displace fat posterolateral (red arrow).
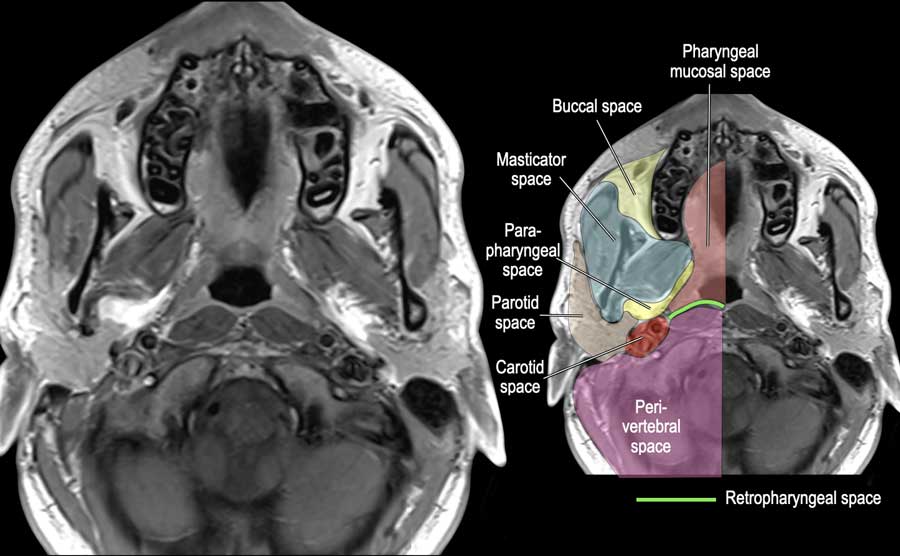
This MRI image demonstrates a cross-section at the level of the maxilla.
Note the fat-containing parapharyngeal space (highlighted in yellow) and the virtual retropharyngeal space (demarcated by the green line).
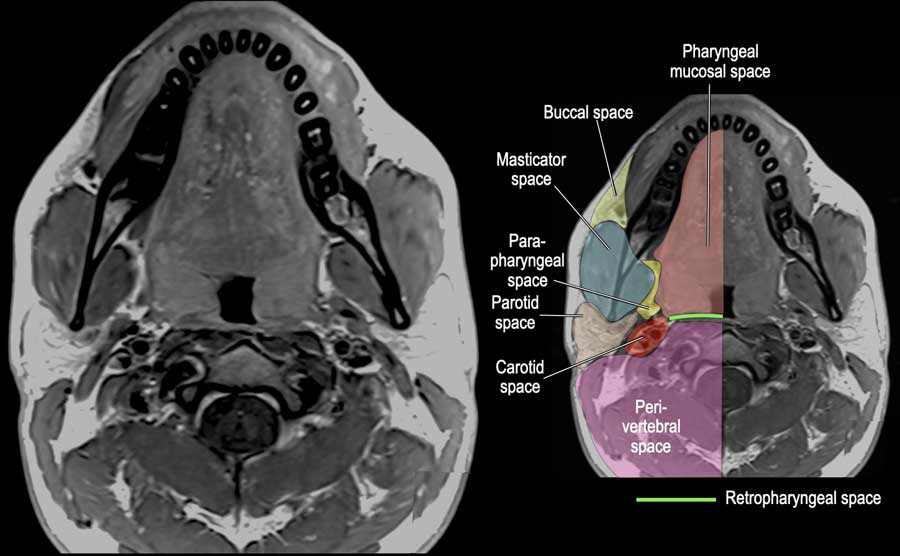
This MRI image demonstrates a cross-section at the level of the mandible.
Note the fat containing parapharyngeal space (yellow) and the virtual retropharyngeal space (green line).
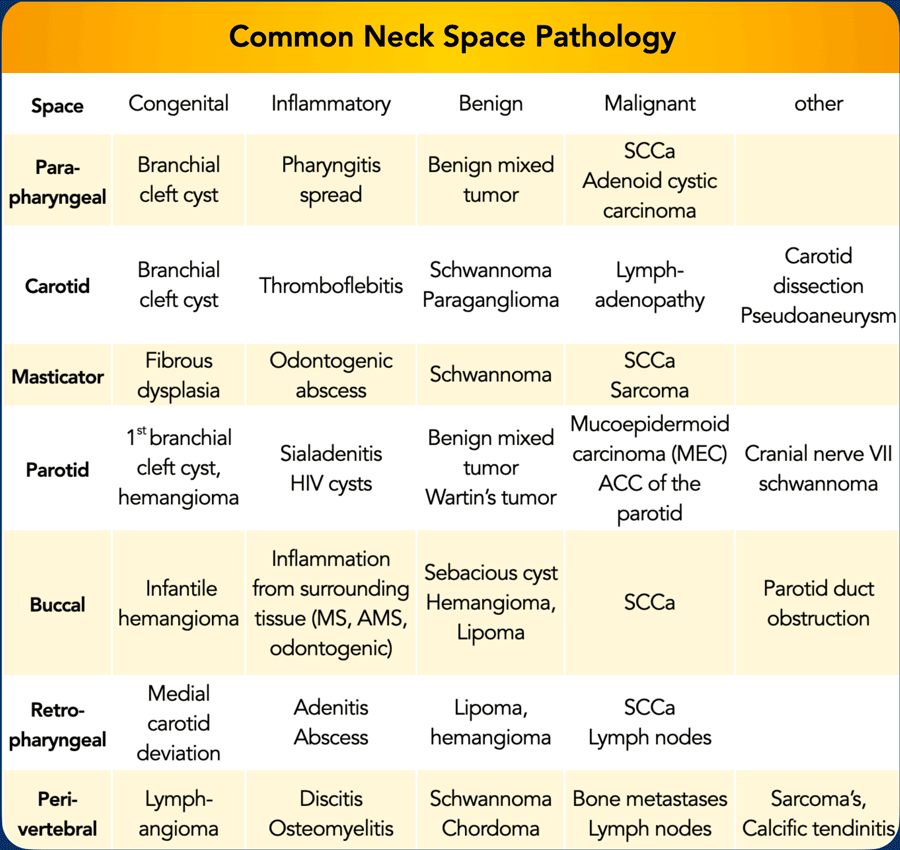
Common Pathology
Table summarizing common pathology types for each suprahyoid space of the neck, divided into congenital, inflammatory, benign, malignant and miscellaneous categories.
Reference: Yousem, David M.. “Suprahyoid spaces of the head and neck.” Seminars in roentgenology 35 1 (2000): 63-71.
Systematic approach
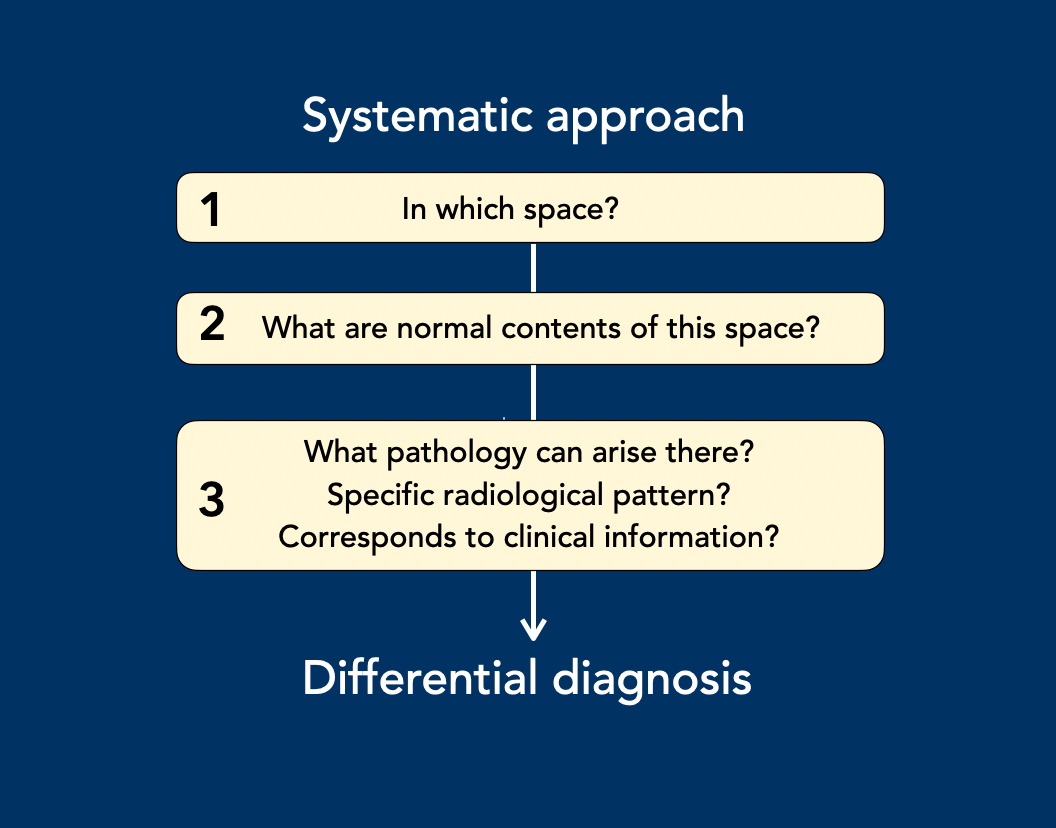
The evaluation of suprahyoid neck pathology follows a structured 3-step approach:
- Localization: Determine the anatomical neck space in which the lesion is situated.
- Anatomical Context: Identify the normal anatomical structures and contents of that space.
- Pathological Correlation: Consider which pathologies typically arise from these structures.
Tissue-specific considerations:
- Fat: May give rise to lipoma or liposarcoma.
- Muscle: May result in rhabdomyosarcoma.
- Lymph and blood vessels: May be the origin of enlarged lymph nodes, lymphatic malformations, or vascular malformations.
- Nerves: May give rise to schwannoma.
Imaging Assessment:
Evaluate whether the lesion demonstrates a characteristic imaging pattern on:
- Ultrasound: Cystic or solid.
- CT: Density, enhancement.
- MRI: T1/T2 signal intensities, diffusion restriction.
Final Step:
Assess whether the radiologic findings are consistent with the clinical presentation.
Buccal space
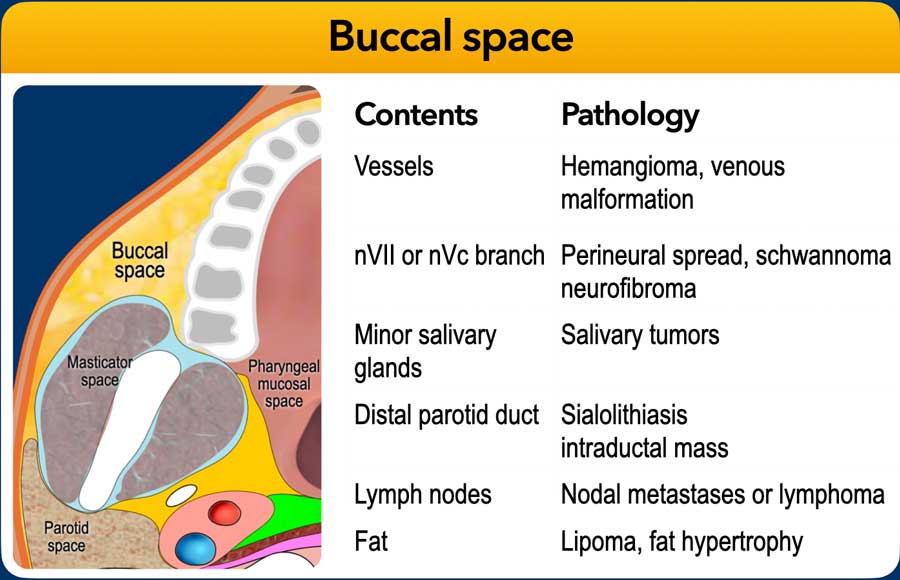
The buccal space is a superficial, predominantly fat-filled compartment that is incompletely enclosed by fascia. Inferiorly, it is in direct contact with the submandibular space. Due to its small size and primarily adipose contents, this space often receives less attention than other neck compartments.
Primary lesions in the buccal space are most commonly salivary gland tumors, both benign and malignant, typically arising from minor salivary glands. Malignant lymph nodes should also be considered in the differential diagnosis.
Important mimics include an accessory parotid gland, which is present in approximately 20% of individuals and may simulate a buccal space mass. A dilated parotid duct, secondary to an obstructing stone or intraductal tumor, can also present similarly. Notably, most Stensen’s duct stones are radiopaque, and sialolithiasis is more frequently encountered in the submandibular and sublingual ducts.
Infectious processes in the buccal space may originate from dental or periodontal infections.
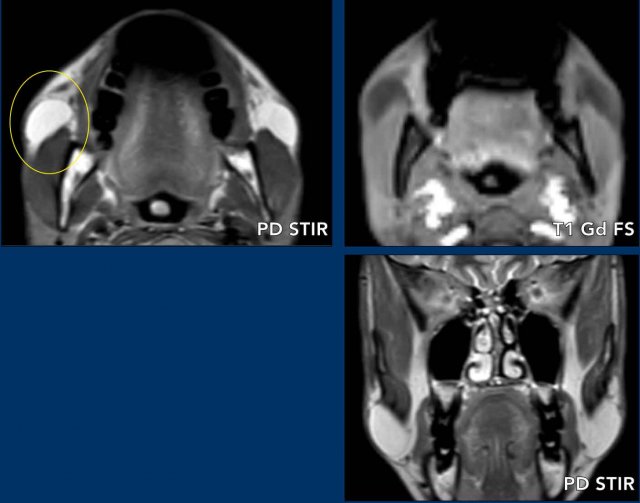
Buccal fat pad
Case presentation
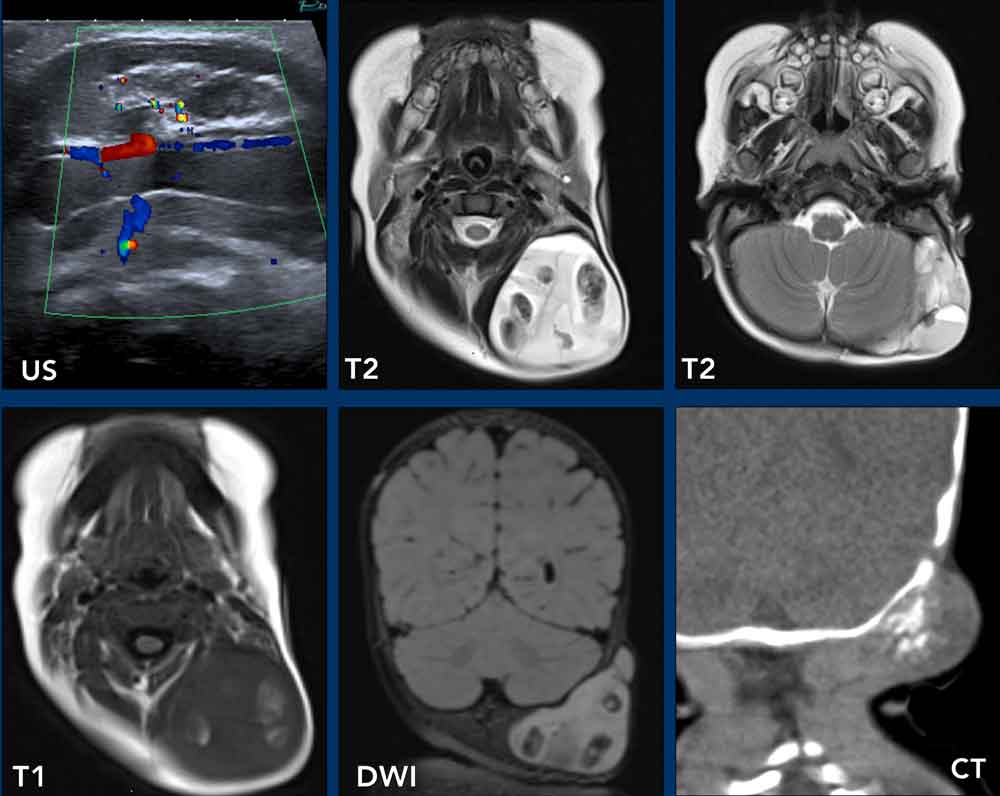
A 32-year-old female presents with symmetrical swelling of both cheeks.
Imaging
- Location: Buccal space
- Normal contents: Fat, lymph nodes, minor salivary glands, blood vessels, and nerves.
- MRI: symmetrical lesions within the buccal spaces, exhibiting signal characteristics identical to fat on all sequences shown.
Final diagnosis
Findings are consistent with hypertrophy of the buccal fat pads (Bichat’s fat pads).
Subsequent evaluation revealed Cushing’s disease, a condition that strongly supports the diagnosis of fatty hypertrophy.
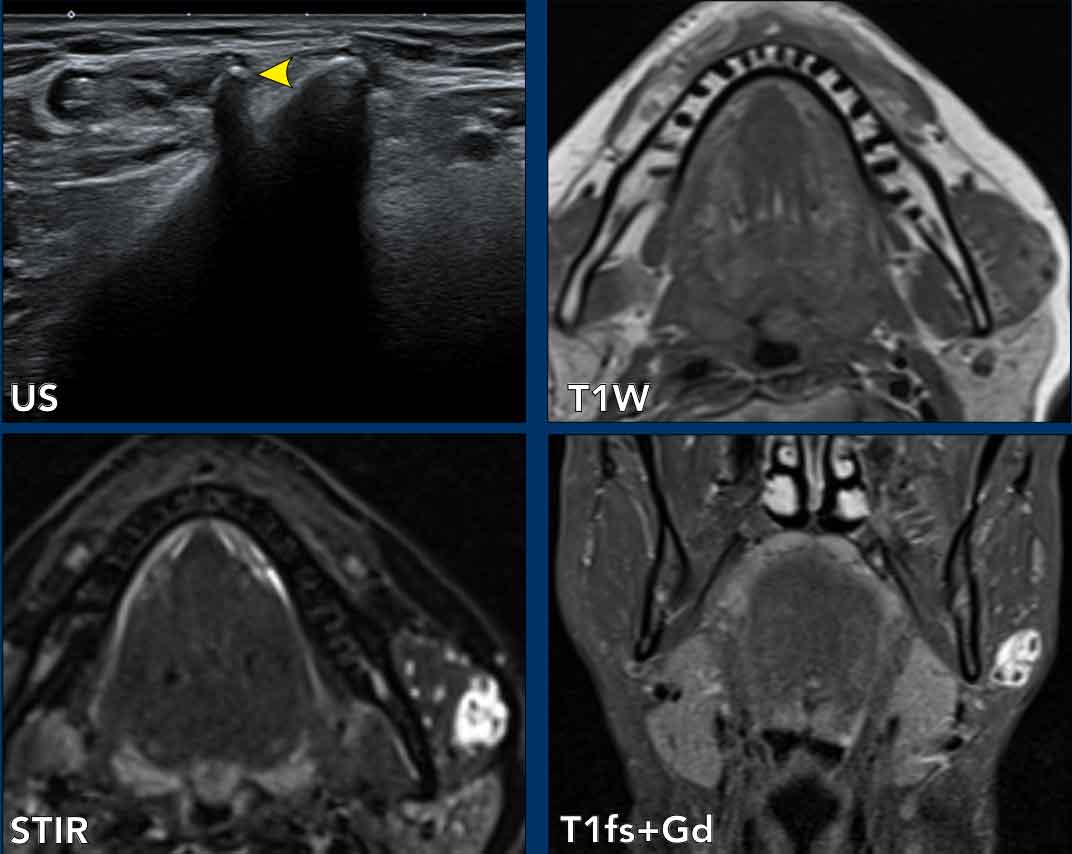
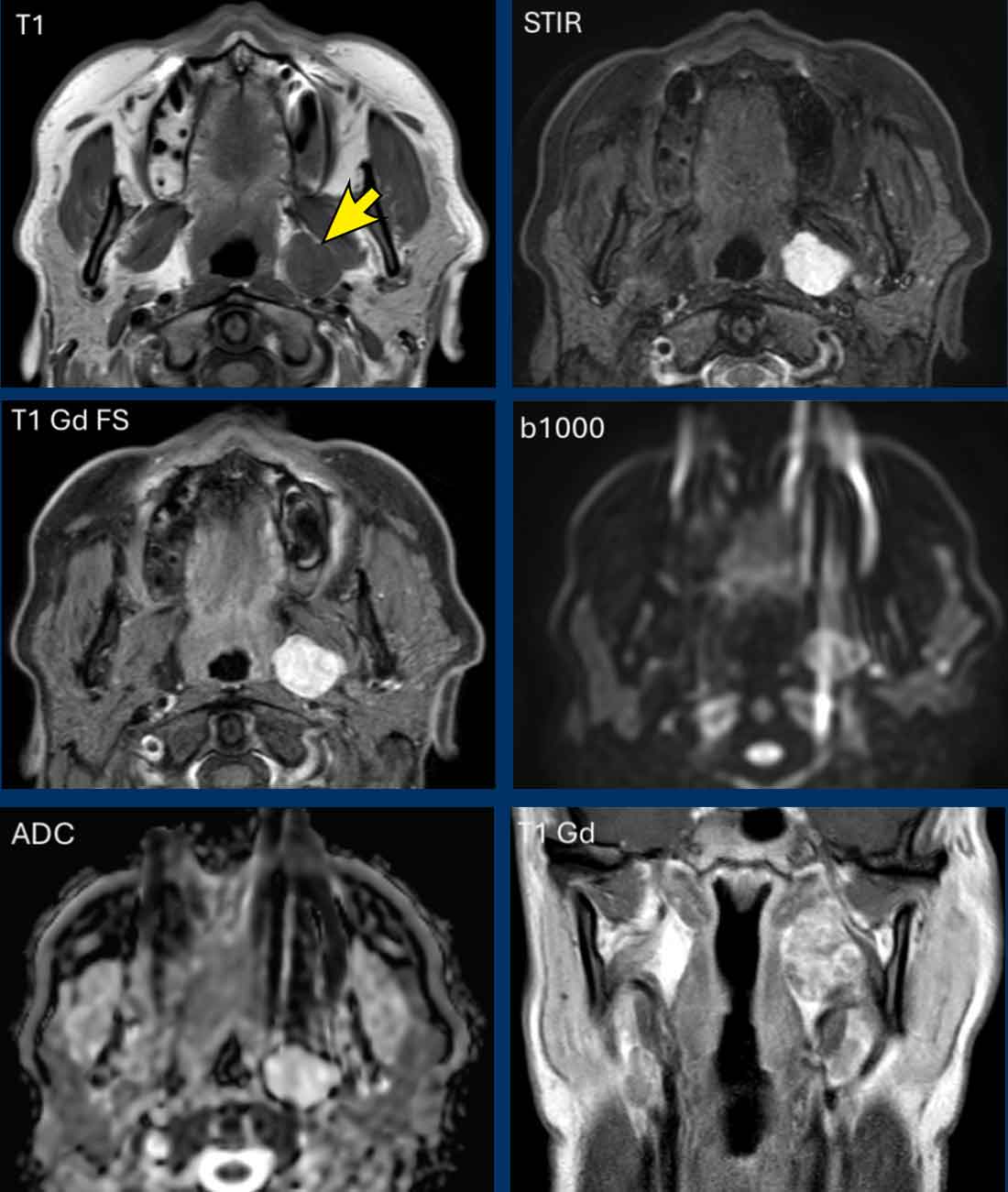
Salivary gland tumor
Case presentation
A 28-year-old man with a long-standing swelling of the left cheek.
Imaging
- Location: Buccal space
- Normal contents: Fat, lymph nodes, accessory parotid gland , facial blood vessels, buccal branches of facial and trigeminal nerves.
- MRI: T1: Iso-intense to muscle, distinct from subcutaneous fat (lipoma unlikely). T2/STIR: High signal intensity. Post-contrast T1: Solid enhancement.
Differential Diagnosis
- Cyst – unlikely (because of the solid enhancement).
- Lipoma – excluded (no fat signal on T1).
- Hemangioma – unlikely (no calcifications, typically larger).
- Favored diagnosis – minor salivary gland tumor (pleomorphic adenoma most likely).
Final diagnosis
US-guided FNA: Pleomorphic adenoma.
In this location however, it is a rare lesion.

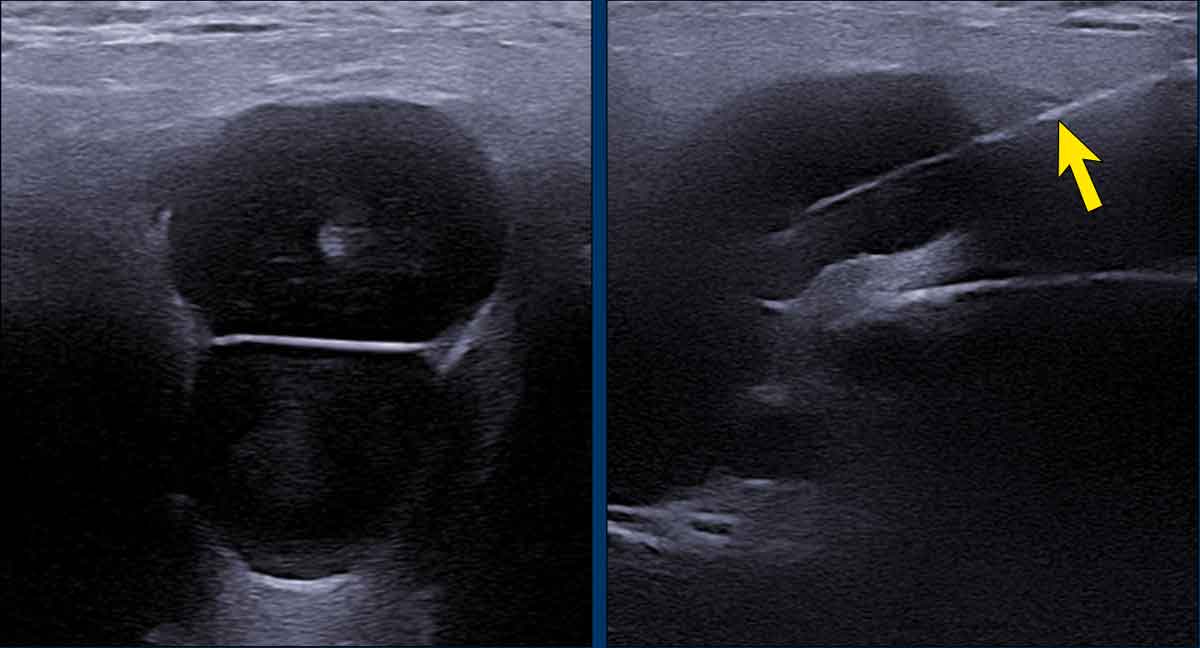
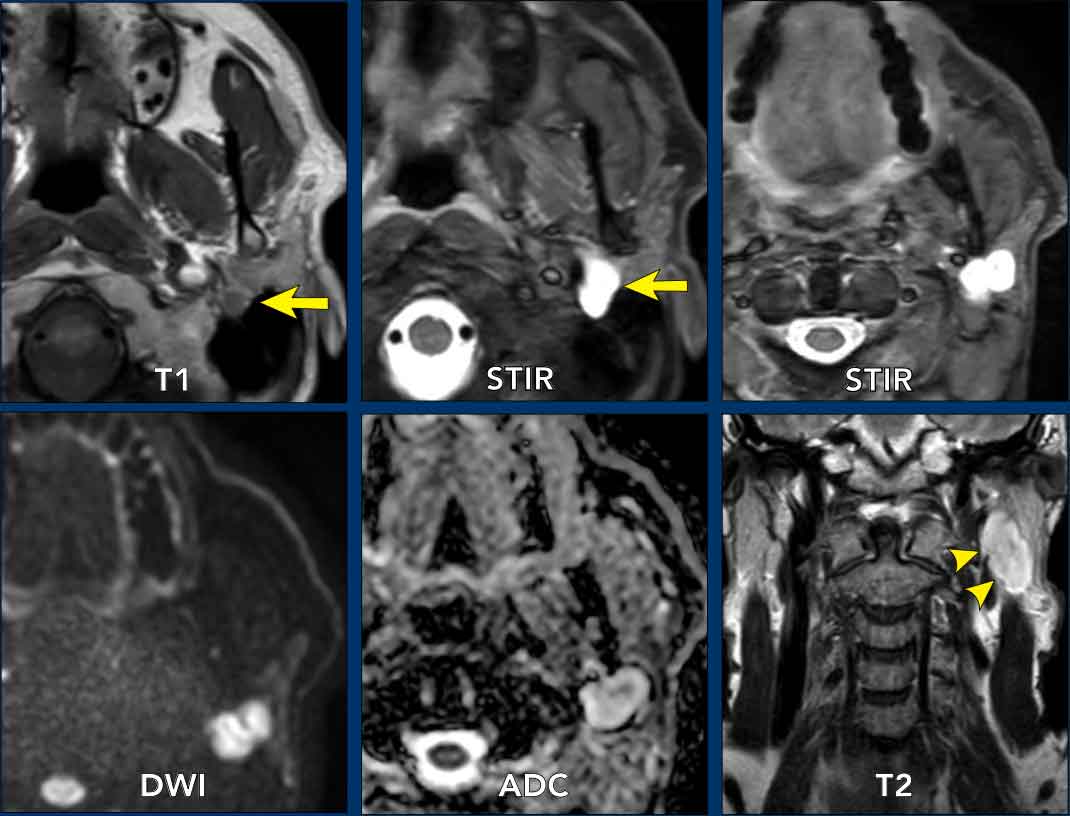
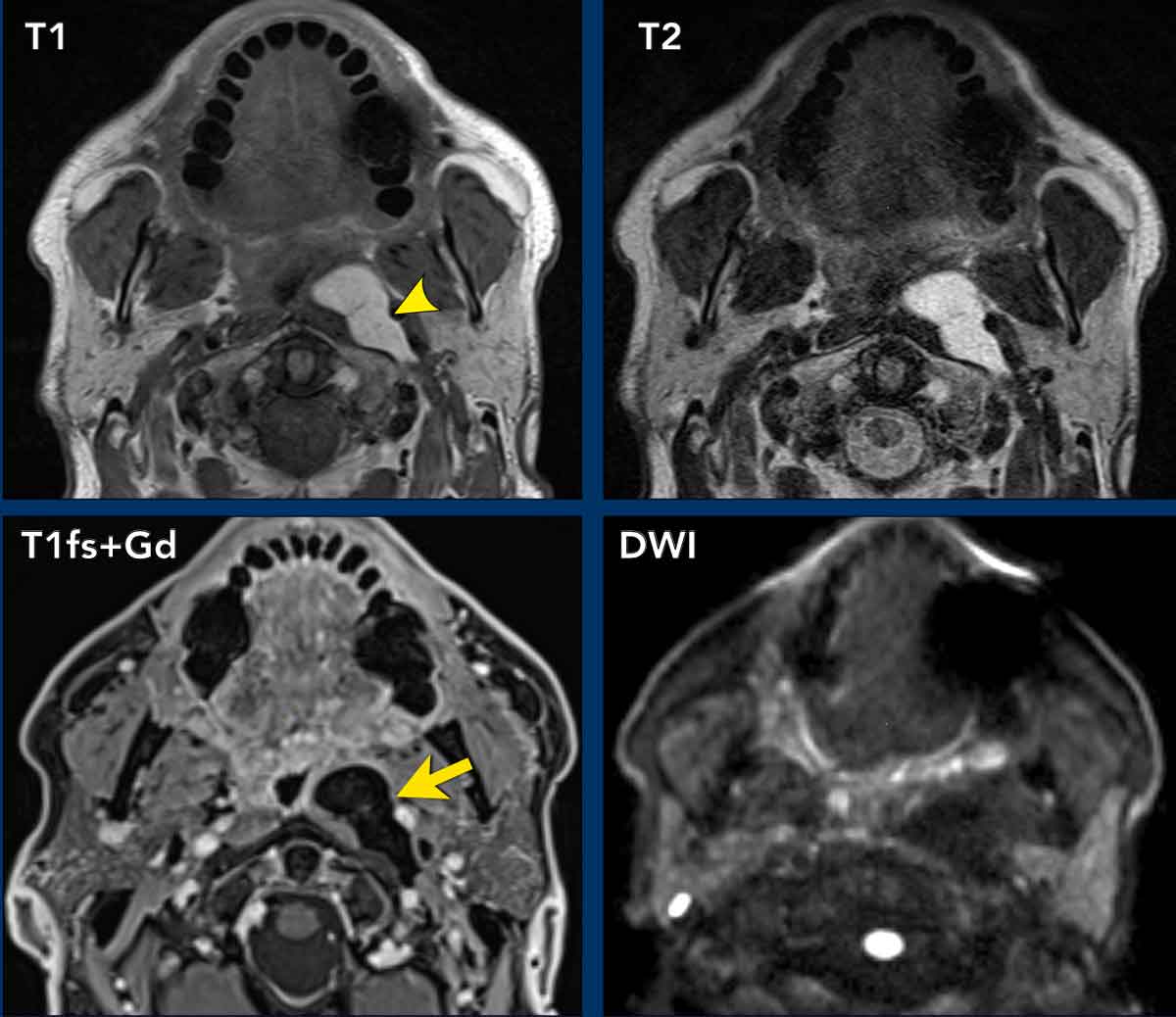
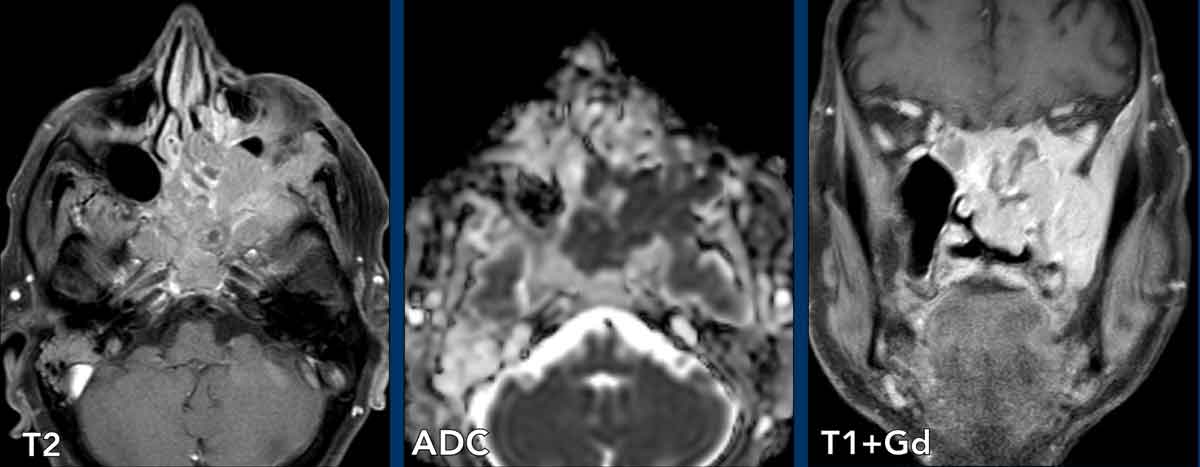
Lymph node metastasis
Case presentation
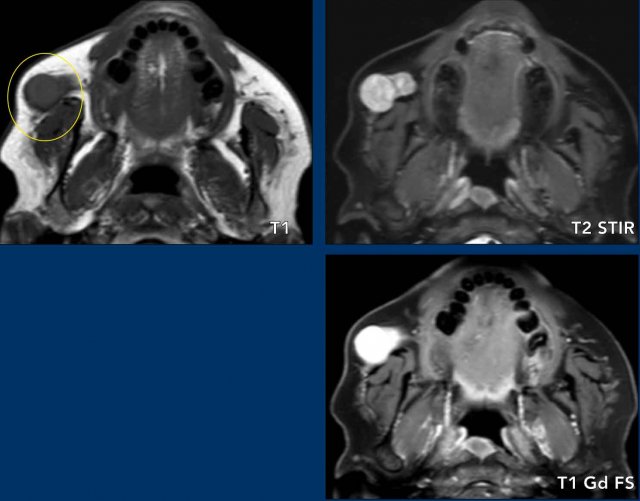
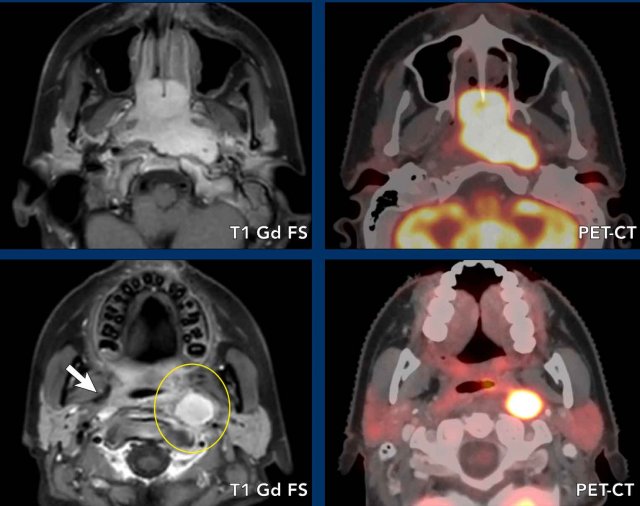
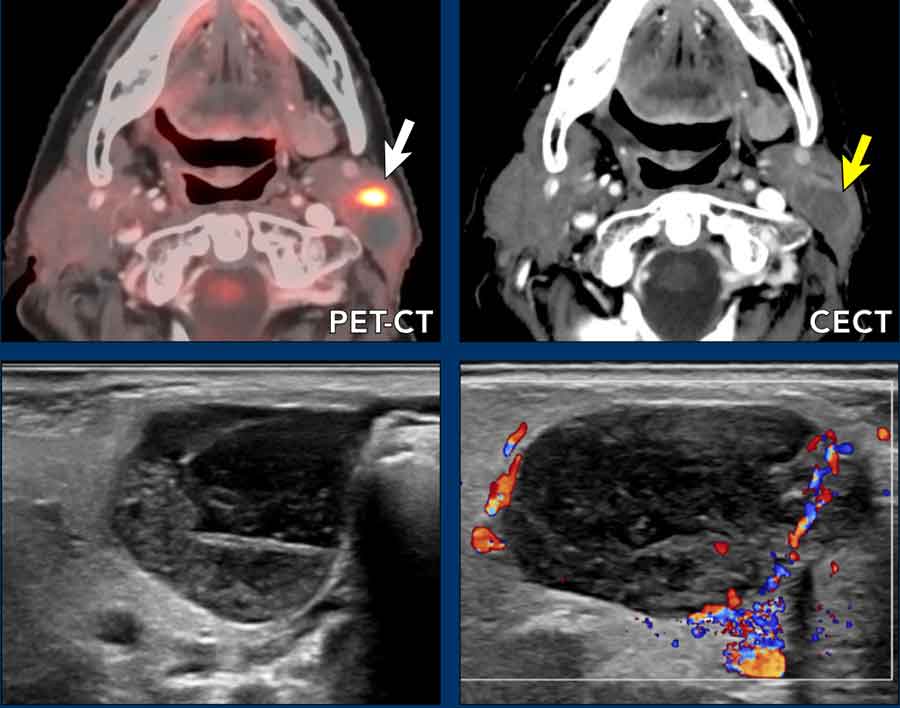
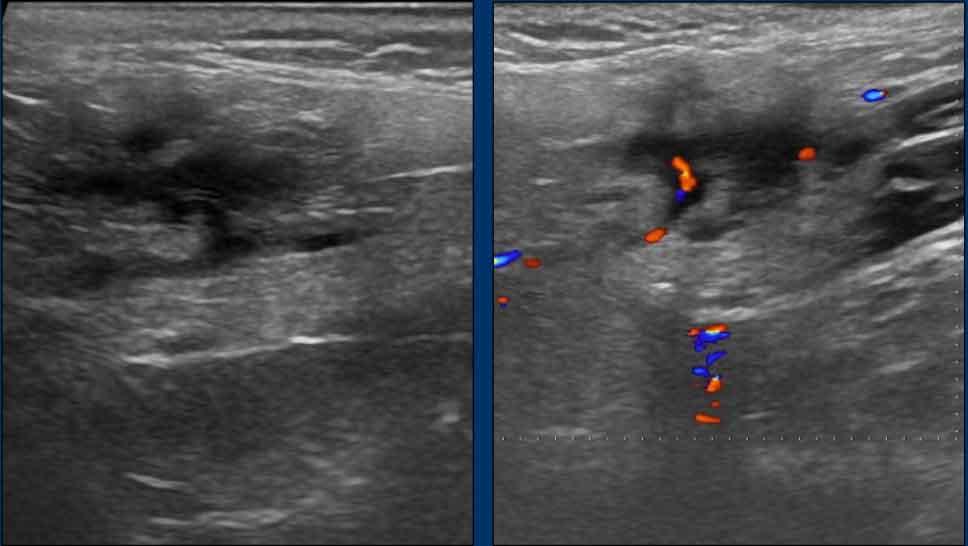
A 40-year-old male with a six-week history of right cheek swelling. Biopsy of maxillary mass: squamous cell carcinoma. MRI performed for local staging and nodal assessment.
Imaging
- Location: Buccal space
- Normal contents: Fat, lymph nodes, accessory parotid gland, facial blood vessels, buccal branches of facial and trigeminal nerves.
- MR Findings: Right buccal space – round, well-defined enhancing lesion with diffusion restriction (ADC not shown here) and marked PET avidity (images 1–3).
- Right maxillary sinus – enhancing mass with lateral wall bony destruction and soft-tissue extension into the right cheek (image 4, arrow).
Differential diagnosis
- Given known primary maxillary squamous cell carcinoma, the buccal space mass is most likely a metastatic lymph node.
- Salivary gland tumor: more often has a sharp border.
- Lymphoma: more often homogenous enhancement and sharp border.
Final diagnosis US-guided FNA confirmed metastatic squamous cell carcinoma.
Teaching Point During neck ultrasound in sinonasal malignancies, include the buccal region to assess for nodal disease.
Facial fillers
Case presentation
A 56-year-old female with prior facial filler injections in Syria presents with heavy eyelids.
Imaging
- Location: Buccal space
- Normal contents: fat, lymph nodes, minor salivary glands, vessels, nerves)
- Findings
MRI: Widespread subdermal material in the face, including bilateral buccal fat pads, more pronounced on the right; high T2 signal characteristic of filler material.
PET-CT: Increased FDG uptake in these areas, likely reflecting low-grade chronic inflammation or foreign body reaction (arrow).
Teaching Point
Facial fillers are artificial and do not represent normal buccal space anatomy, so the standard 3-step anatomical assessment is not fully applicable. Recognition of their imaging appearance is important, given rising prevalence.
Retropharyngeal space
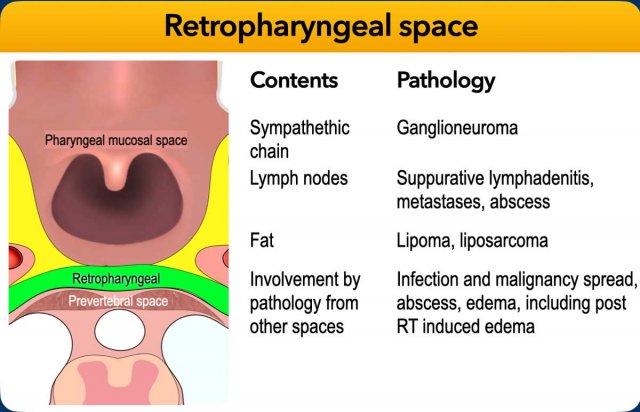
The retropharyngeal space is a potential compartment extending from the skull base to the upper mediastinum (T1–T2 level), bounded anteriorly by the posterior pharyngeal wall and posteriorly by the prevertebral fascia.
It permits supero-inferior movement of the larynx, pharynx, and esophagus relative to the cervical spine.
Lesions in this space typically displace parapharyngeal fat anterolaterally.
Retropharyngeal lymph nodes may become involved in oropharyngeal infections, leading to suppurative lymphadenitis and potential rupture with abscess formation.
They may also harbor metastases from squamous cell carcinoma of the nasopharynx, posterior oropharyngeal wall, soft palate, or hypopharynx.
Lipoma
Case presentation
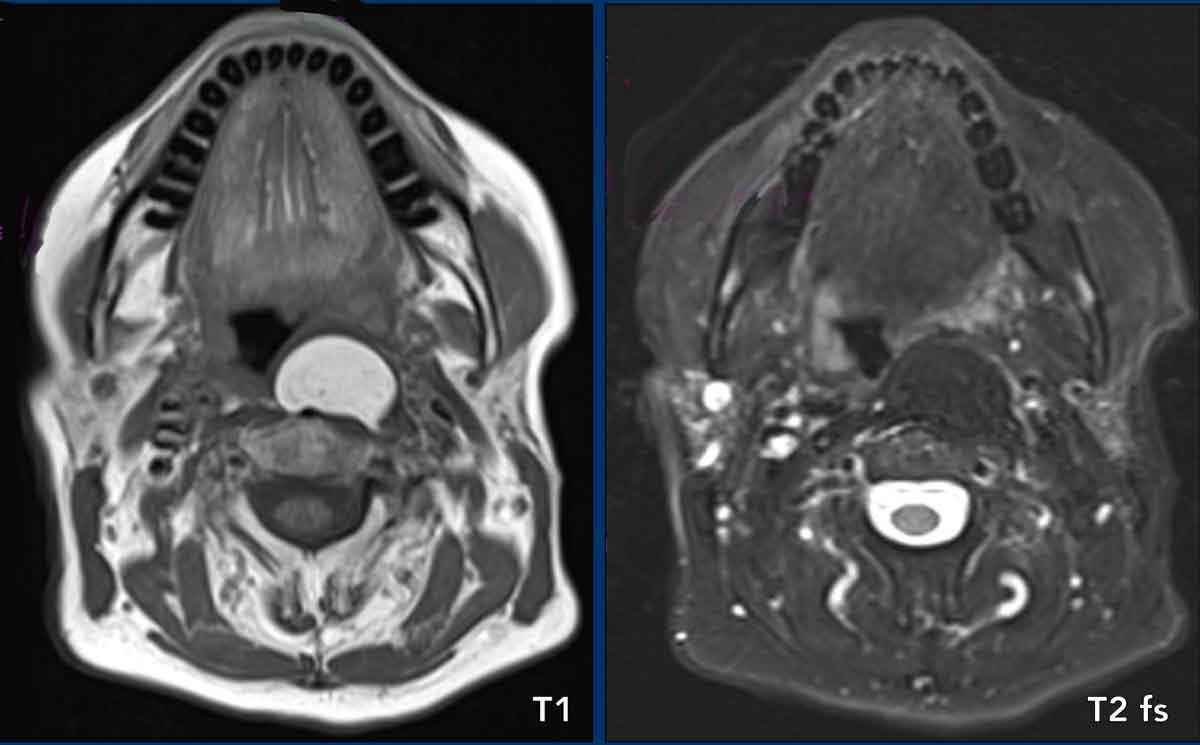
A patient with obstructive sleep apnea syndrome.
Imaging
- Location: the lesion displaces the parapharyngeal fat anterolateral and we see mass effect on the longus colli muscles from anterior, indicating that the lesion originates from the retropharyngeal space.
- Normal contents: Fat, lymph nodes, sympathetihic chain.
- Findings: Sharply demarcated mass in the left retropharyngeal space. Bright on T1, low signal on fat suppressed T2 indicative of a simple lipoma.
The space-specific differential diagnosis is:
- Lymph node: usually not hyperintense on the T1.
- Ganglioneuroma: tend to have homogenous low/intermediate signal on T1 and heterogenous on T2.
- Lipoma: following the signal of fat, most likely diagnosis.
Final diagnosis
Lipoma.
Biopsy: fat and muscle cells (no malignancy).
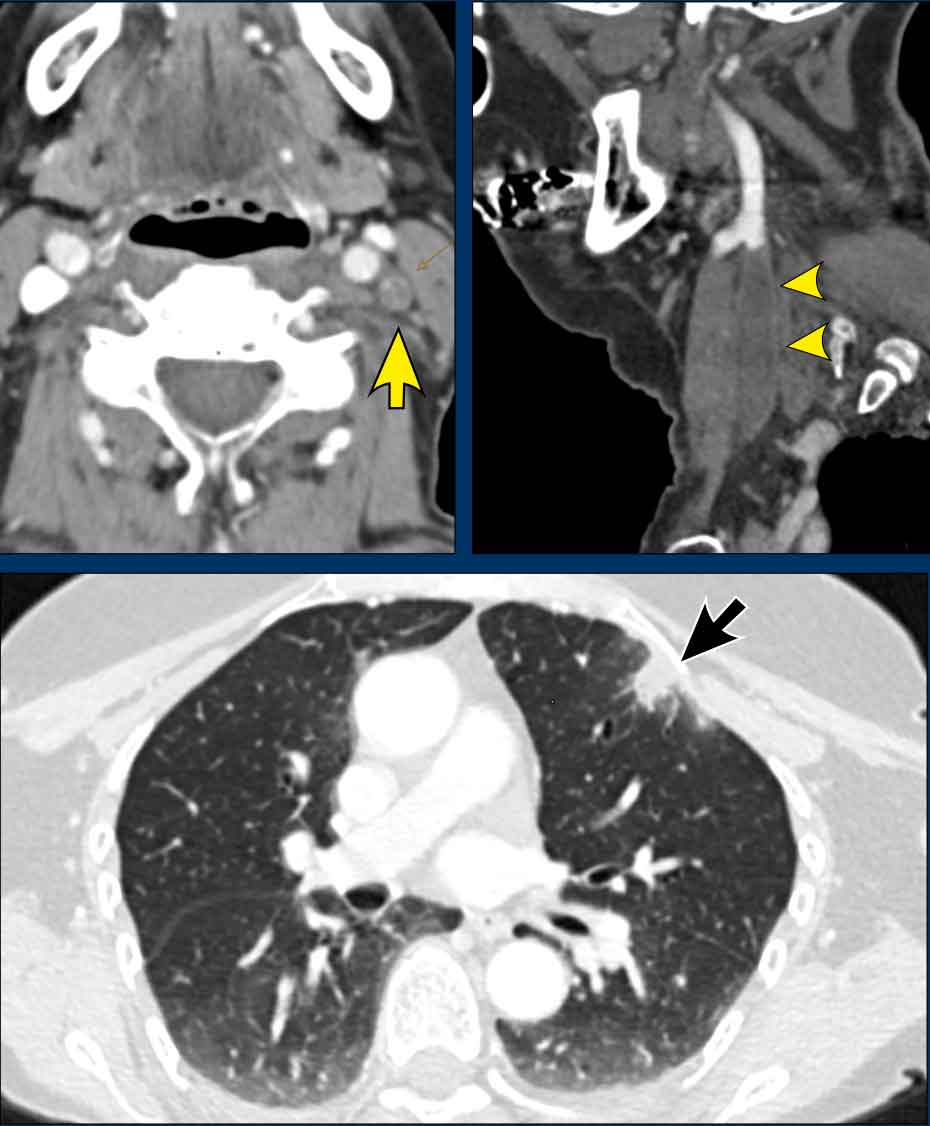
Lymph node metastasis
Case presentation
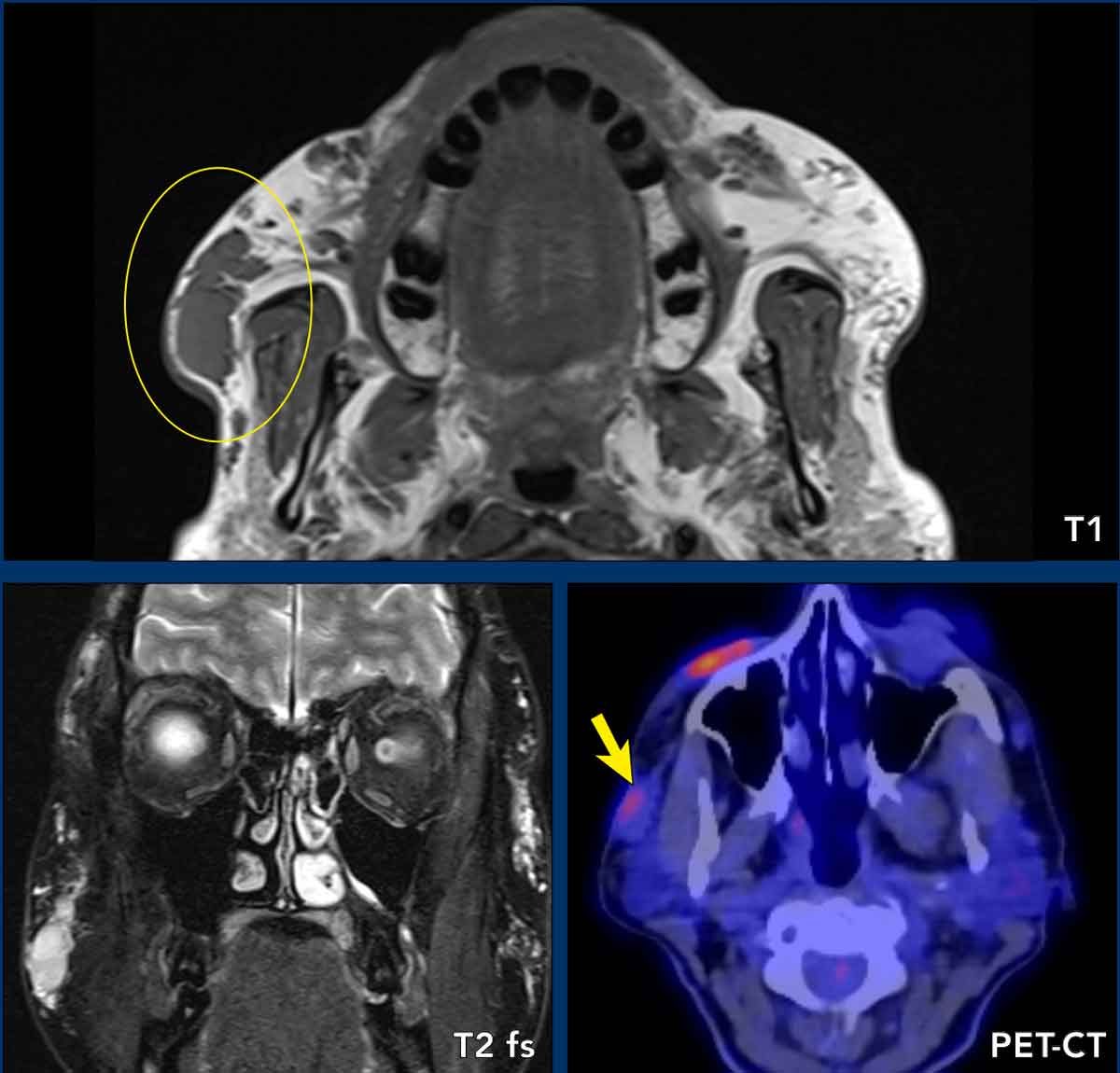
18-year-old female with nasal obstruction.
Imaging
- Location: the lesion displaces the parapharyngeal fat anterriorly and we see mass effect on the longus colli muscles from anterolateral, indicating that the lesion originates from the retropharyngeal space.
- Normal contents: Fat, lymph nodes, sympathetic chain.
- Findings
- Nasopharyngeal level (upper images) - Gadolinium-enhanced, fat-suppressed MRI demonstrated a large bilateral nasopharyngeal mass with left parapharyngeal extension and anterior spread through both choanae. PET/CT fusion images showed corresponding hypermetabolic activity.
- Oropharyngeal level (lower images) - The lesion displaced parapharyngeal fat anterolaterally and flattened the longus colli muscles, indicating origin in the retropharyngeal space. The internal carotid artery was displaced laterally.
Impression
Space-specific differential diagnosis for a retropharyngeal mass included:
- Ganglioneuroma: Typically demonstrates absent to heterogeneous enhancement and no FDG uptake.
- Lymph node metastasis: Most likely etiology. The node was enlarged and rounded, without surrounding inflammatory changes such as edema or fat stranding.
Final Diagnosis
Biopsy-confirmed EBV-positive nasopharyngeal carcinoma.
Treatment and Follow-up
Proton beam radiotherapy.
Three-year follow-up: complete remission.
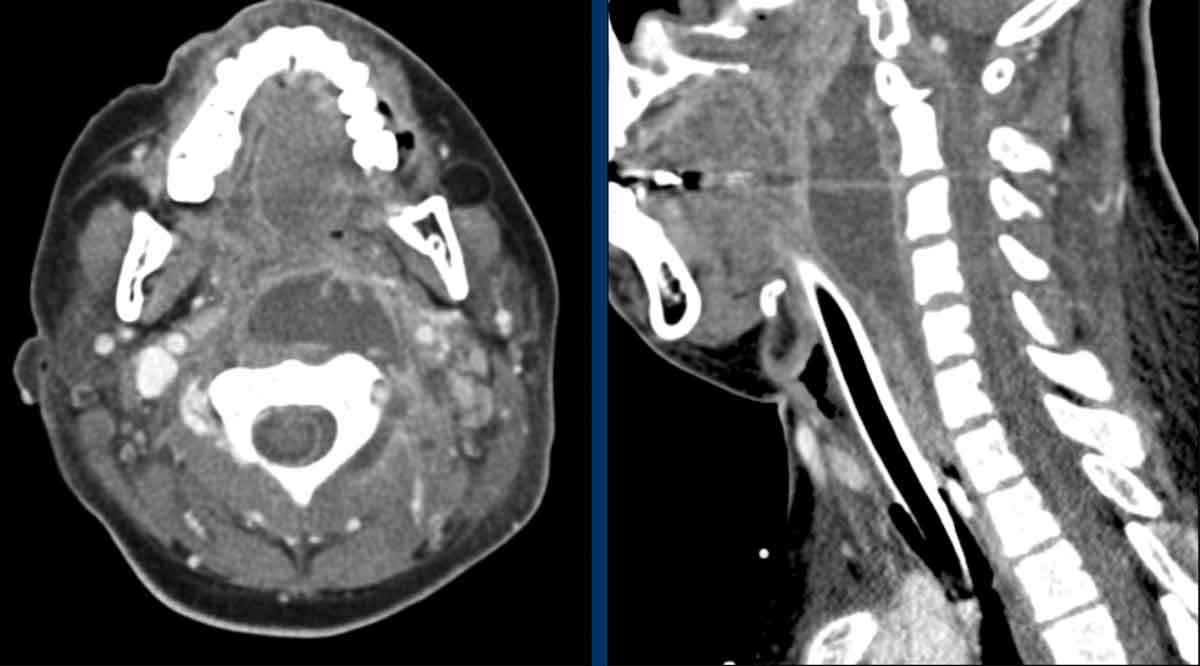
Retropharyngeal abscess
Case presentation
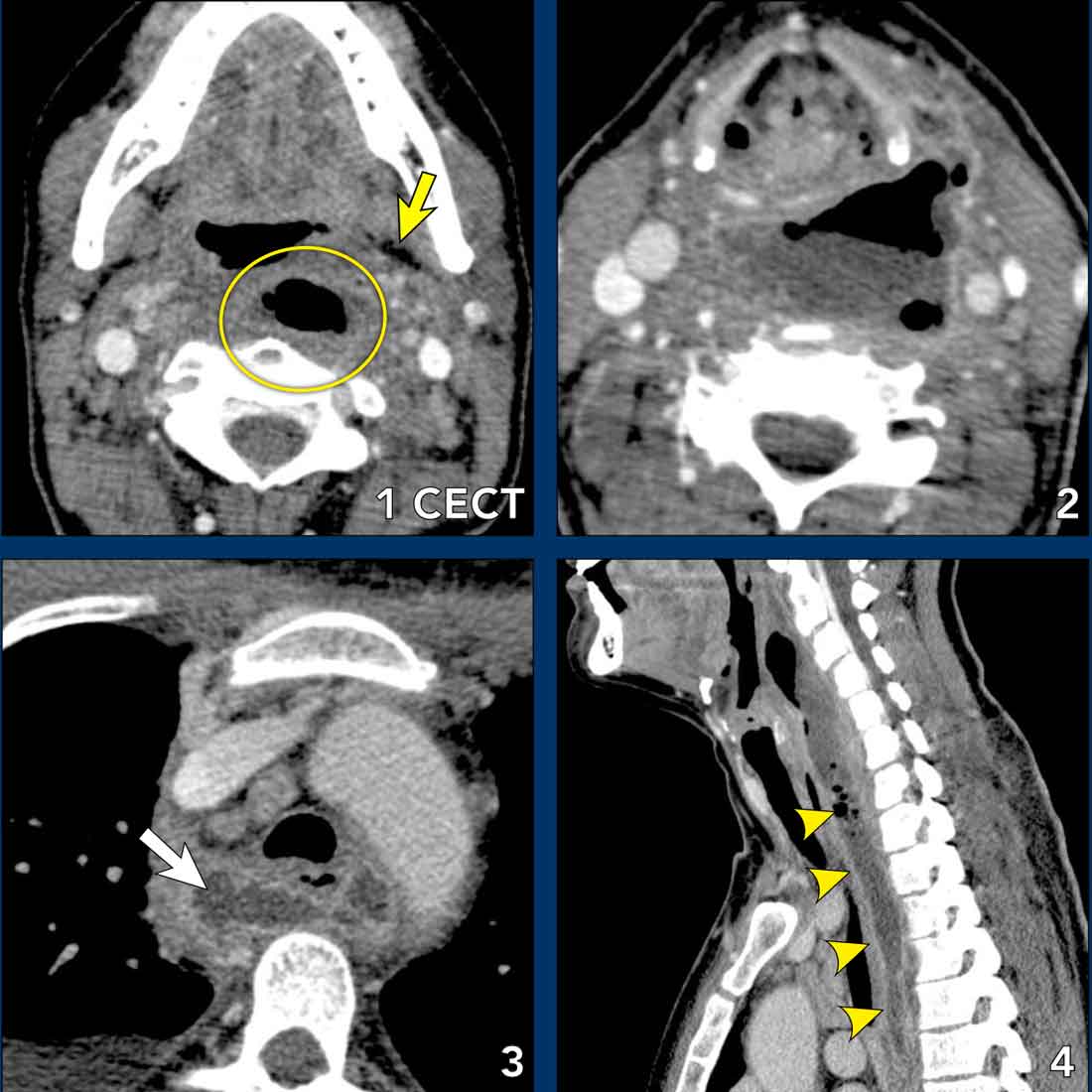
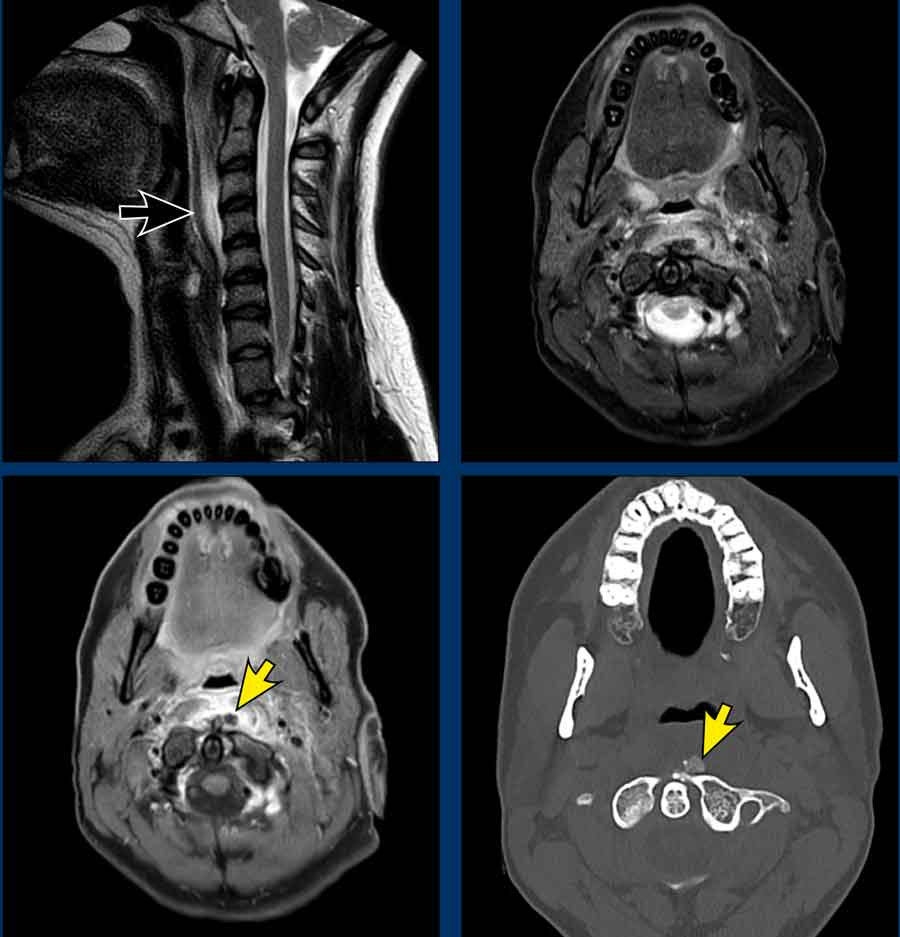
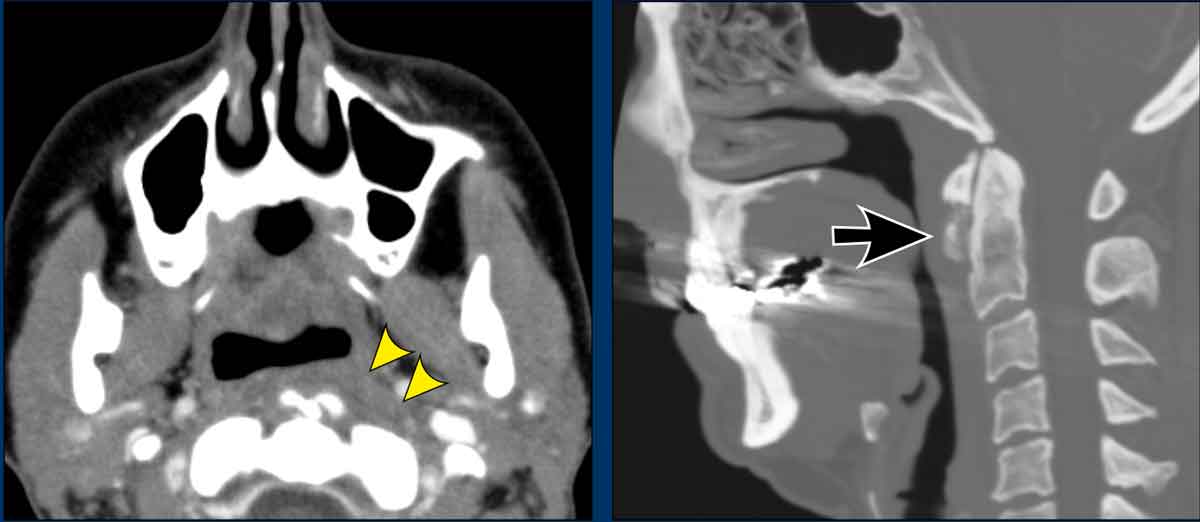
A 31-year-old female with progressive throat pain and dysphagia two days after falling downstairs with a dishwashing brush in her mouth, which was removed in the emergency department.
Imaging
- Location: Contrast-enhanced CT demonstrates anterolateral displacement of the parapharyngeal fat (yellow arrow on image 1)and lateral displacement of the carotid space, indicating a retropharyngeal origin.
- Normal contents: Fat, lymph nodes, sympathetic chain.
- Findings: CT shows a rim-enhancing fluid collection with an air–fluid level extends from the oropharynx to the posterior mediastinum (arrowheads image 4)—consistent with typical retropharyngeal spread due to absence of fascial barriers.
Impression
Findings favored retropharyngeal abscess over hematoma.
- Hematoma: Typically hyperdense, heterogeneous.
- Abscess: Rim enhancement, surrounding tissue induration—most likely in this case.
Notes
True retropharyngeal abscesses are uncommon. Etiologies include suppurative lymphadenitis, direct extension from mucosal injury, peritonsillar abscess, or hematogenous spread.
Potential Complications
- Prevertebral extension → osteomyelitis
- Carotid artery or jugular vein thrombosis
- Airway compromise
- Mediastinitis
- Grisel syndrome (non-traumatic atlantoaxial subluxation secondary to local inflammation)
Retropharyngeal suppurative lymphadenitis
Case
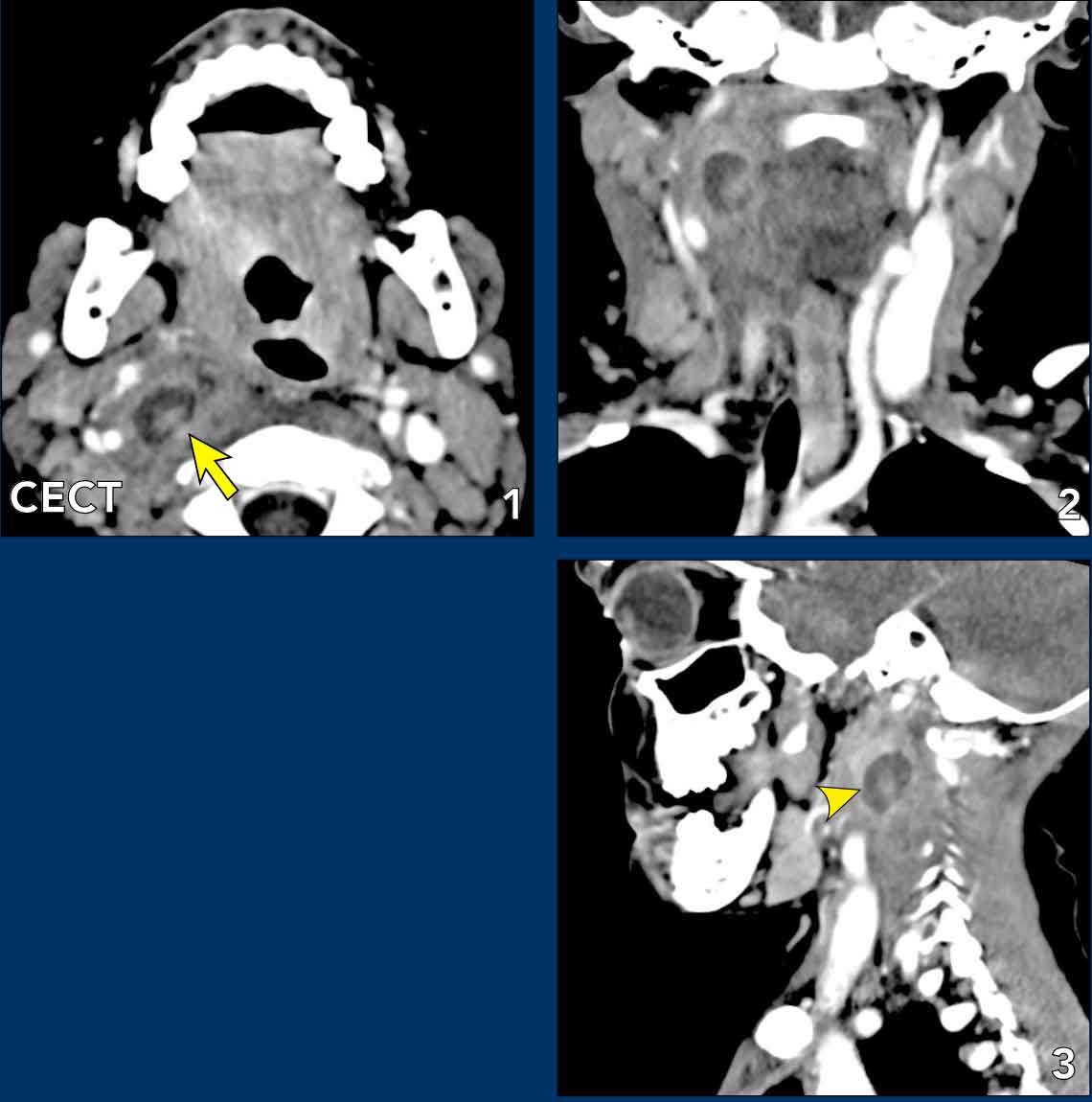
A 4-year-old presents with one week of fever and throat pain, followed by onset of torticollis one day prior to admission. Initial CT suggested a retropharyngeal abscess; however, surgical exploration revealed no pus.
Imaging
- Location: Contrast-enhanced CT demonstrates anterolateral displacement of the parapharyngeal fat and lateral displacement of the carotid space, indicating a retropharyngeal origin.
- Normal contents: Fat, lymph nodes, sympathetic chain.
- Findings ontrast-enhanced CT demonstrated anterolateral displacement of parapharyngeal fat and lateral displacement of the internal carotid artery and jugular vein, consistent with a retropharyngeal origin. The lesion appeared hypodense with some central enhancement indicative of suppuration.
Differential Diagnosis
- Abscess: Typically has central hypodensity with inferior extension along the path of least resistance, rather than a focal mass.
- Suppurative lymphadenitis: Usually more laterally positioned within the retropharyngeal space.
Note
Distinguishing suppurative lymphadenitis from abscess on imaging is challenging, potentially leading to unnecessary surgery. Correlation with clinical findings is essential.
Treatment and Outcome
The patient was managed successfully with intravenous antibiotics and made a full recovery.
Neck phlegmon
Case
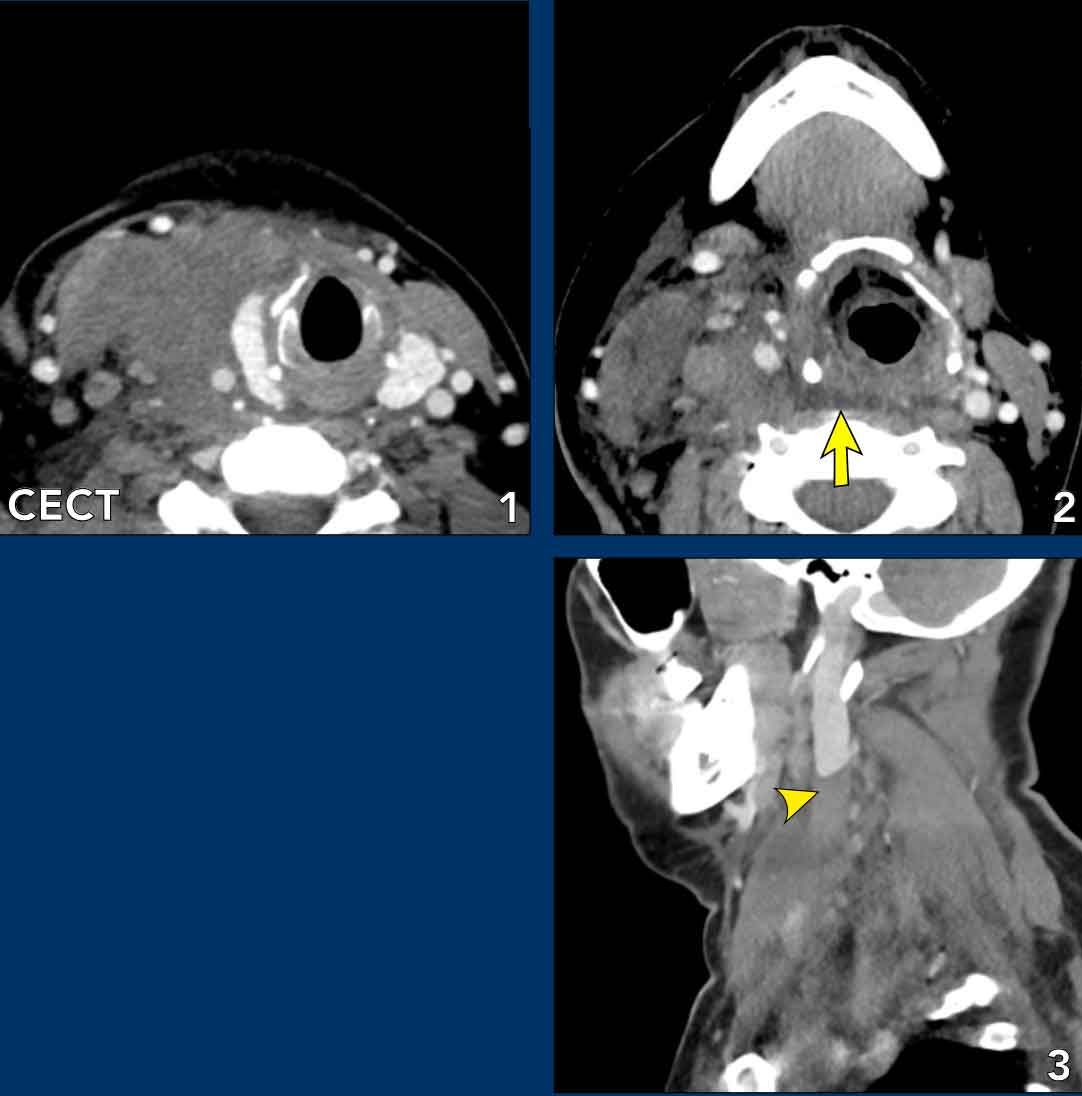
A 37-year-old female presents with progressive swelling on the right side of the neck.
Imaging
- Location: at the level of the hyoid bone (image 2), there is anterolateral displacement of the parapharyngeal fat and vascular structures and compression on the longus colli muscles, consistent with a lesion originating in the retropharyngeal space. Additionally, splaying of the vascular structures is observed, suggesting involvement of the retrostyloid parapharyngeal space (as indicated by the yellow arrow on image 2).
- Normal contents: Fat, lymph nodes, sympathetic chain.
- Findings
- Diffuse hyperdense swelling of the right side of the neck (image 1).
- At the level of the hyoid the entire retropharyngeal space demonstrates a diffuse hyperdense appearance relative to the expected fatty density of this region (arrow on image 2). No focal mass or encapsulation is identified.
- Jugular vein thrombosis as a result of compression by the infection (arrowhead on image 3).
Impression
The space-specific differential diagnosis is:
- Abscess: typically encapsuled (not present here).
- Hematoma: usually more hyperdense and heterogenous.
- Phlegmone: diffuse infiltration of fat causing diffuse increased density, most likely diagnosis in this case.
Final Diagnosis
Neck phlegmon with retropharyngeal edema and secondary thrombosis of the jugular vein.
Treatment and Follow-up
The patient was treated with IV anticoagulation and antibiotics, resulting in full recovery.
Parotid space
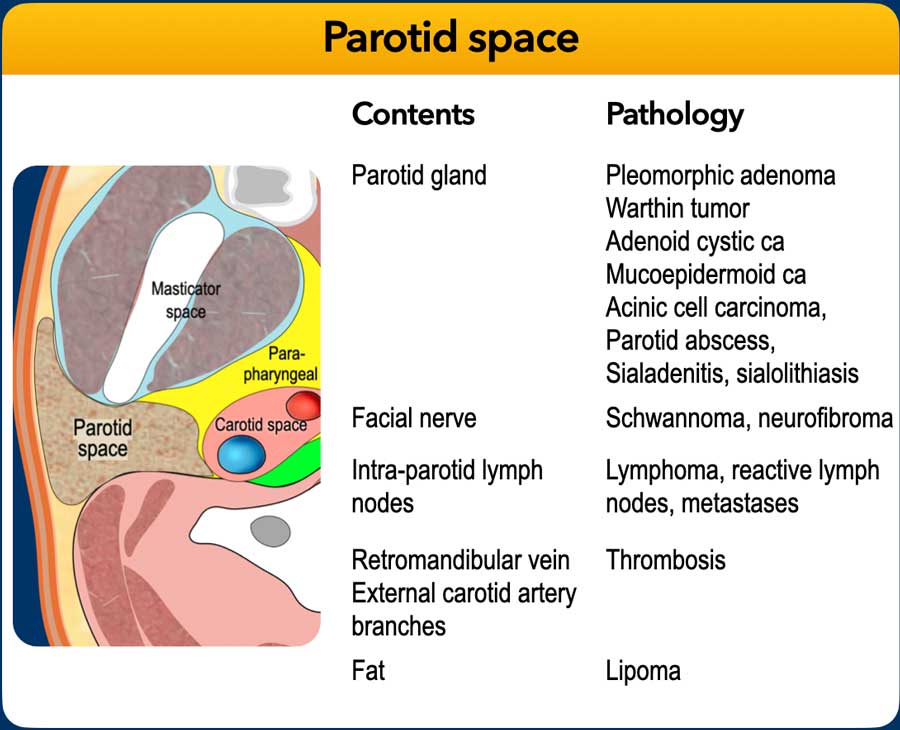
Parotid Space Anatomy
The parotid gland is the dominant structure in the parotid space and is divided into superficial and deep lobes by the facial nerve.
The deep lobe extends medially toward the parapharyngeal space, a key consideration in tumor spread.
Common Masses and Tumors
The most frequent parotid mass is a normal intraparotid lymph node.
Over 80% of parotid tumors are benign, typically pleomorphic adenoma (most common), or Warthin tumor (often bilateral).
Imaging alone rarely differentiates benign from malignant lesions, as some malignancies (e.g., acinic cell carcinoma, adenoid cystic carcinoma) may grow slowly, mimicking benign masses.
Imaging Features Suggestive of Malignancy
- Irregular borders
- Diffusion restriction
- Low T2 signal
- Adjacent tissue invasion
- Perineural spread along facial nerve branches, especially toward the stylomastoid foramen.
- Lymphadenopathy
Diagnostic Workup
The primary strengh of imaging (ultrasound, CT, MRI, PET-CT) in parotid lesions lies not necessarily in predicting the exact histology, but in assessing tumor extention, resectability, perineural spread and lymph node involvement.
Fine-needle aspiration (FNA) is recommended when a lesion is not clearly a lymph node.
Cytology or histopathology remains essential for a definitive diagnosis. A complicating factor is the heterogeneous cellular composition of parotid lesions, which increases the risk of sampling error.
- Fine-needle aspiration (FNA) is less invasive and often used as the first step.
- Core needle biopsy should be considered in cases of (repeatedly) non-diagnostic or inconclusive cytology.
Branchial cleft cyst.
Case
A 39-year-old female noticed an fluctuating swelling at the angle of the right jaw.
Imaging
- Location: on the left image (1) a lesion is (partially) located within the parotid gland, making it a parotid space content lesion.
- Normal contents: Fat, lymph nodes, salivary gland tissue, neurovascular bundle.
- CT Findings: Well-defined, hypodense cystic lesion with a thin rim in the right parotid gland. May show a sinus tract to the skin, EAC or parapharyngeal space.
Differential Diagnosis
- Parotid neoplasm with cystic degeneration
- Abscess
- Cystic lymph node metastasis
Conclusion
The thin wall and extension towards the skin make it most likely a first branchial cleft cyst.
Pathology:
Postsurgical examination confirmed a cystic lesion.
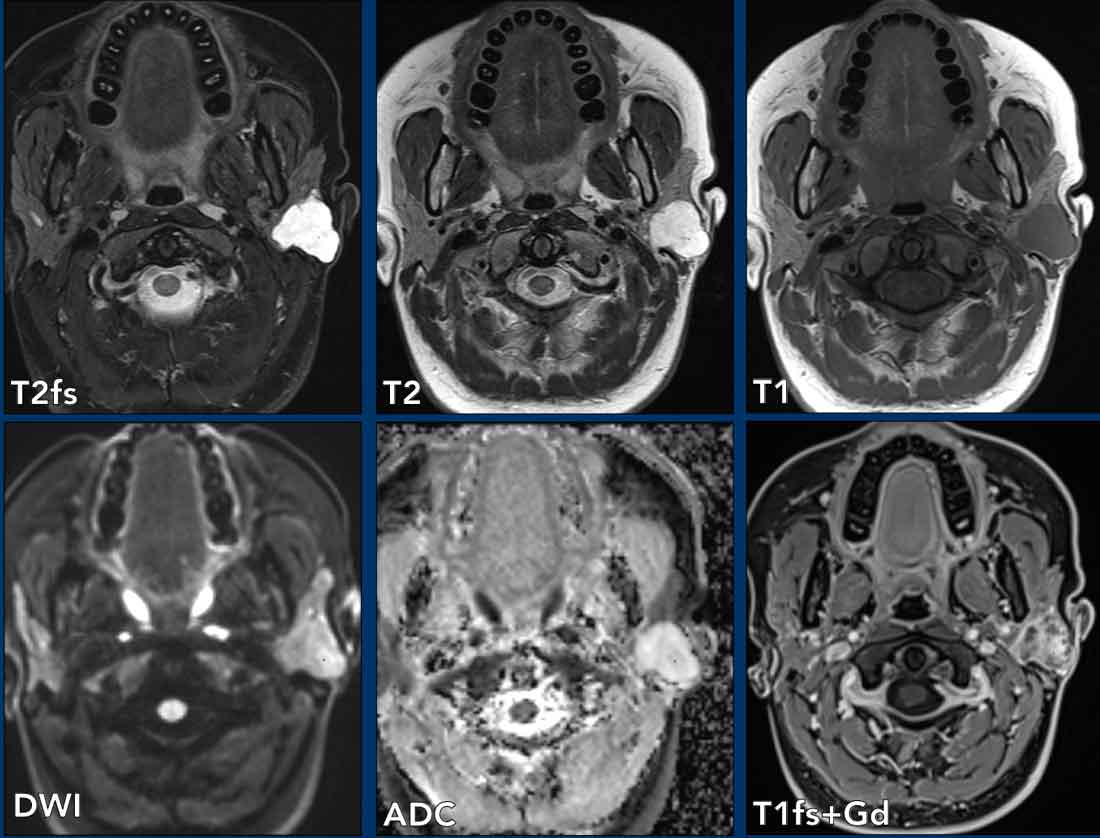
Pleomorphic adenoma.
Case
A 24-year-old female noticed a left postauricular swelling approximately 3 years ago. Recently the lesion has grown and become tender.
Imaging
- Location: lesion within the superficial lobe of the parotid gland, making it a parotid space lesion.
- Normal contents: Fat, lymph nodes, salivary gland tissue, neurovascular bundle
- MRI Findings: Well-defined, lobulated, homogeneous mass with a capsule. Hyperintense ("light bulb bright") on T2-weighted imaging—a classic feature. Typically located in the superficial lobe of the parotid gland.
Differential Diagnosis
- Pleomorphic adenoma: most likely diagnosis
- Warthin tumor: More common in smokers, bilateral, older men; less T2 hyperintense.
- Mucoepidermoid carcinoma: Usually has irregular borders, infiltrative appearance, and mixed solid-cystic components.
Fine-needle aspiration: Cytological findings consistent with a pleomorphic adenoma.
Pathology: Parotidectomy confirmed pleomorphic adenoma.
Key Points:
- Most common benign salivary gland tumor (~60% of cases) characterized by slow growth and a mix of epithelial and stromal components (hence pleomorphic).
- Benign but carries a risk of malignant transformation.
- Recurrence risk if incompletely resected.
- US Findings: Well-defined, hypoechoic mass with lobulated margins and a heterogeneous echotexture.
May show internal vascularity on Doppler. - MRI Findings: Typically hypo- to isointense on T1 and bright on T2-weighted images with heterogeneous enhancement
Well-circumscribed with a lobulated appearance.
May demonstrate a capsule.
 Carcinoma ex pleomorphic adenoma
Carcinoma ex pleomorphic adenoma
Carcinoma Ex Pleomorphic Adenoma
Pleomorphic adenomas may undergo malignant transformation, though this is relatively rare. The resulting malignancy is termed carcinoma ex pleomorphic adenoma (CXPA), an aggressive tumor associated with a poorer prognosis and requiring complete surgical excision.
Risk Factors:
- Long-standing tumors (especially those present for >10 years)
- Incomplete excision or recurrent tumors
- Radiation exposure (historical risk factor)
Key Points:
- Incidence: ~5–10% of long-standing pleomorphic adenomas
- Red Flags: Rapid growth, pain, facial nerve palsy, or fixation to surrounding tissues
Case
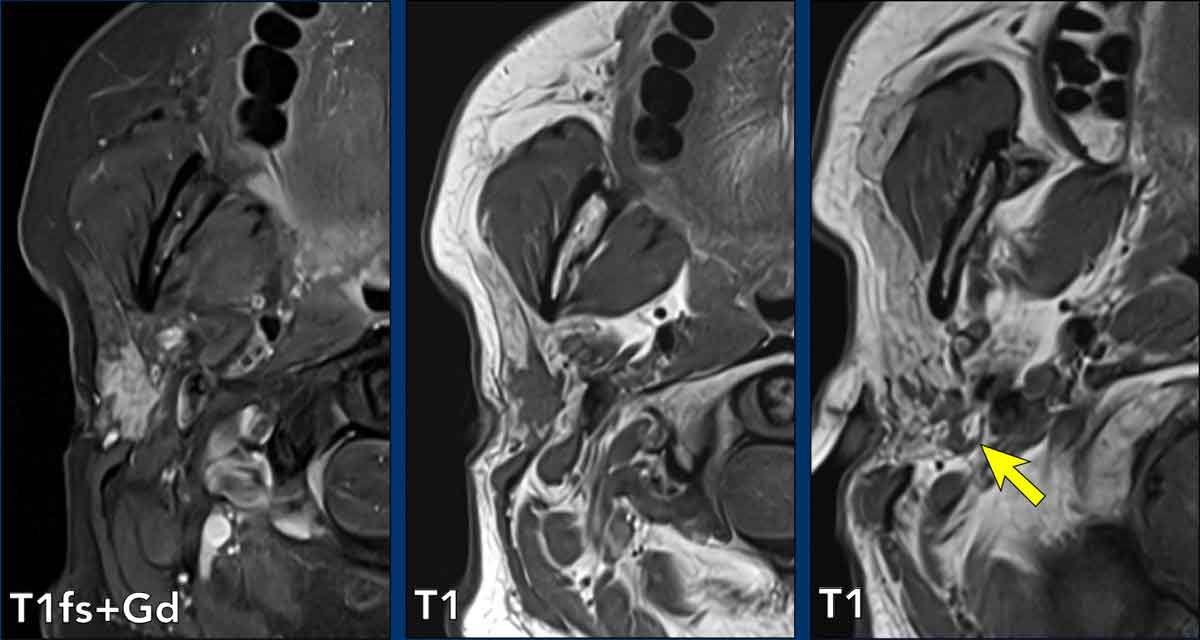
73-year-old male presents with a long standing swelling in the right neck that progresses the last coups of weeks. Now also reduced flexibility of the left side of the face with problems closing mouth and left eye.
Imaging
- Location: Lobulated lesion at the junction of the deep and superficial lobes of the left parotid gland, with anteromedial displacement of the carotid space and widening of the stylomandibular foramen, consistent with a parotid space lesion.
- Normal Contents: Fat, lymph nodes, salivary gland tissue, and the neurovascular bundle.
- MRI Findings: The lesion exhibits hypo- to isointense signal on T1-weighted imaging and hyperintense signal on T2-weighted imaging, with heterogeneous enhancement—features typical of pleomorphic adenoma. However, several regions demonstrate moderate diffusion restriction, corresponding to relatively lower T2 signal intensity. These findings may suggest more aggressive or potentially malignant characteristics. Additionally, there is suspicion of perineural spread along the facial nerve, extending from the lesion to the stylomastoid foramen and into the mastoid segment. This should be considered malignant until proven otherwise (as indicated by the arrow on the sagittal image).
Pathology: Carcinoma ex pleiomorphic
Warthin Tumor
Case presentation
A 73-year-old female with a known history of supraglottic laryngeal carcinoma presented with an incidental finding on PET/CT.
Imaging Findings
- Location: Lesion in the superficial lobe of the left parotid gland (parotid space lesion).
- Normal Contents: Fat, lymph nodes, salivary gland tissue, neurovascular bundle.
- CT Findings: Multicystic lesion in the parotid gland (yellow arrow), with a solid mural nodule demonstrating FDG avidity (white arrow).
Ultrasound Findings: Well-defined hypoechoic lesion with internal septations, posterior acoustic enhancement, and vascularity in the wall.
Differential Diagnosis
- Warthin tumor
- Lymph node metastasis
- Pleomorphic adenoma
Fine-Needle Aspiration (FNA) Cytology : Primary salivary gland tumor, most consistent with Warthin tumor.
Key Points: Warthin Tumor
- Benign salivary gland tumor, typically arising in the parotid gland.
- Often bilateral or multifocal; strongly associated with smoking.
- Malignant Potential: None.
- PET-CT: Usually FDG avid; frequently bilateral or multifocal; often incidental.
- Ultrasound: well-defined, hypoechoic or heterogeneous mass with cystic components and internal septations, may have posterior acoustic enhancement and show vascularity on Doppler (may mimic lymph nodes). 30% show cystic component
- MRI: Hypo- to isointense on T1W and hyperintense on T2-weighted (especially cystic areas). There is heterogeneous enhancement. Multilobulated or bilateral presentation is common.
Malignant Parotid Salivary Gland Tumor
Case presentation
A 54-year-old female presented with a 1-year history of swelling at the right mandibular angle.
Imaging
- Location: lesion in the superficial lobe of the right parotid gland, making it a parotid space lesion.
- Normal contents: Fat, lymph nodes, salivary gland tissue, neurovascular bundle
- Findings: ultrasound shows a hypoechoic mass with irregular borders in the superficial lobe of the right parotid gland.
Ultrasound-guided fine-needle aspiration cytology (US-FNAC) was performed and a MRI for further evaluation.
Continue with the next images...
MRI findings
- Axial T1 with fatsat shows a spiculated enhancing tumor in the superficial part of the right parotid gland.
- The tumor extends posteriorly in the direction of the stylomastoid foramen, i.e. the main facial trunk (arrow).
Continue with additional MR images...
MRI findings
- Pathological enhancement of the mastoid portion of the facial nerve indicative of perineural extension (yellow arrows).
- Compare to normal left side.
Surgery
Right superficial parotidectomy was performed
Pathology
Adenoid cystic carcinoma (ACC) with extensive perineural spread.
Note
When dealing with a parotid tumor with malignant imaging feature, perineural spread should be actively searched for.
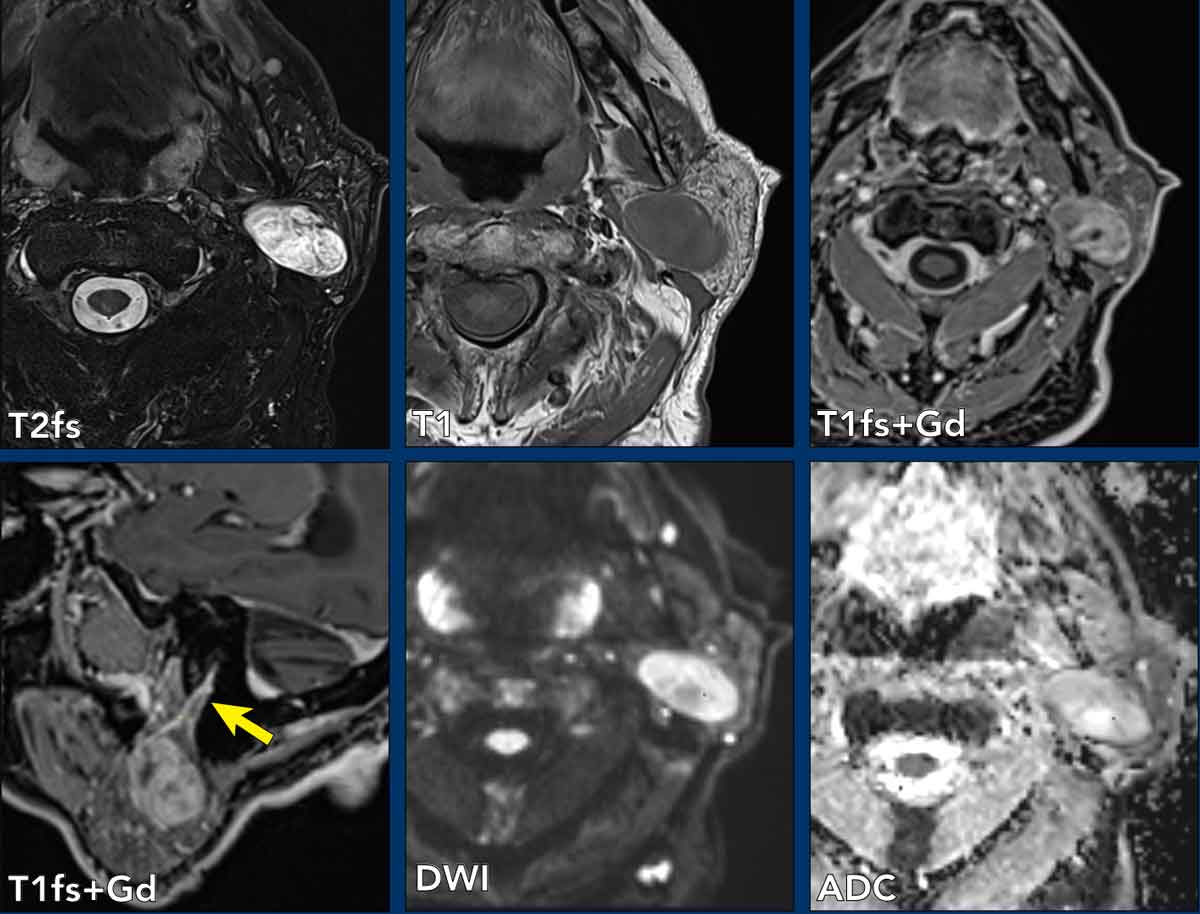
Peripheral nerve sheath tumor (PNST)
Case presentation
A 56-year-old male presented with a 2-month history of swelling at the left mandibular angle.
Imaging
- Location: lesion in the superficial and deep lobe of the left parotid gland, making it a parotid space lesion.
- Normal contents: Fat, lymph nodes, salivary gland tissue, neurovascular bundle
- Findings
- Ultrasound: multilocular hypo-echoic lesion in the superficial and deep lobe of the left parotid gland. Suspicion of intraparotid lymphadenopathy.
Diagnostic Workup
- US-guided FNA: inconclusive.
- US-guided core needle biopsy—painful, with radiating facial pain during the procedure (PA diagnosis: PNST)
Continue with the MRI, which was performed after the PNST diagnosis...
MRI findings
- Axial T1W image shows a lesion at the stylomastoid foramen.
- Axial STIR-images: the lesion can be followed in the parotid gland - in the expected position of the facial nerve.
- DWI shows no diffusion restriction.
- Coronal T2W-image shows a lobulated elongated intraparotid mass.
Differential diagnosis
- Peripheral nerve sheath tumor with typical fusiform shape is the most likely diagnosis based on the MR findings.
- Lymph node: unlikely, is more oval and has central vascularisation.
- Pleomorphic adenoma: not located along the nerve.
- Warthin tumor (cystic, lower T2).
Key points
- PNST can cause gradual painless facial weakness.
- A benign peripheral nerve sheath tumor (PNST) involving the facial nerve is typically a schwannoma or, less commonly, a neurofibroma or malignant peripheral nerve sheath tumor (MPNST).
- Ultrasound: Well-defined, hypoechoic fusiform mass along the nerve course without infiltration and variable vascularity on Doppler.
- MRI: Hypo- to isointense on T1W and hyperintense on T2W images with heterogeneous or homogeneous enhancement.
Nerve continuity may be visible, confirming origin.
"Split-fat sign" (thin rim of fat around the lesion).
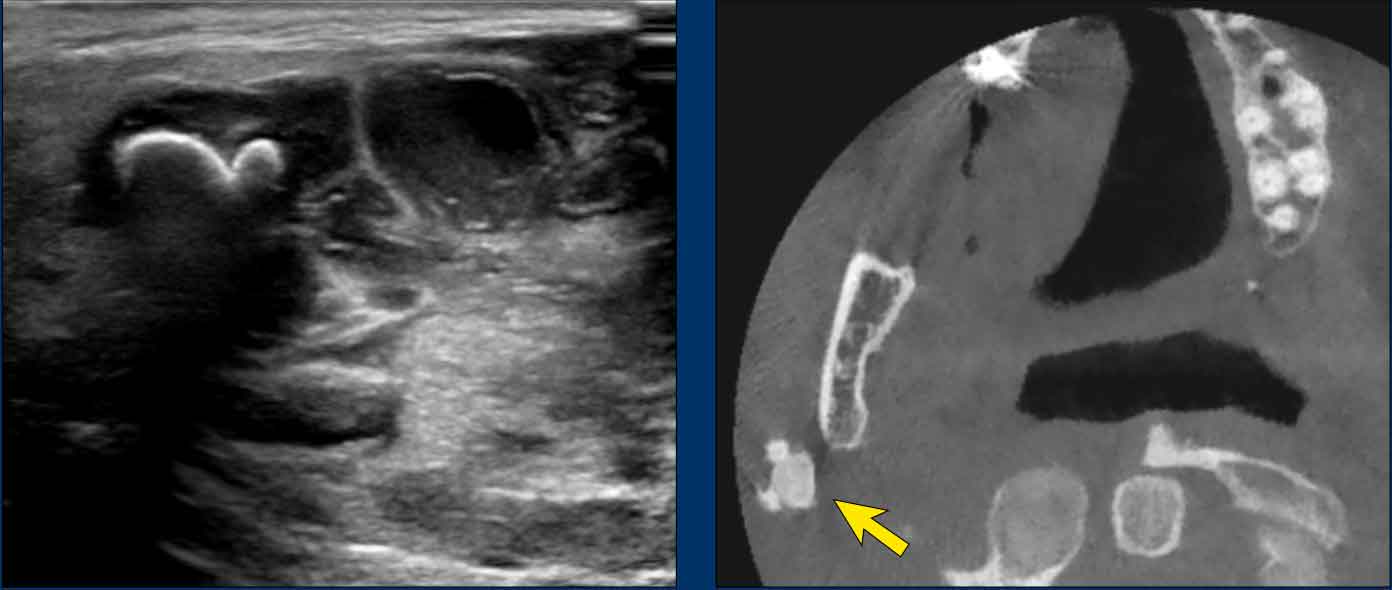
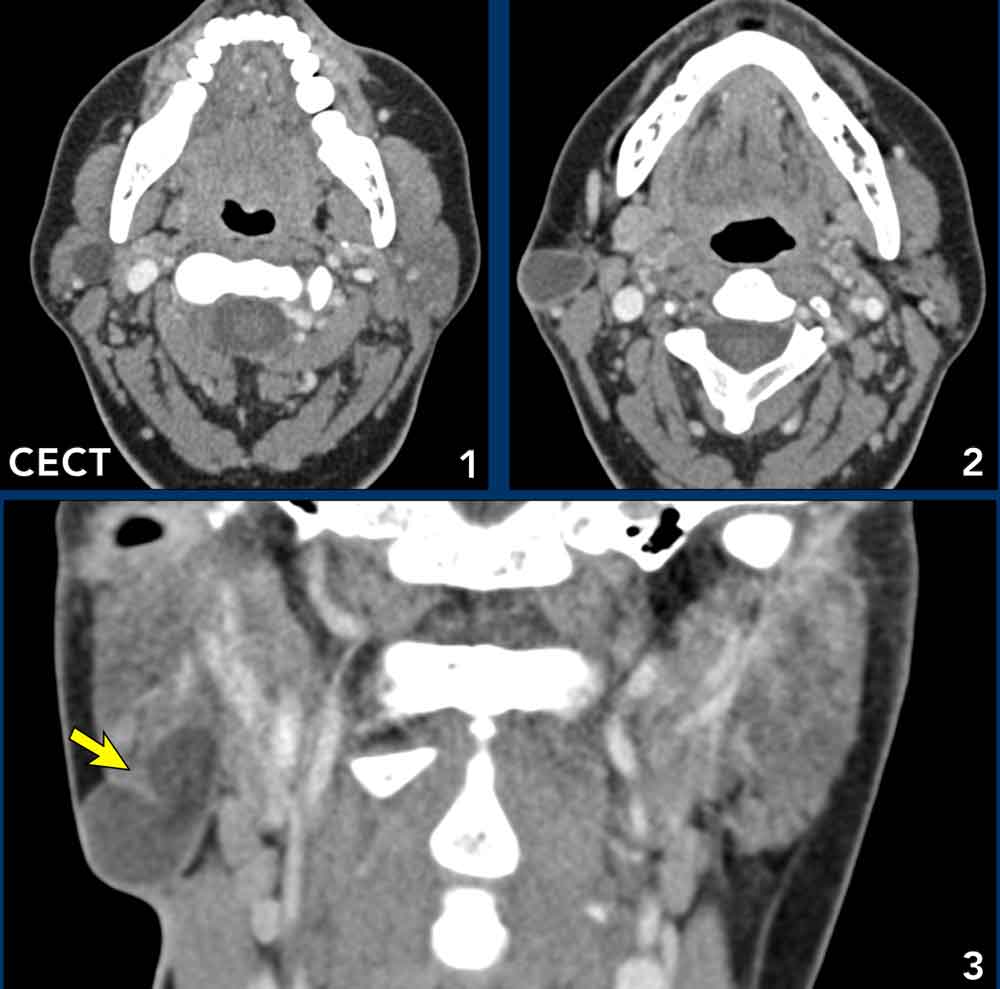
Sialolithiasis
Case presentation
A 38-year-old female presented with a painful swelling at the right mandibular angle.
Imaging
- Location: lesion in the superficial lobe of the right parotid gland, making it a parotid space lesion.
- Normal contents: Fat, lymph nodes, salivary gland tissue, neurovascular bundle
- Findings
- Ultrasound: shows multiple stones in the parotid gland with acoustic shadowing, located in and around fluid containing spaces (probably abscesses).
- CT shows three calcifications at the mandibular angle (arrow).
Continue with the MR...
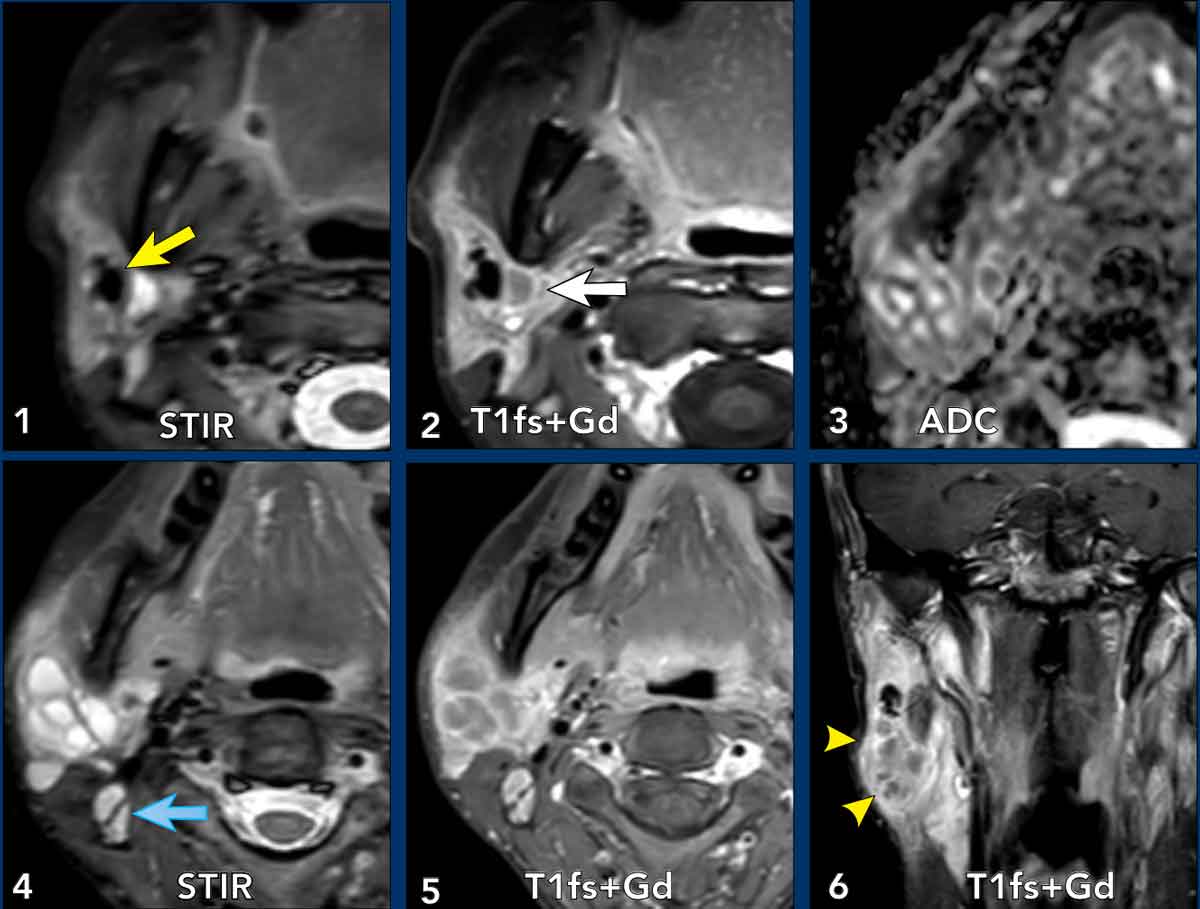 Click on image for an enlarged view
Click on image for an enlarged view
MRI findings confirm the diagnosis of sialadenitis with sialoliths and abscesses
- Axial STIR shows areas of signal void compatible with salivary stones.
- T1fs+Gd shows stones and fluid collectionswith rim enhancement compatible with abscess formation.
- ADC map shows multilocular intraparotid lesions with restriction in the rim (corresponding tot the enhancement in 2 and 5).
- Axial STIR: fluid collections and enlarged retroparotid lymph node (blue arrow)
- T1fs+Gd image: multiple fluid containing locules with rim enhancement and enlarged retroparotid lymph node .
- Coronal T1fs+Gd image: full view of the multilocular parotid abscesses and intraparotid stones.
Operative Findings and Follow-Up:
- Procedure: Drainage of multiple abscess pockets; removal of a 1.5 cm sialolith and several subcentimetric salivary stones.
- Follow-Up (1 month): Resolved swelling and pain; asymptomatic.
Key points Sialolithiasis
- Stones most commonly form in Stensen’s duct or within the gland itself and can range from less than 1 mm to several centimeters.
- Stones can cause pain and swelling and may lead to inflammation with abscess formation.
- Ultrasound is very effective for detecting stones.
- CT Scan provides detailed images, especially for deeper or smaller stones.
- Obstruction of Stensen’s duct by a sialolith can cause obstructive sialadenitis, which can be complicated by abscesses. In a chronic fase atrophy of the gland and fatty replacement of the gland can be seen.
Lipoma
Case Presentation
A 59-year-old female presented with a two-month history of a nagging sensation in the right ear and swelling anterior to the right ear.
Imaging Findings
- Location: Lesion in the deep lobe of the right parotid gland, with medial displacement of the parapharyngeal fat and carotid space vascular structures, as well as anteromedial displacement of the pterygoid muscles (i.e. parotid space lesion).
- Normal Contents: Fat, lymph nodes, salivary gland tissue, neurovascular bundle.
- MRI Findings:
- Well-defined, lobulated lesion with homogeneous content in the deep lobe of the parotid gland.
- Signal intensity follows fat:
- T1 hyperintense
- Signal suppression on T2 fat-saturated sequence
- Low signal on DWI
- The lesion splays the masseter muscle rather than infiltrating it (yellow arrow).
Differential Diagnosis
- Lipoma: Most probable, given the well-defined, homogeneous lesion with fat signal characteristics.
- Liposarcoma: Typically demonstrates infiltrative margins, heterogeneity, calcifications, necrosis, or vascularity.
Key Notes
- The primary role of imaging is to:
- Confirm benign fatty composition
- Define lesion extent
- Exclude liposarcoma or other mixed lesions
- Parotid space lipomas are rare, usually located superficial or deep to the parotid gland, and uncommonly intraglandular.
- Most lipomas are solitary and sporadic.
Parotid lymph nodes
Case Presentation
An 86-year-old male with a history of chronic lymphocytic leukemia (CLL) presented with bilateral neck swelling.
Imaging Findings
- Location: Multiple oval lesions in both parotid glands.
- Normal Contents: Fat, lymph nodes, salivary gland tissue, neurovascular bundle.
- MRI Findings:
- Axial T1: Multiple solid intra- and periparotid round to oval lesions with iso-intense T1 signal in both parotid glands.
- Coronal T1 (fat-saturated + Gadolinium): Additional multiple non-necrotic lymph nodes bilaterally in the neck.
Differential Diagnosis
- Normal lymph nodes: Typically few, bilateral, oval nodules with homogeneous intermediate T1 signal.
- Parotid lymphoma: Often presents as bilateral, multiple oval nodules with homogeneous intermediate T1 signal.
- Lymph node metastases: More commonly unilateral, with infiltrative margins and central necrosis in some cases.
Note:
Differentiating between normal intra-parotid lymph nodes and lymphoma nodes on MRI is challenging. The presence of associated cervical lymphadenopathy may raise suspicion for lymphoma.
Diagnostic Approach: Ultrasound-guided core needle biopsy is the preferred procedure for histopathological confirmation.
Key Notes
- The parotid space contains intraglandular and periglandular lymph nodes, which drain the scalp, forehead, eyelids, external ear, and parotid gland.
- Enlargement may be due to reactive, infectious, or neoplastic causes.
- Lymph node metastasis in this region most commonly originates from skin cancers of the face, external ear, and scalp, with squamous cell carcinoma (SCC) being the most frequent etiology.
- Lymphoma nodes typically show homogeneous enhancement, whereas central necrosis is a hallmark of SCC metastases.
Masticator space
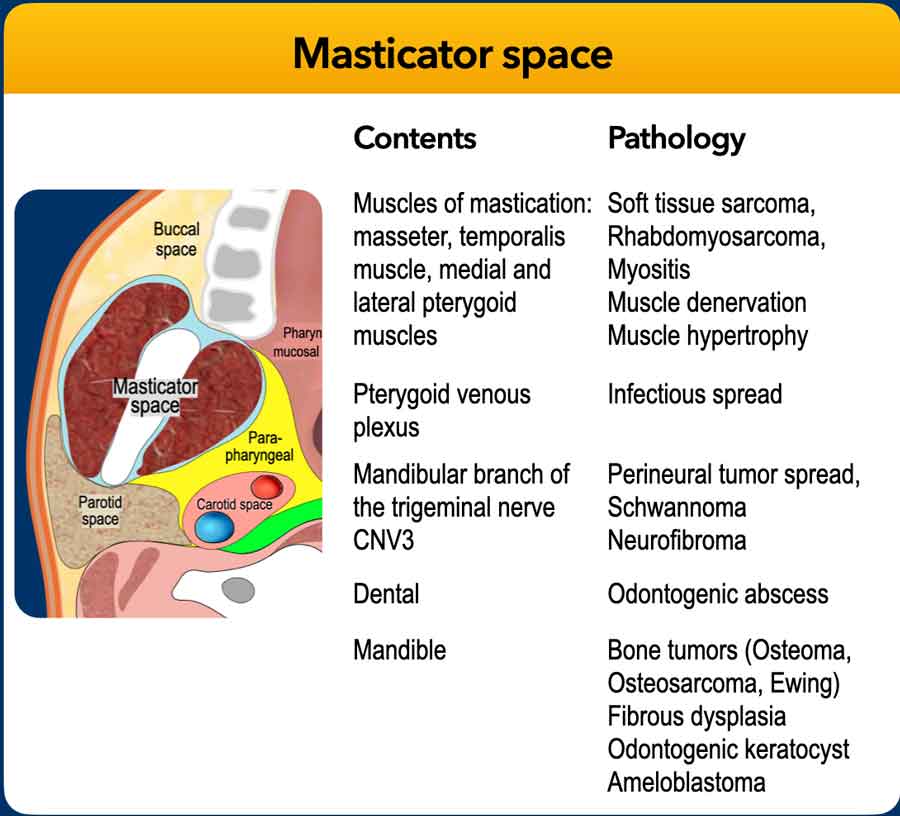
The masticator space runs from the skull base to the mandibular angle.
Head and neck malignancies frequently demonstrate a propensity for perineural tumor spread along the course of the mandibular division of the trigeminal nerve.
Consequently, it is essential to ensure that your imaging protocol encompasses the entire nerve trajectory—from the mental foramen to the trigeminal nucleus within the lateral pons.
 Click on the images to obtain an enlarged view
Click on the images to obtain an enlarged view
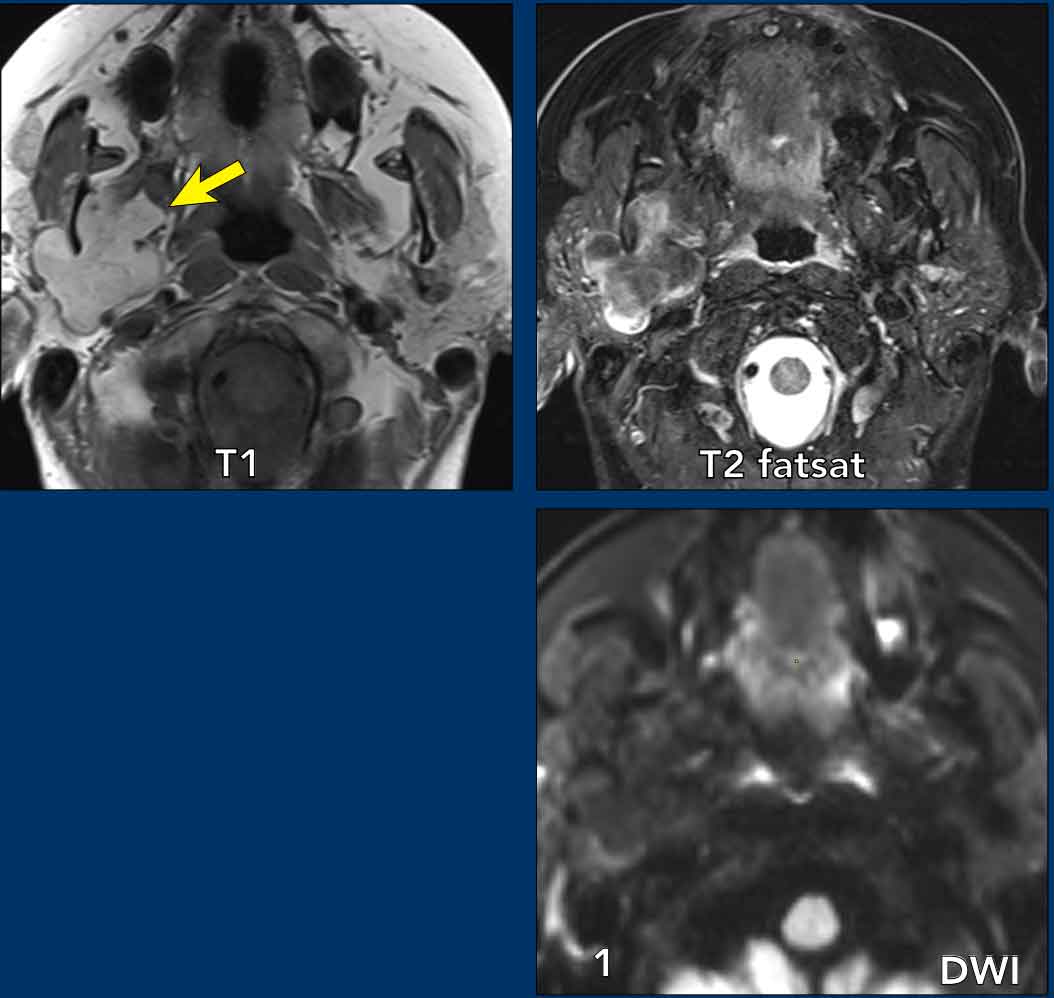
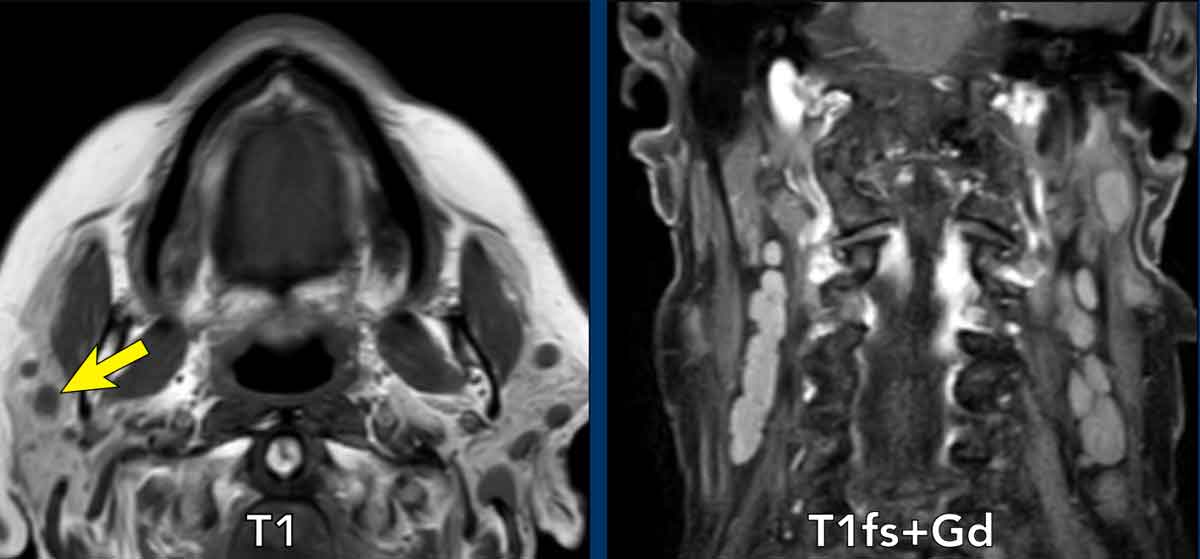
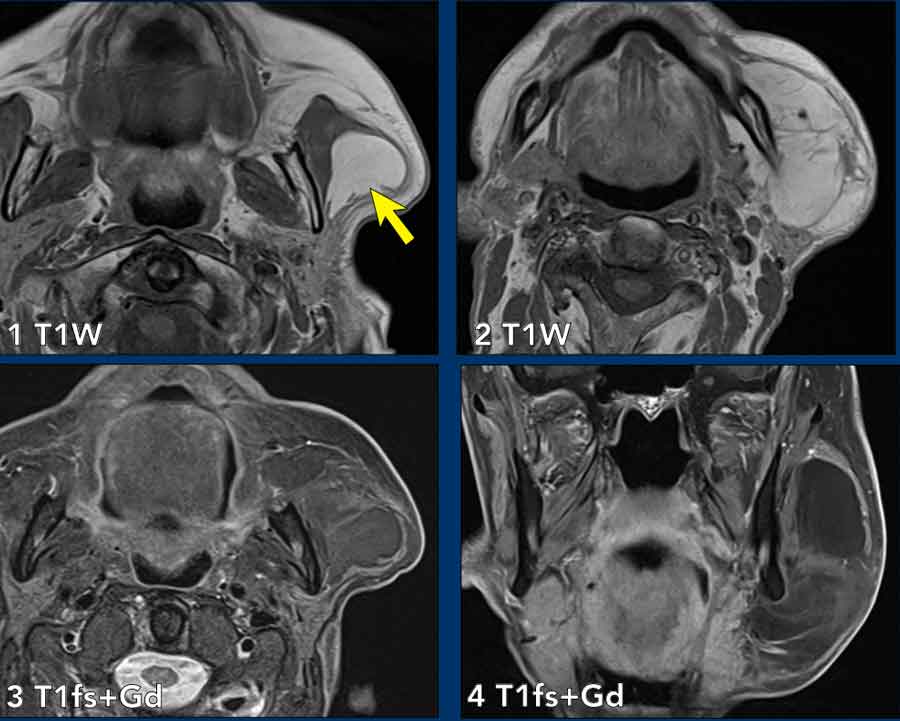
Pediatric rhabdomyosarcoma
Case Presentation
A 5-year-old boy presents with a slowly enlarging, painless swelling of the right cheek.
Imaging
- Location: The lesion is centered around the posterior body of the mandible, with posteromedial displacement of the parapharyngeal fat, consistent with a masticator space lesion.
- Normal Contents of the Masticator Space: Muscles (masseter, medial and lateral pterygoid), Venous plexus, Bone and Nerves
- MRI findings:
- Intermediate T1 signal intensity
- Hyperintense T2 signal intensity
- Contrast enhancement
- Diffusion restriction
- The lesion demonstrates remodeling of the posterior angle and condyle of the mandible, with invasion into the muscles of mastication (masseter, medial and lateral pterygoid).
Differential Diagnosis
- Rhabdomyosarcoma
- Osteosarcoma
- Lymphoma
Final Diagnosis: Biopsy-confirmed embryonal rhabdomyosarcoma
Treatment and Response
The patient was treated according to the FaR-RMS (Fusion and Risk-adapted Rhabdomyosarcoma) protocol, showing a favorable response to chemotherapy and proton beam radiation therapy.
Key Points
- Rhabdomyosarcoma accounts for up to 40% of head and neck sarcomas and is the most common childhood soft tissue sarcoma.
- Check for perineural spread.
Perineural tumorspread
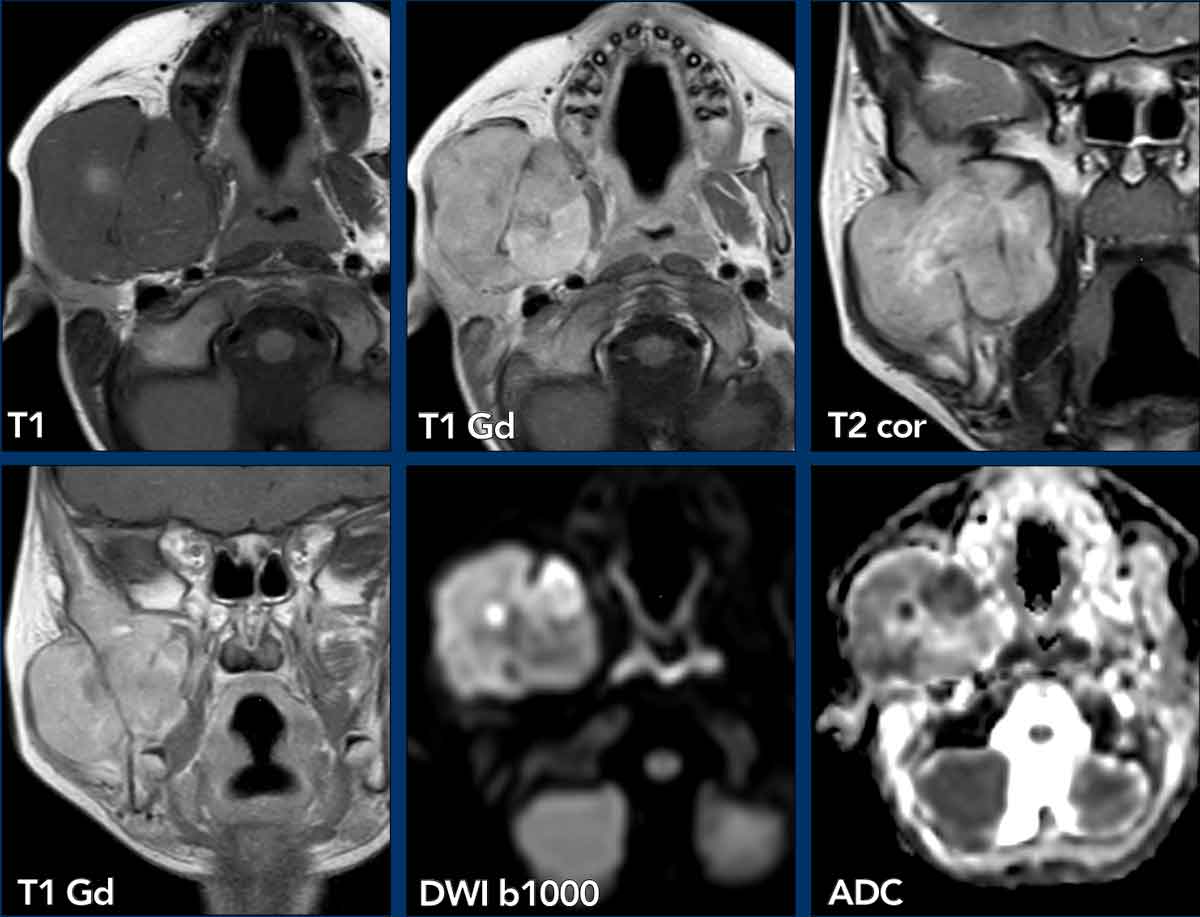
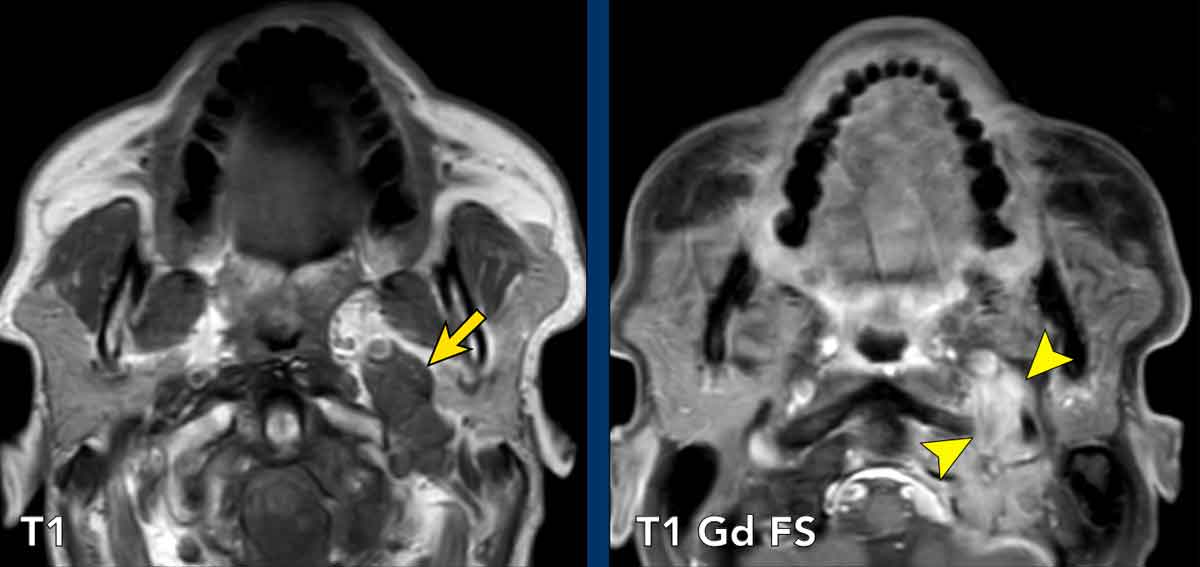
Case Presentation
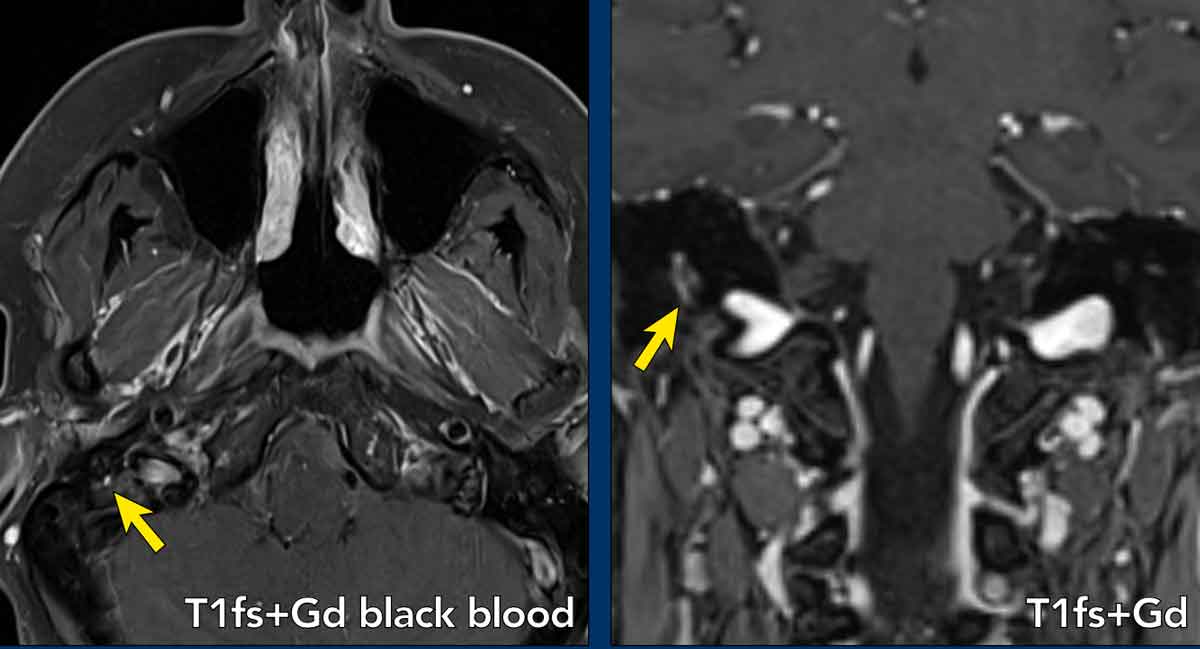
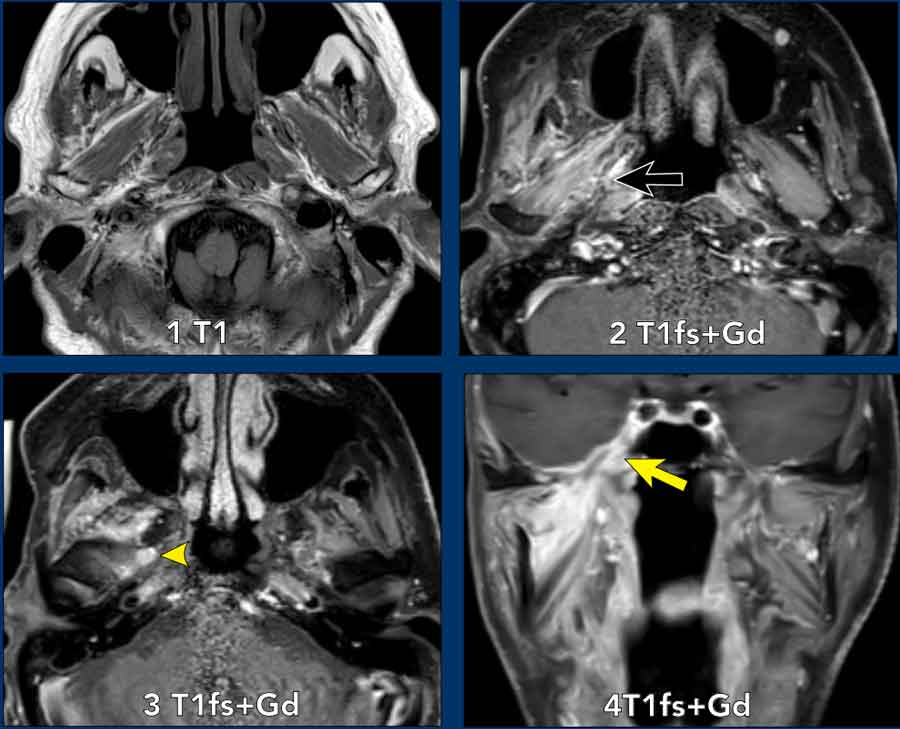
An 84-year-old male presented with a recurrent cutaneous squamous cell carcinoma of the right temporal region.
Imaging
- Location: Pathological enhancement was identified along the right medial pterygoid muscle, anterolateral to the parapharyngeal fat, consistent with a masticator space lesion.
- Normal Contents: Muscles (e.g., medial pterygoid), venous plexus, bone and nerves
- MRI Findings
- Axial T1-weighted imaging: Symmetric, normal appearance of the medial pterygoid muscle.
- T1-weighted gadolinium-enhanced fat-saturated (T1 Gd FS) imaging: Abnormal enhancement of the right medial pterygoid muscle (black arrow), indicative of acute denervation. The acute denervation was attributed to extensive perineural spread along the mandibular nerve, extending to the level of the cavernous sinus and involving Meckel’s cave (indicated by an arrowhead at the oval foramen).
- Pathologic enhancement within Meckel’s cave (yellow arrow).
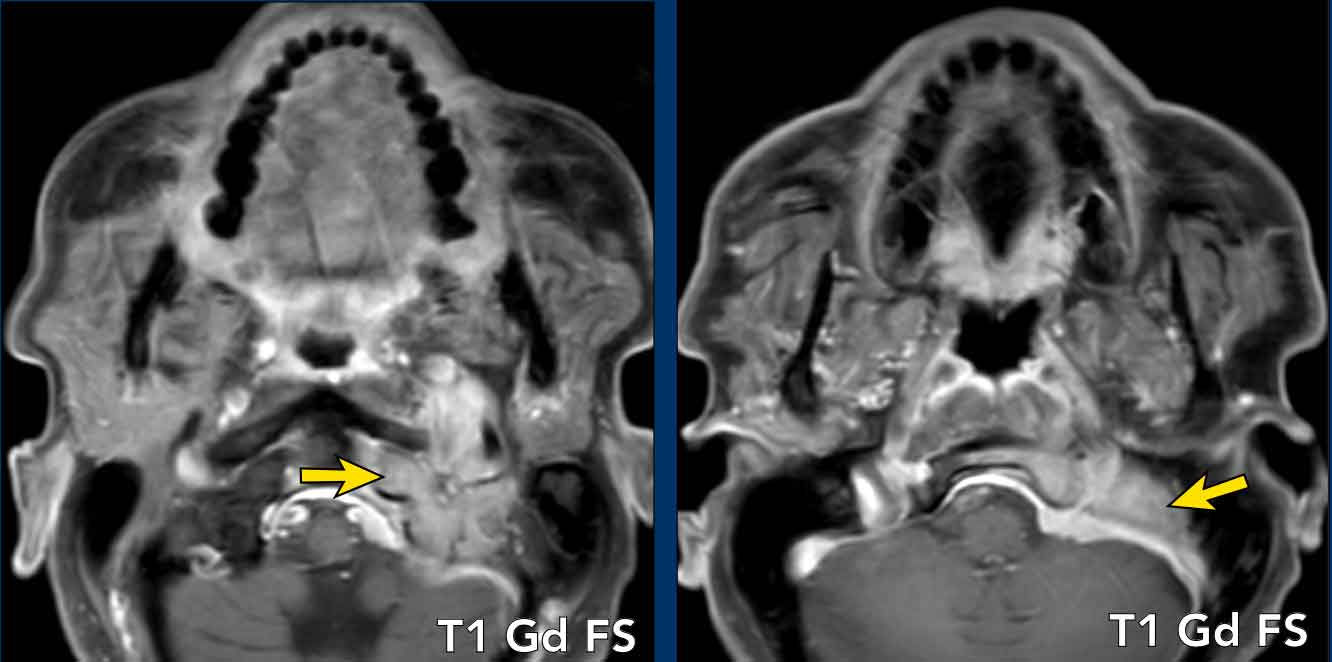
Treatment and Follow-up
The patient underwent radiotherapy targeting the areas affected by perineural spread.
A follow-up MRI study conducted four years post-radiotherapy revealed atrophy of the right medial pterygoid muscle, indicative of chronic denervation, with resolution of the previously observed abnormal enhancement.
Keypoints
- Radiological features of perineural spread to recognize:
- Nerve thickening
- Asymmetrical abnormal enhancement of the nerve
- Obliteration of the fat along the nerve (use T1)
Foraminal widening on CT - Secondary denervation of the (masticator) muscles if longstanding.Branches of the mandibular nerve (V3) of the trigeminus such as the inferior alveolar nerve are found in the masticator space. Therefore, always look along the route of V3 if a malignant lesion is found in the masticator space.
- Branches of the mandibular nerve (V3) of the trigeminus such as the inferior alveolar nerve are found in the masticator space. Therefore, always look along the route of V3 if a malignant lesion is found in the masticator space. The route is from the mandibular canal > foramen ovale > Meckels cave > sinus cavernous.
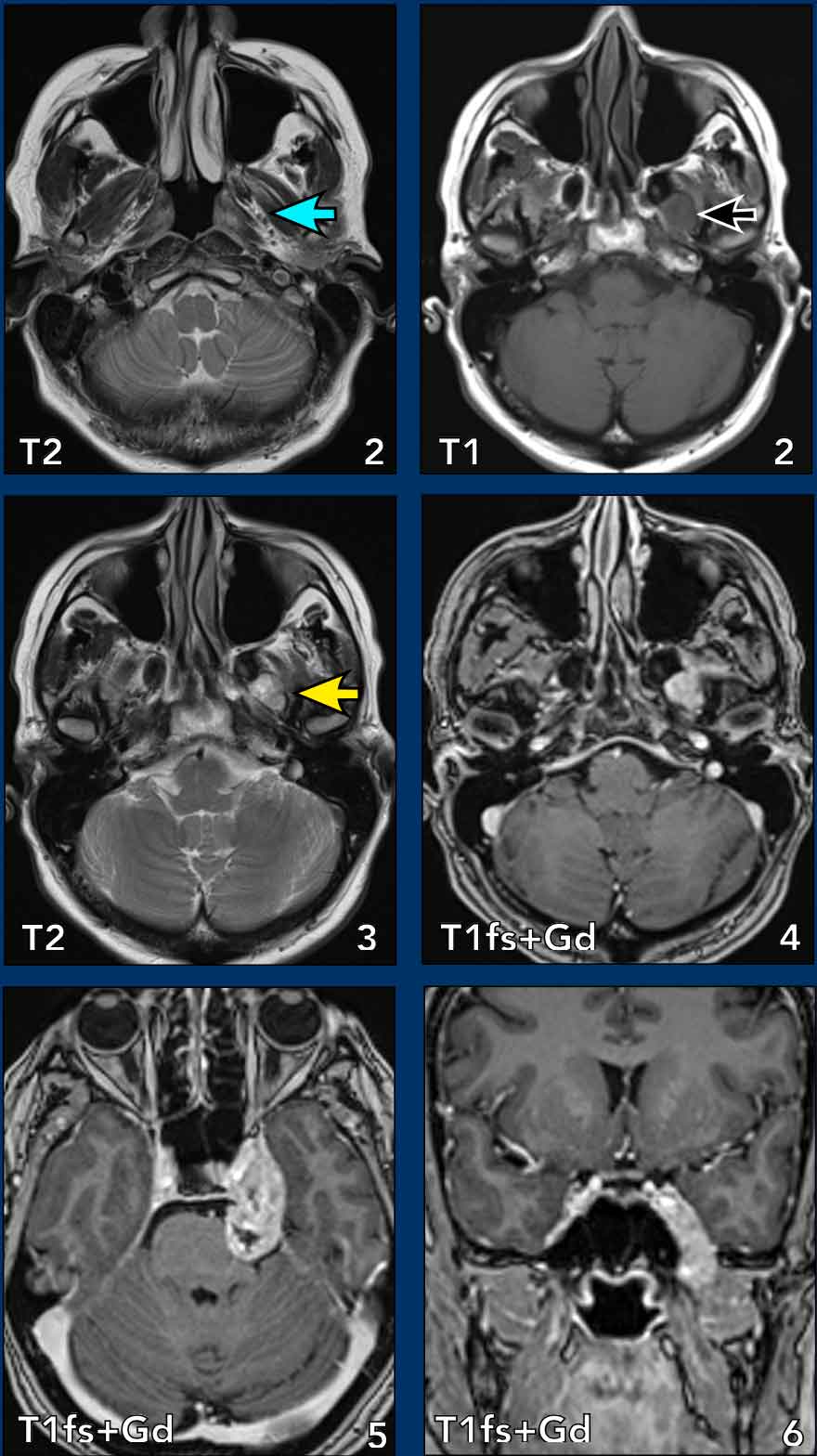
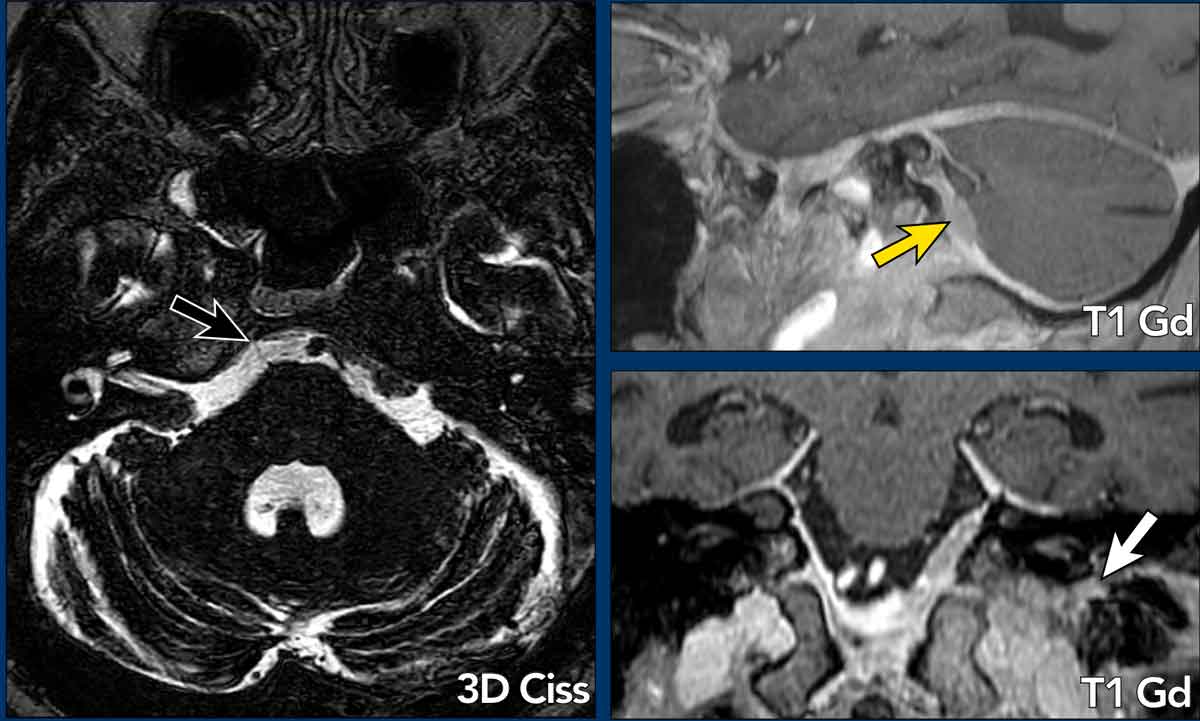
Trigeminal Schwannoma
Case Presentation
An adult patient presents with vertigo, a sensation of falling, dizziness, and vasovagal symptoms. Initially attributed to benign paroxysmal positional vertigo (BPPV), the patient later developed left facial paresthesia and headaches, with no focal neurological deficits.
Imaging
- Location: Lesion medial to the pterygoid muscle (yellow arrow), with posteromedial displacement of the parapharyngeal fat, consistent with a masticator space lesion.
- Normal Contents: Muscles, venous plexus, bone, nerves.
- MRI Findings
- Enlargement of the left mandibular nerve medial to the lateral pterygoid muscle (blue arrow).
- Images 3–5: Continuous lesion extending through an enlarged foramen ovale (yellow arrow), Meckel’s cave (enlarged), cavernous sinus (bulging), with cisternal extension and pons compression.
- Lesion Characteristics: Well-defined, fusiform, T1 isointense, T2 hyperintense, with homogeneous enhancement.
Differential diagnosis
- Schwannoma: the fusiform shape and non- invasive character makes schwannoma the most likely diagnosis.
- Neurofibroma: (usually in Neurofibromasis type 1 mutation) ; occurs rarely isolated.
- Malignant peripheral nerve sheath tumor: more invasive.
- Perineural spread: there is no primary tumor visible and usually less mass effect.
Learning Points
- Mandibular nerve (V3) course: Mandibular canal → foramen ovale → Meckel’s cave → cavernous sinus.
- Benign vs. malignant lesions: Assess margins, invasiveness, and destruction of surrounding structures.
Follow-Up
The lesion decreased in size after radiation therapy, confirmed by repeat MRI.
Lipoma
Case Presentation
An 81-year-old male presents with left-sided facial swelling.
Imaging
- Location: Well-defined lesion in the left masseter muscle (yellow arrow), consistent with a masticator space lesion.
- Normal contents: muscles, venous plexus, bone, nerves
- MRI Findings
- Axial T1-weighted imaging: Well-defined lesion in the masseter muscle with high signal intensity (arrow).
- Gadolinium-enhanced fat-suppressed imaging: Signal drop observed, with no abnormal enhancement.
Diagnosis
Lipoma
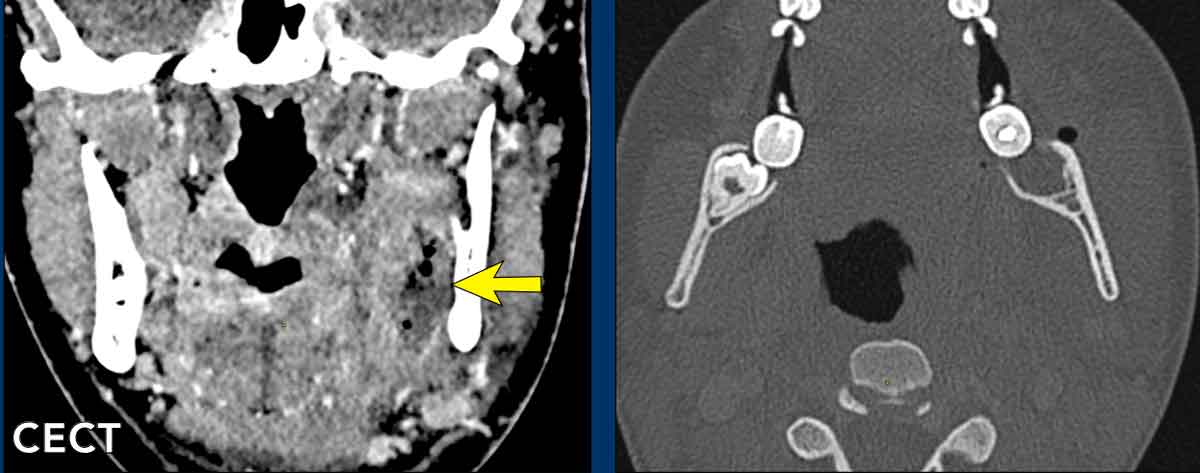
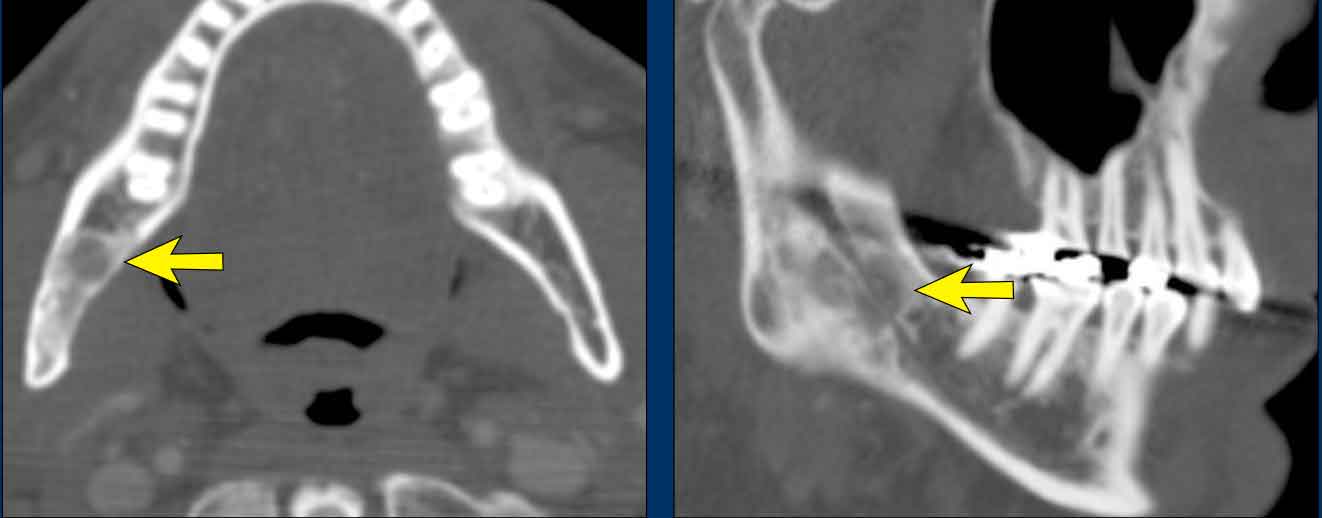
Odontogenic abscess
Case Presentation
A 27-year-old female presents three days post-extraction of tooth #38.
Imaging
- Location: Fluid collection along the lingual side of the mandibular bone in the masticator space.
- Normal Contents: Muscles, venous plexus, bone, nerves, dental elements.
- CT Findings
- Hypodense area medial to the mandible, containing air collections and minimal peripheral enhancement.
- Appearance: Typical of an abscess.
- Bone window: Extraction vacuole of the molar (tooth #38) visible.
Treatment and Follow-Up
- Surgical incision of the masticator space abscess resulted in purulent drainage.
- A drain was placed post-evacuation.
- Antibiotic therapy administered, leading to rapid clinical improvement.
Fibrous Dysplasia of the mandible
Case Presentation
A 55-year-old male with an incidental finding on neck CT.
Imaging
- Location: Lytic lesion in the right mandible within the masticator space.
- Normal Contents: Muscles, venous plexus, bone, nerves.
- CT Findings
- Partially sclerotic lesion without bone destruction in the angle of the right mandible.
- On the coronal CT image, some expansion of the marrow cavity is noted when compared to the normal left side.
- Radiology report: Suggestive of a primary bone tumor or metastasis.
Differential Diagnosis
- Fibrous Dysplasia: Ground-glass appearance, non-sharply defined, often expansile, respects cortex
- Bone Tumor/Metastasis: More sclerotic or lytic, cortical destruction
- Ossifying Fibroma: Ground-glass appearance, well-circumscribed or encapsulated
Pathological Diagnosis
Biopsy was performed under local anesthesia.
Benign bone-producing lesion, most consistent with monostotic fibrous dysplasia.
Key Points
- Fibrous dysplasia is monostotic (75%) or polyostotic (25%), often involving the skull and facial skeleton (maxilla, orbit, ethmoid, sphenoid bones).
- Ground-glass appearance on CT results from fibrous tissue + immature bone, with marrow cavity expansion but no cortical destruction.
Vascular malformation
Case Presentation
A 53-year-old female presented with an asymptomatic left cheek swelling of several years’ duration.
Imaging
- Location: Lesion in the left masseter muscle within the masticator space.
- Normal Contents: Muscles, venous plexus, bone, nerves.
- Ultrasound Findings
- Well-defined lesion within the left masseter muscle.
- Two echogenic structures with posterior acoustic shadowing, consistent with phleboliths (arrowhead).
- Ultrasound-guided aspiration: Yielded only blood.
- MR Findings
- Axial T1-weighted imaging: Swelling of the left masseter muscle with two small foci of signal void(corresponding to phleboliths).
- Axial STIR imaging: Sharply demarcated intramuscular lesion with high signal intensity and focal areas of signal void.
- Coronal Gd-enhanced fat-saturated imaging: Strong, patchy enhancement of the lesion, except in areas of signal void.
Differential Diagnosis
- Venous Malformation: Most likely: Phleboliths present, bright T2 signal, contrast enhancement; slow Doppler flow.
- Lymphatic Malformation: often more cystic components with enhancement of septa
- Venolymphatic Malformation: Phleboliths and cystic components, may show fluid-fluid levels
Conclusion
Low-flow venous malformation.
No treatment initiated due to asymptomatic presentation.
For symptomatic cases, ultrasound-guided sclerotherapy may be considered as a minimally invasive first-line treatment.
Key points
- Venous malformations are common in the head and neck, particularly in the masseter muscle, buccal space, tongue, floor of mouth, and cheek.
- Transspatial lesions are possible.
- Phleboliths are a key imaging clue for venous malformation, resulting from chronic venous thrombosis and calcification.
- Imaging limitations: Differentiating venous, lymphatic, or venolymphatic malformations is not always possible.
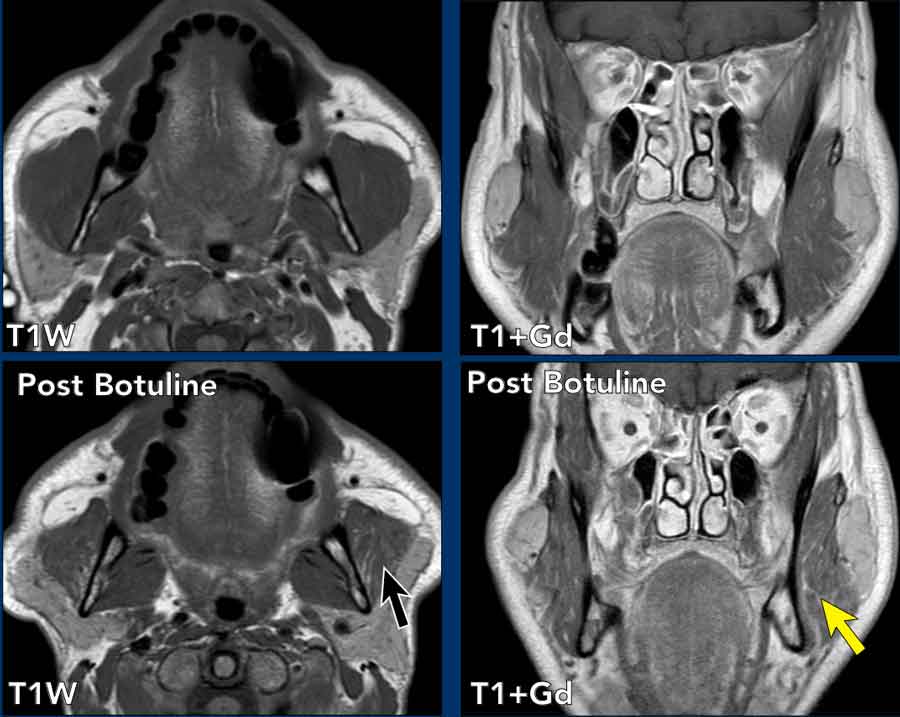
Masseter hypertrophy
Case Presentation
A 56-year-old male presents with bilateral preauricular swelling causing cosmetic concerns.
Imaging
- Location: Findings in both masseter muscles within the masticator space.
- Normal Contents: Muscles, venous plexus, bone, nerves.
- MRI Findings
- Axial and coronal T1-weighted gadolinium-enhanced (T1 Gd) images:
- Symmetric hypertrophy of the masseter muscles.
- Bilateral ventral extensions of the parotid glands contributing to the swelling.
- Follow-up imaging (6 months post-botulinum toxin injections): Marked reduction in muscle volume (black arrow). Patchy intramuscular areas of increased T1 signal intensity, consistent with fatty atrophy (yellow arrow).
Differential Diagnosis
- Masseter Muscle Inflammation: Edema, enhancement, hypervascularity
- Masseter Muscle Hypertrophy: Smooth, diffuse enlargement, normal signal intensity, no focal lesion. In rare cases, it can be unilateral and then it is important to differentiate if the asymmetry is due to hypertrophy or contralateral atrophy.
- Masseter Muscle Atrophy: Denervation-related, often unilateral.
In acute stage (<1 month): fatty replacement.
In chronic stage (>12 months): fatty replacement combined with volume loss.
Key points
- Masseter muscle hypertrophy is most often bilateral and asymmetric.
- Causes of hypertrophy:
- Bruxism (nocturnal teeth grinding)
- Excessive gum chewing
- Temporomandibular joint dysfunction
- Idiopathic masseter muscle hypertrophy
- Anabolic steroid use
Parapharyngeal space
Key Features of the Parapharyngeal Space (PPS)
- Central in the suprahyoid neck, extending from the skull base to the hyoid bone.
- Inferiorly the PPS ends at the superior margin of the submandibular gland, continuous with the sublingual spaces—facilitating disease spread.
- Styloglossus muscle separates the PPS from the carotid space.
- The direction of parapharyngeal fat displacement helps localize the primary lesion.
Function
- Facilitates smooth movement of masticator muscles during mastication and swallowing.
- Acts as a fatty "elevator shaft" for infection and tumor spread between the skull base and hyoid bone.
Lesions
- Mostly secondary, originating from adjacent spaces:
- Retropharyngeal
- Masticator
- Parotid
- Pharyngeal mucosal space
Lipoma
Case Presentation
A 69-year-old male presented with asymmetric left hearing impairment for years, along with increased ear pain during elevation changes. Otoscopy revealed bulging of the left tympanic membrane without signs of infection. The Valsalva maneuver was difficult but provided some symptomatic relief through pressure equalization.
Imaging
- Location: The lesion lies anterior to the longus colli muscles, medial to the carotid artery, with compression of the pharyngeal mucosal space. It is completely surrounded by fat, consistent with a parapharyngeal space (PPS) lesion.
- Normal Contents of PPS: Fat, minor salivary glands, vascular structures.
- MRI Findings
- Well-defined lesion with high signal on T1 and T2
- Signal drop on fat suppression images
- No enhancement or diffusion restriction
Learning Point
Primary parapharyngeal space lesions are rare. Given the limited contents of the PPS (primarily fat), the differential diagnosis is narrow:
- Benign or malignant salivary tumors (e.g., pleomorphic adenoma from ectopic minor salivary gland tissue)
- Branchial cleft cyst
- Lipoma
Minor salivary gland tumor
Case presentation
A 49-year-old female had an incidental finding on a brain MRI.
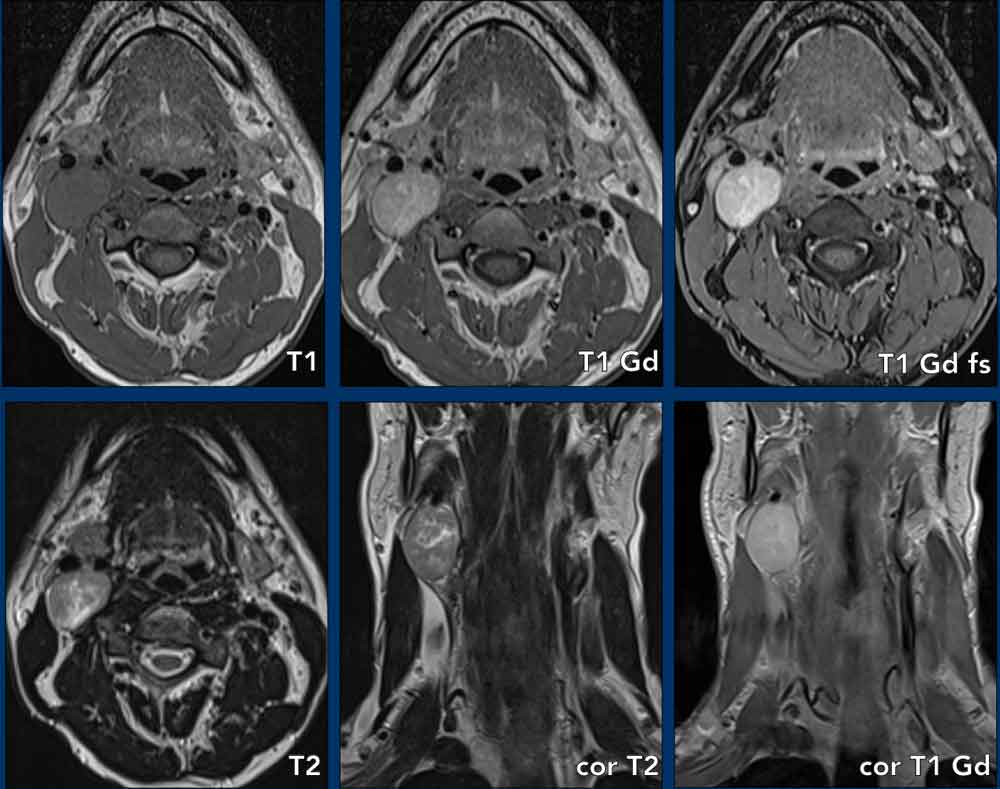
Imaging
- Location: The identification of the thin layer of fat completely encircling the lesion is the key finding indicative that the lesion is located in the PPS (arrow).
- Normal contents: fat, minor salivary glands, vascular structures
- MR Findings
- Lobulated, sharply defined, solid lesion with T1 iso-intens signal and T2 hyperintens signal, entirely surrounded by parapharyngeal fat with uniform strong enhancement, no diffusion restriction.
- The lesion shows T2 hyperintens singal and strong enhancement, making it most likely a salivary gland tumor (e.g. pleomorphic adenoma).
Since the lesion is entirely surrounded by parapharyngeal fat, it may be assumed that the lesion arises from embryonic salivary remnants in the PPS (i.e. a minor salivary gland tumor).
The patient did not want an operation and is followed up by yearly MR (wait-and-scan policy).
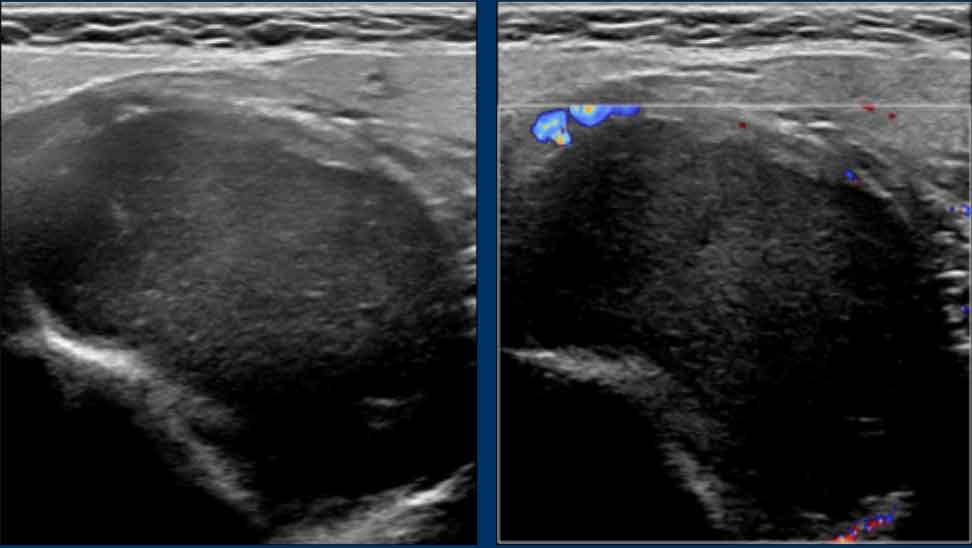
Second branchial cleft cyst
Case Presentation
A 46-year-old female presented with a swelling in the right neck and globus sensations since four weeks
Ultrasound
Thin-walled, sharply marginated, cystic mass without internal vascularization.
Continue with the MR...
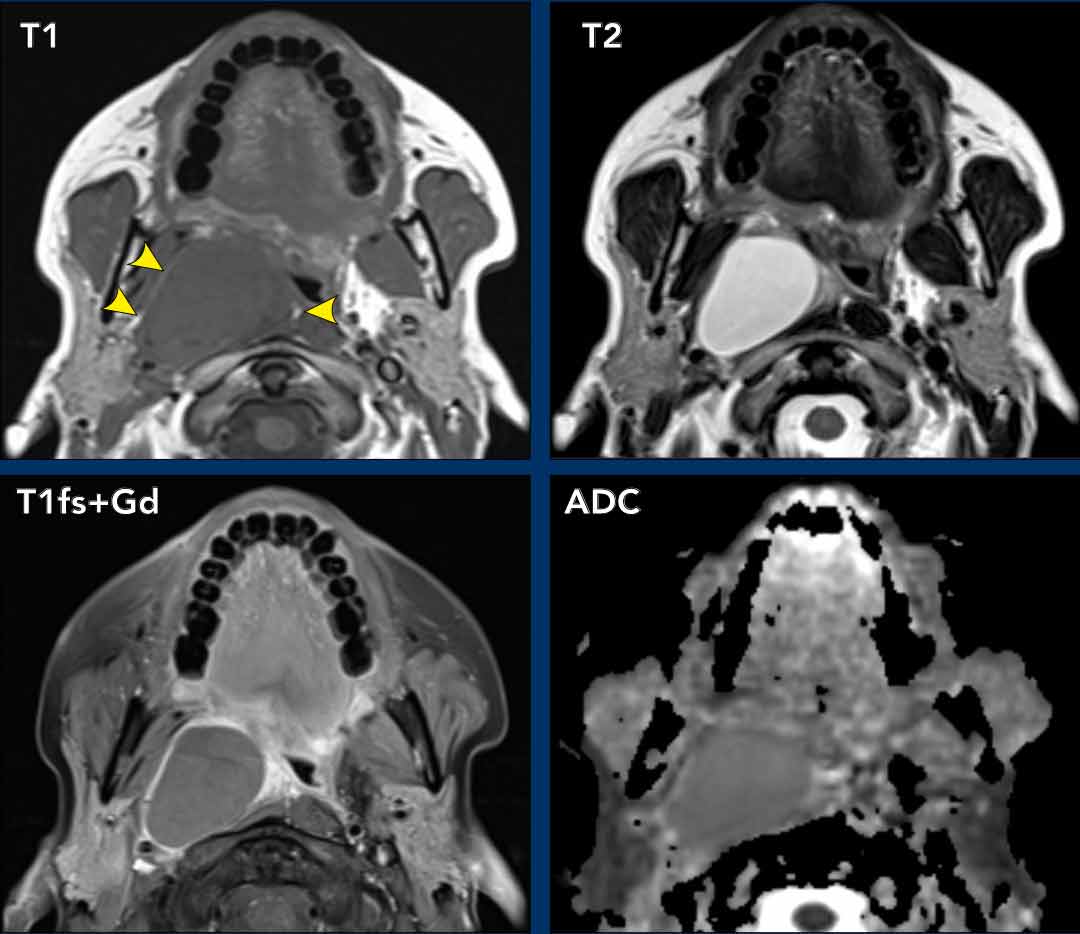
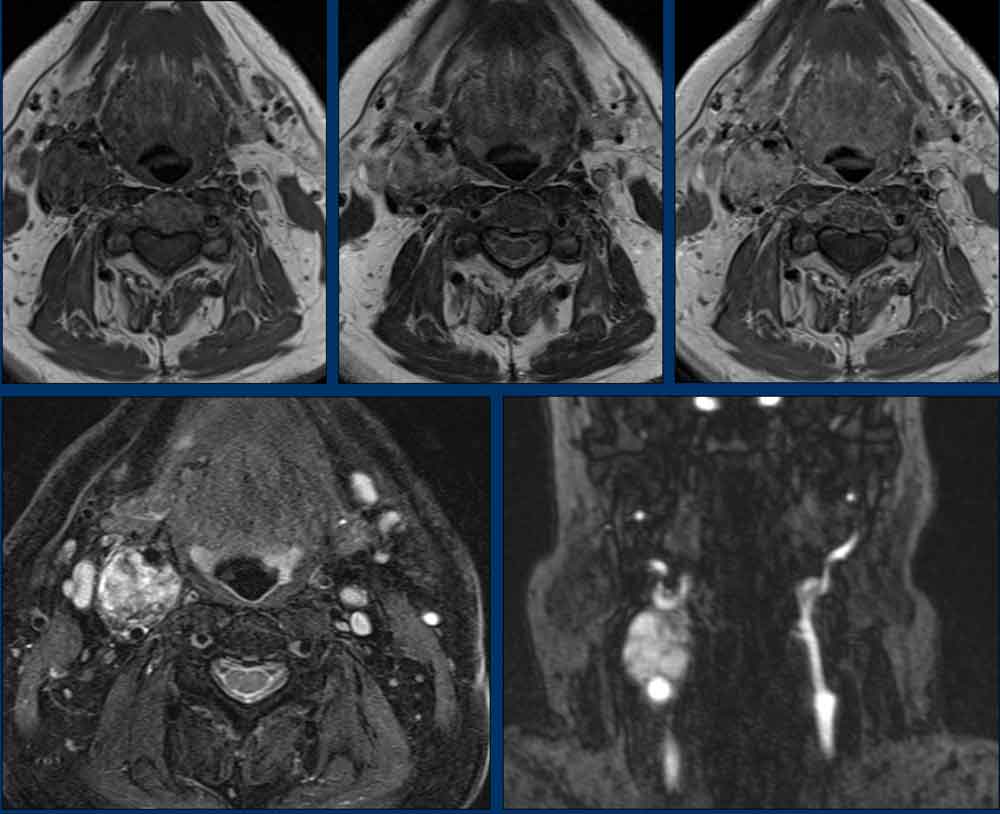
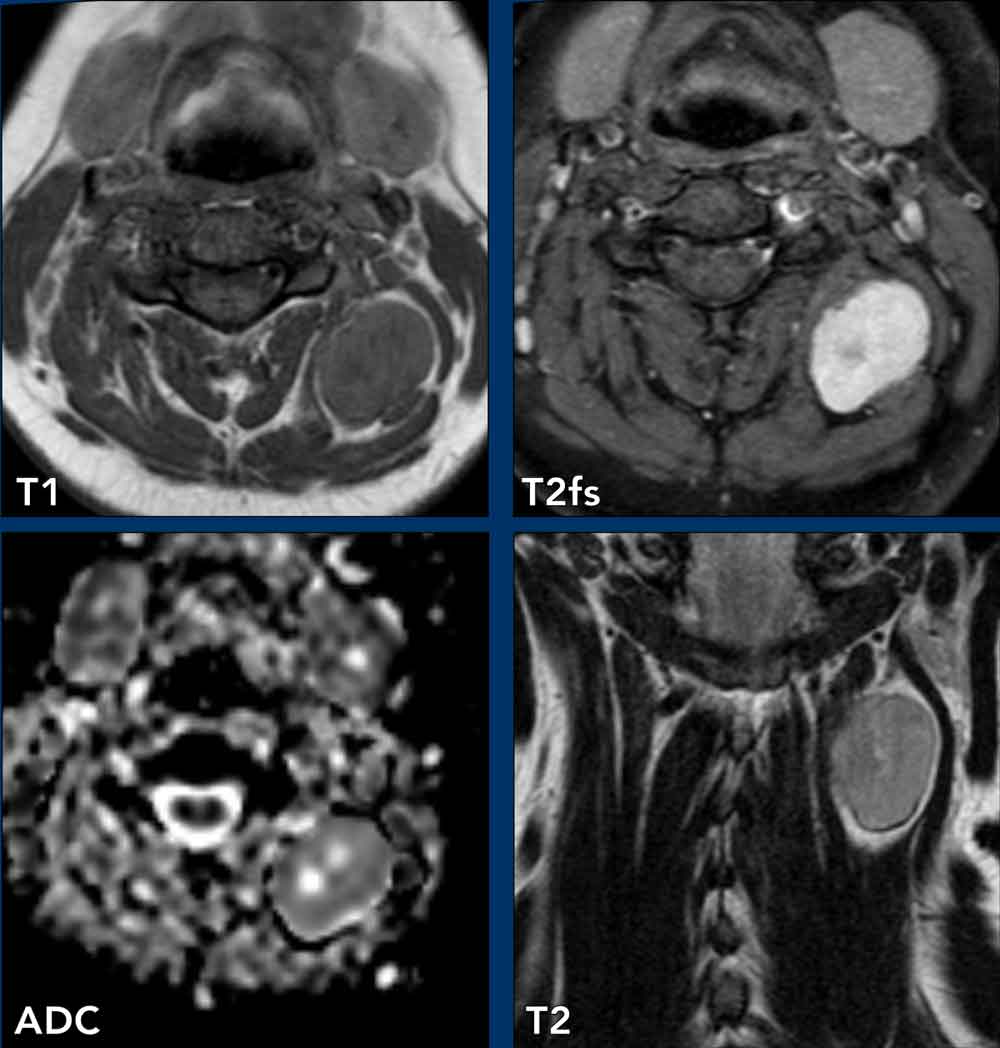
Imaging
- Location: Right-sided lesion completely surrounded by compressed fat (arrowheads), indicating a parapharyngeal space (PPS) lesion.
- Normal Contents of PPS: Fat, minor salivary glands, vascular structures.
- MRI Findings
- Axial T2: Sharply marginated cystic lesion.
- Axial Gd-enhanced fat-suppressed image: Enhancement of the thin wall of the lesion, lateral displacement of the internal carotid artery and internal jugular vein. Compression of the right longus colli muscle.
- Axial ADC map: No diffusion restriction.
Treatment and Pathology
- Surgical excision of the entire lesion was performed.
- Intraoperative finding: Possible deep connection to the pharynx, which was ligated.
- Pathological diagnosis: Benign cyst with reactive changes, compatible with a parapharyngeal second branchial cleft cyst.
Note
The parapharyngeal space (PPS) is a rare location for a branchial cleft cyst. This rare superior location to the tonsillar fossa can be explained by the fact that a second branchial cleft cyst may have an associated tract passing to the palatine tonsil. Since this tract passes through the caudal PPS, cysts in this location are usually classified as second cleft anomalies.
 Courtesy Lukas Boomgaert, UZLeuven
Courtesy Lukas Boomgaert, UZLeuven
Asymmetric pterygoid venous plexus
Case Presentation
An adult patient had an incidental finding on a brain MRI.
Imaging Findings
- Location: Masticator space, specifically anterior to the ventral margin of the lateral pterygoid muscle.
- Normal Contents: Fat, minor salivary glands, vascular structures.
- MRI Findings
- Spoiled GRE axial image: Asymmetric enhancement anterior to the ventral margin of the lateral pterygoid muscle (arrow). Normal enhancement of the pterygoid venous plexus, which can appear asymmetric and should not be mistaken for pathology.
- Spoiled GRE axial and coronal MIP images: Bilateral extension of the normal pterygoid venous plexus (arrows). More prominent on the right side in this patient.
Learning Point
The pterygoid venous plexus is a small intercommunicating cluster of venules closely related to the lateral pterygoid muscle, lying both intramuscularly and around the muscle.
It is a normal finding but may be confused with pathology, such as a venous malformation.
Carotid space
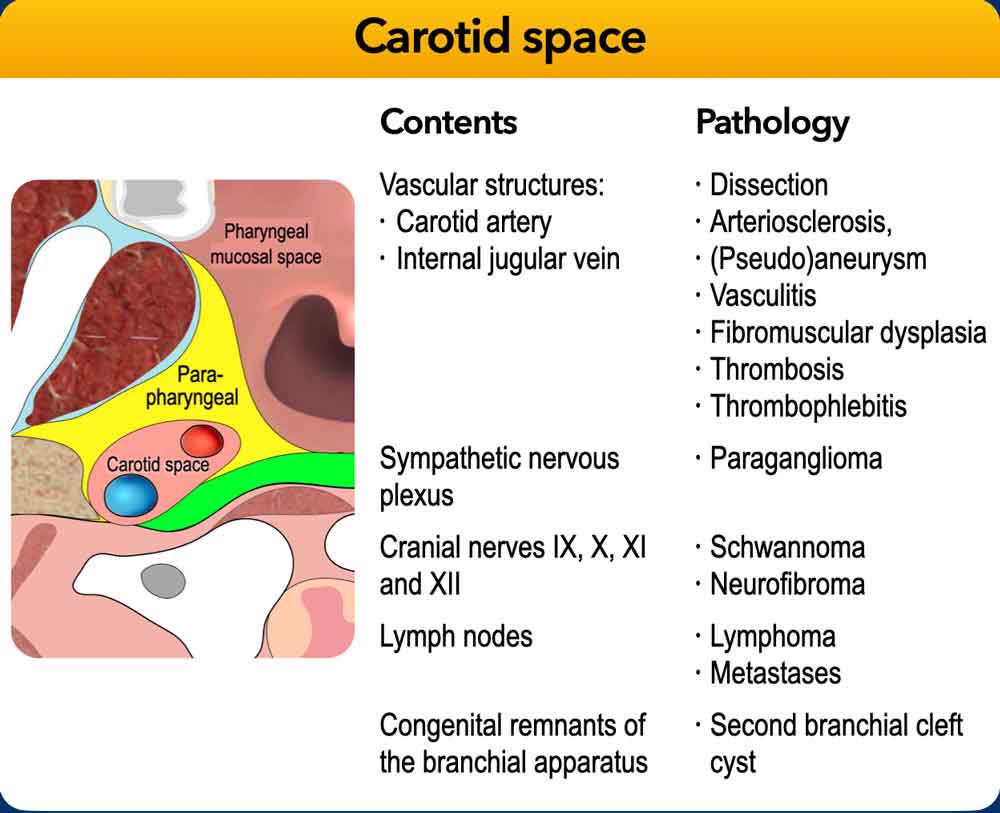
The carotid sheath (CS) is composed of all layers of the deep cervical fascia. It traverses both the suprahyoid and infrahyoid neck, extending from the jugular foramen superiorly to the aortic arch inferiorly.
Displacement patterns of CS masses:
- Nasopharyngeal level: CS masses may displace PPS fat anteriorly.
- Oropharyngeal level: CS masses may displace the posterior belly of the digastric muscle laterally and narrow the stylomandibular tunnel.
Common pathologies in the carotid space include:
- Paragangliomas (e.g., glomus vagale tumors)
- Vagal schwannomas
- Metastatic lymphadenopathy (e.g., from nasopharyngeal or oropharyngeal carcinoma)
- Internal carotid artery dissections or aneurysms
- Thrombosis or thrombophlebitis of the internal jugular vein
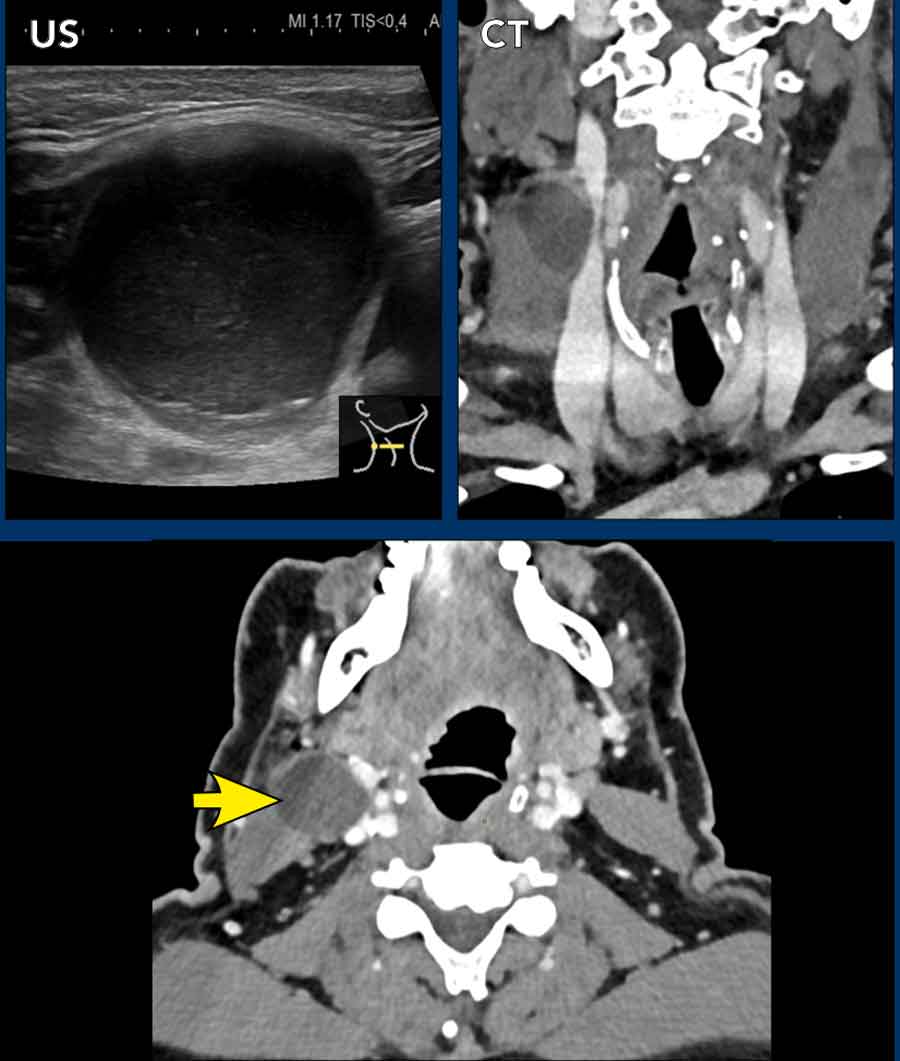
Second branchial cleft cyst
Case Presentation
A 60-year-old male presented with a swelling in the right neck at level 2.
Imaging Findings
- Location: The lesion is splaying the carotid artery and the jugular vein on the right side, making it a carotid lesion.
- Normal contents: vascular structures, nerves and sympathetic nervous plexus, lymph nodes and congenital remnants
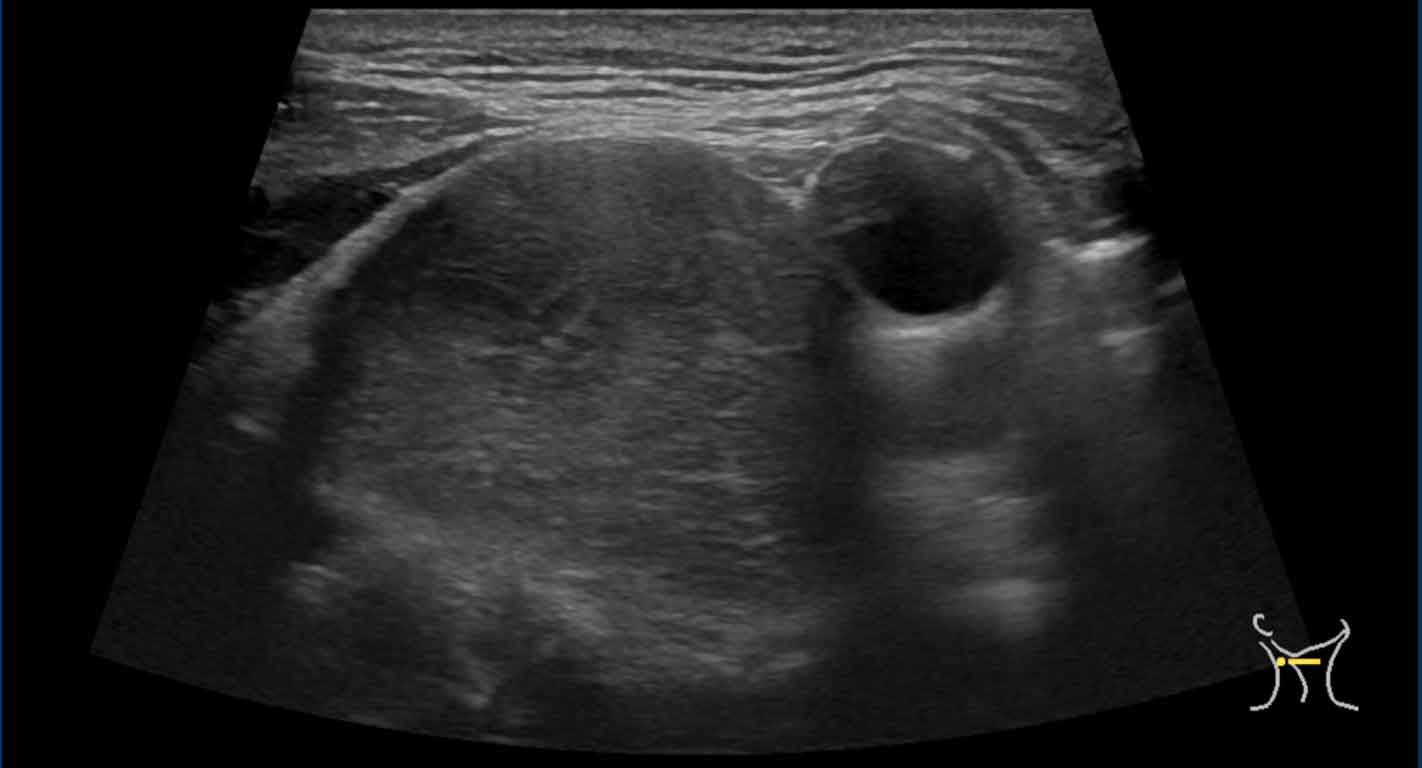
- US Findings
- Well-defined lesion with thin walls, not completely anechoic content, posterior acoustic enhancement.
- CT Findings
- Unilocular lesion with thin slightly enhancing wall and homogenous cystic content with compression of the internal jugular vein.
Differential diagnosis
- Necrotic lymph node metastasis: typically, more thick enhancing walls with heterogenous architecture and hypervascularity.
- Abscess: typically, thick enhancing walls with induration of surrounding tissue and internal gas or debris.
- Lymphatic malformation: typically multilocular, transspatial and completely anechoic.
- Second branchial cleft cyst: typical location is lateral in the carotid space and anteromedial to the sternocleidomastoid muscle. Following an infection or hemorrhage a branchial cleft cyst can may show a thick enhancing wall, heterogenous internal content, fluid-fluid levels or surrounding fat stranding.
Pathology
The lesion was resected. Findings consistent with a lateral branchial cyst. No evidence of malignancy.
Note
- Often a branchial cleft cyst is difficult to differentiate from a necrotic lymph node metastasis of squamous cell carcinoma or from papillary carcinoma of the thyroid. Therefore cytology, and if not conclusive, resection is essential for diagnosis.
- As a rule of thumb; any cystic neck lesion in an adult patient should be considered to be malignant until proven otherwise!
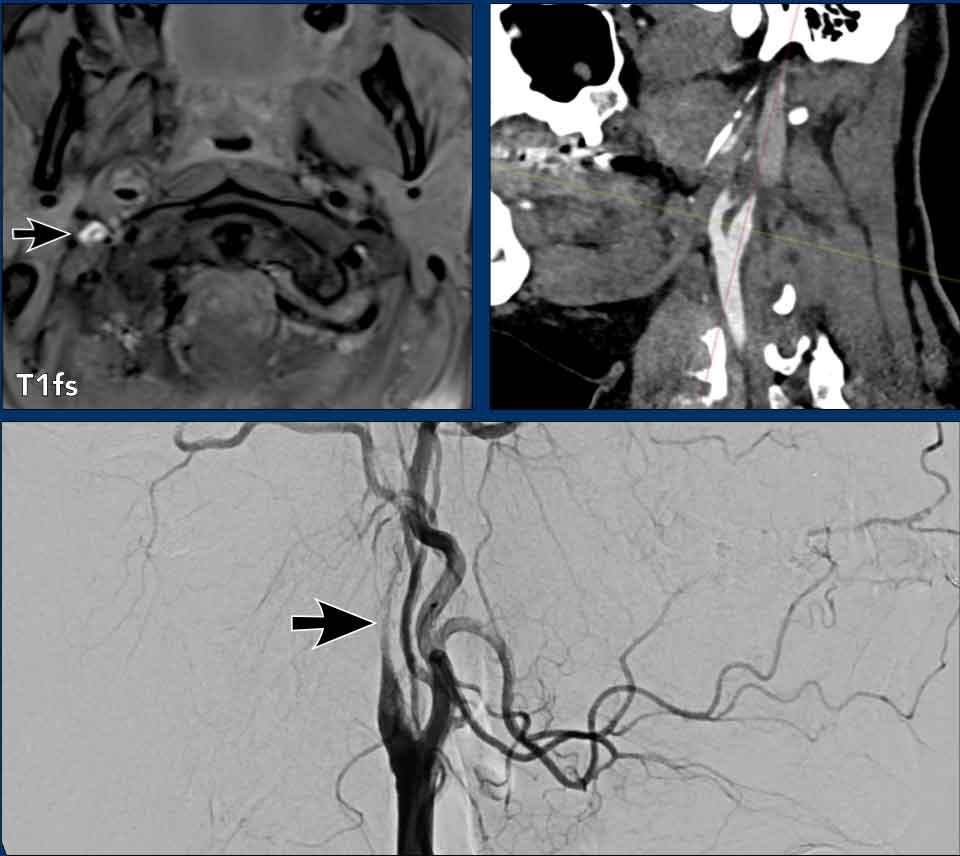
Internal Carotid Dissection
Case Presentation
A 39-year-old female with a history of multifocal fibromuscular dysplasia (FMD) presented with right sided brain ischemia.
Imaging
- Location: The lesion is within the right carotid artery, making it a carotid space lesion.
- Normal contents: vascular structures, nerves and sympathetic nervous plexus, lymph nodes and congenital remnants
- MRI Findings
- T1 with fat saturation shows a crescent-shaped high signal in the wall of the right internal carotid artery (black arrow), suggestive for being a hematoma in the tunica media.
- Notice that the flow void of the true lumen lays eccentric.
- CT Findings
- Dilatation of the internal carotid artery secondary to an intramural hematoma, a crescent-shape mural thrombus and decreased contrast enhancement distal tot the lesion.
- DSA Findings
- Flame-shaped configuration in the internal carotid artery, indicating a compressed true lumen, which can even be occluded in cases of severe compression.
Differential diagnosis
- ICA thrombus: typically an intraluminal filling defect often associated with (calcified) plaque
- ICA dissection: sometimes a clear intima flap, but often an eccentric mural hematoma with narrowing of the true lumen
- ICA web: more a thin shelf-like protrusion of the intimal fibrous tissue into the bulb of the carotid artery from the posterior wall
*See also ‘How to differentiate carotid obstructions’
Final diagnosis
Internal carotid dissection causing a brain stroke.
Note
- Patients with FMD have increased risk (prevalence of 10-20%) of spontaneous cervical carotid artery dissection.
- The vast majority of cervical carotid dissections involve the internal carotid artery (ICA) rather than the common carotid artery.
- Most common sites are 2-3 cm superior to the common carotid bifurcation and at the petrous part at the skull base since the carotid artery is tethered as it enters the carotid canal.
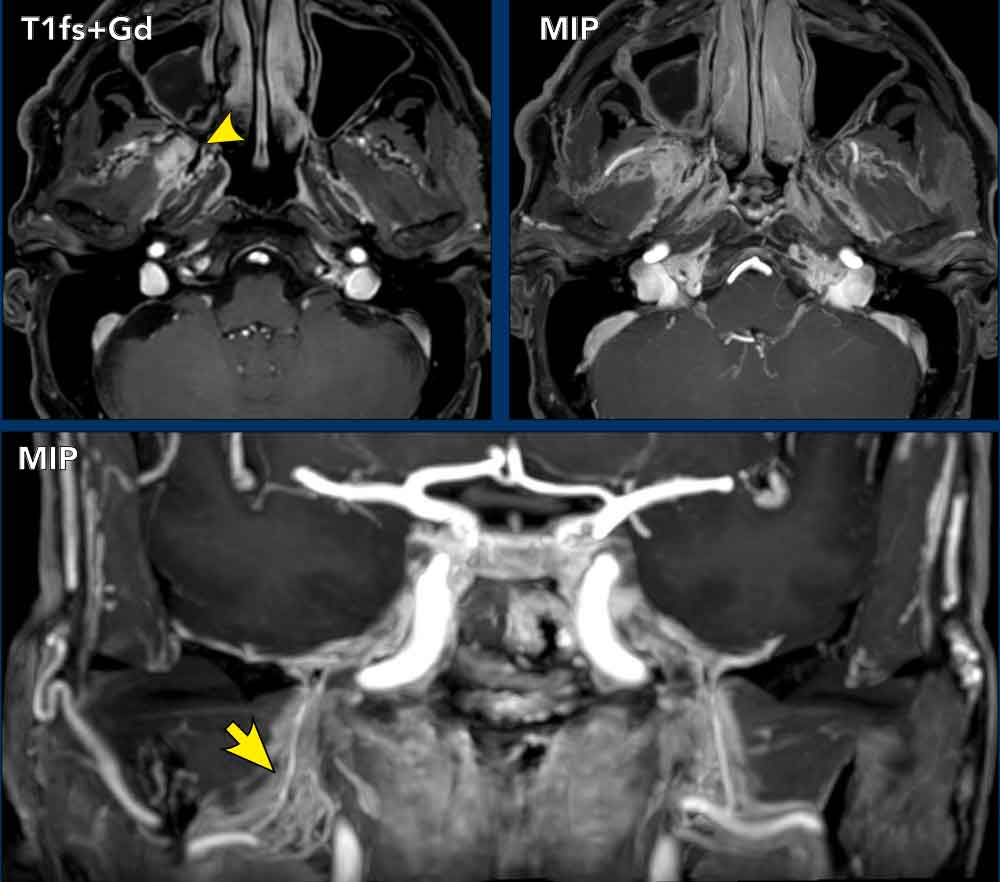
Thrombophlebitis of the internal jugular vein
Case Presentation
A 74-year-old female presented with rapid onset of left neck pain and swelling, progressively worsening over several days
Imaging
- Thrombophlebitis of the internal jugular vein (arrow and arrowheads).
- Peripheral consolidation in the left lung, likely secondary to a septic embolus (black arrow).
- No identifiable cause was identified in the neck region.
Conclusion
The findings are consistent with Lemierre syndrome, a rare but life-threatening condition characterized by:
- Thrombophlebitis of the internal jugular vein
- Septic emboli, leading to abscesses in distant sites, most commonly the lungs (septic pulmonary emboli), though joints, bones, or other organs may also be affected.
This syndrome typically follows an oropharyngeal infection (e.g., tonsillitis, peritonsillar abscess).
Outcome: Symptoms resolved following 3 months of anticoagulation therapy.
Schwannoma of the Vagus nerve
Case Presentation
A 43 years-old male presented with headache.
A pulsatile neck mass was noted on physical examination.
Initial suspicion was paraganglioma (patient also reported palpitations), however, no catecholamine overactivity was detected in blood tests.
FNAC
Right lateral neck puncture revealed cytological features consistent with a mesenchymal lesion, most suggestive of a schwannoma.
Post-surgery
Excision of the right neck tumor; the lesion was removed in parts and confirmed to be a schwannoma with no malignant features.
Continue with the MRI...
Imaging Findings
- Location: The lesion displaces the internal and external carotid artery anteriorly, the parapharyngeal fat anteriorly, and the posterior belly of the digastric muscle laterally, making it a carotid space lesion.
- Normal contents: vascular structures, nerves and sympathetic nervous plexus, lymph nodes and congenital remnants
- US Findings
- Sharply-defined lesion dorsal to the right common carotid artery.
- MRI Findings
- T1 iso-intense to muscle, T2 hyperintense to muscle sharply-defined lesion in the right carotid space with homogenous contrast enhancement.
- Some focal area’s of high signal on T2 may indicate intralesional cysts.
- The lesions displaces the internal and external carotid artery anteriorly and the internal jugular vein is flattened and displaced posteriorly.
Differential diagnosis
- Schwannoma: the most common benign neurogenic tumor of the carotid space. They are typically well-defined, T1 iso-intense to muscle, T2 hyperintense, homogenous enhancement (sometimes heterogenous in larger lesions due to cystic degeneration), absence of flow voids and slow growth.
- Neurofibroma: same features as schwannoma, can usually not be differentiated from each other.
- Paraganglioma: often centered between the internal and external carotid artery and typically show multiple intralesional flow voids creating a ‘salt and pepper’ appearance on MRI
- Meningioma: rare extracranial carotid space lesions, usually extending from the skull base with hyperostosis or foraminal enlargement and may show a dural tail
FNA: Right lateral neck puncture revealed cytological features consistent with a mesenchymal lesion, most suggestive of a schwannoma.
Post-surgery
Excision of the right neck tumor; the lesion was removed in parts and confirmed to be a schwannoma with no malignant features.
Note
- May raise symptoms such as dysphagia, internal jugular vein occlusion, Horner syndrome, vocal cord paralysis, sleep apneu or sore throat.
- The combination of a well-circumscribed carotid space mass, T2 hyperintensity, homogeneous enhancement, absence of flow voids, and possible intralesional cystic degeneration strongly favors a schwannoma. Vagal schwannoma usually separates the internal carotid artery and internal jugular vein, while sympathetic chain schwannoma typically displaces both vessels together without splaying them.
- Intralesional cystic changes are common in schwannomas, especially when they exceed 3–4 cm, whereas paragangliomas are usually much more vascular and demonstrate prominent flow voids rather than cystic degeneration.
Glomus caroticum
Case presentation
A 67-year-old male with a SDHD mutation had a screening MRI.
Imaging Findings
- Location: The lesion is nested centered at the carotid bifurcation between the right internal and external carotid artery, making it a carotid space lesion.
- Normal contents: vascular structures, nerves and sympathetic nervous plexus, lymph nodes and congenital remnants
- MR Findings
- Axial T1 shows a lesion with hyperintense foci “salt” (secondary to subacute blood) and hypointense foci “pepper” (due to fast flow) appearance.
- Axial T2 shows shows a lesion with hyperintense foci “salt” (secondary to slow flow) and hypointense foci “pepper” (due to fast flow) appearance
- Axial T1 with contras shows intense enhancement
- Dynamic contrast enhanced MRA shows rapid and intense enhancement in the arterial fphase.
Differential diagnosis
Similar to the previous case of vagal schwannoma.
However the key features such as hypervascular lesion, splaying of the ICA and ECA (Lyre sign) and the marked enhancement make a carotid body paraglioma (glomus caroticum) most likely.
The SDHD mutation is strongly linked to hereditary paraganglioma syndromes (specifically glomus tumors of the head and neck).
Meningeoma extending caudally into CS
Case Presentation
A 79-year-old male known with multiple paragangliomas in the neck, presents with left abducens nerve palsy.
Imaging
- Location: Lesion in the left carotid space between the carotid artery and the internal jugular vein (arrowheads).
- Normal Contents: vascular structures, nerves and sympathetic nervous plexus, lymph nodes and congenital remnants
- MR Findings
- Strongly enhancing lesion between the carotid artery and the internal jugular vein, which could be interpreted as a paraganglioma based on the location.
Continue with more MR images...
MR Findings
- More cranial images show the lesion growing through the jugular foramen (arrow).
- Extensive involvement of the left clivus and both nodular dural thickening as well as dural tail formation indicative of an intracranial extra-axial lesion (e.g. meningioma).
Continue with more MR images...
MR Findings
- Involvement of the left Dorello’s canal by the mass explaining the abducens nerve palsy of the patient.
Note: normal right abducens nerve coursing to Dorello’s canal (arrow). - Sagittal reconstruction showing the mass growing inferiorly through the jugular foramen in the carotid space (dorsal to the internal carotid artery).
- Coronal reconstruction: a small part of the mass extends in the middle ear (arrow). This was biopsied endoscopically.
Pathological diagnosis: Meningioma
Perivertebral space
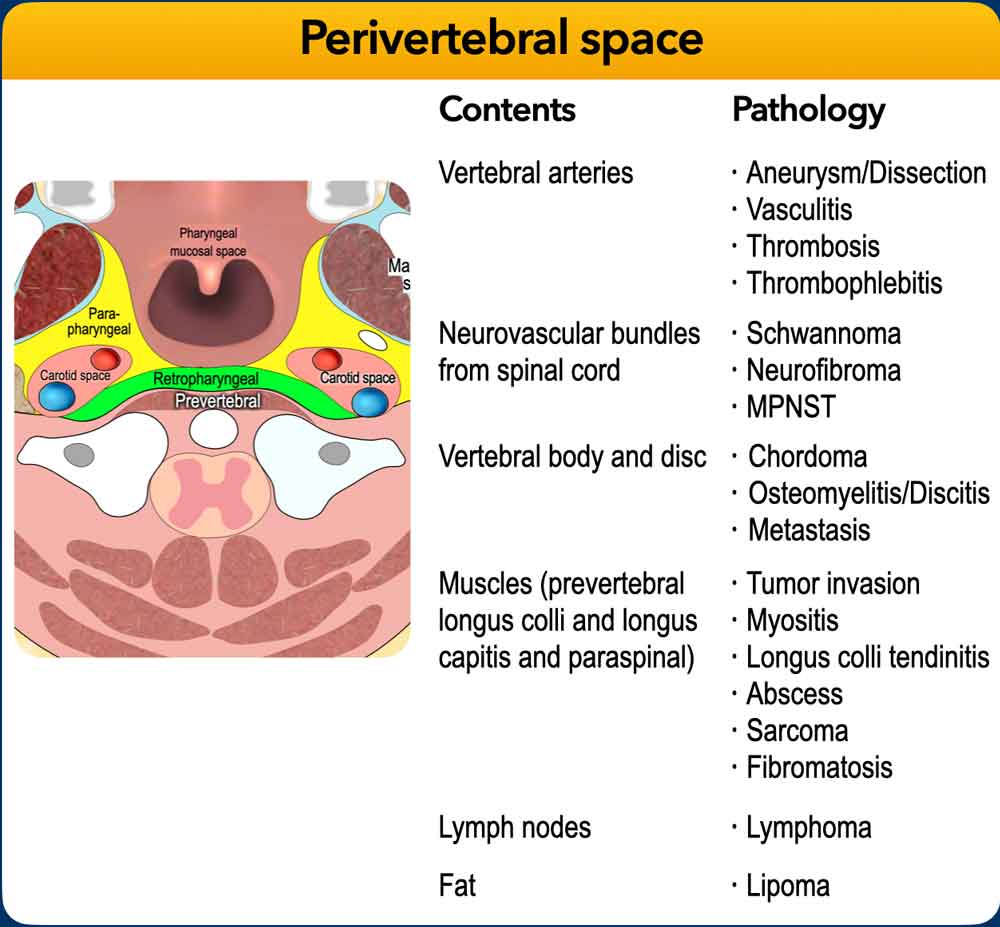
The perivertebral space includes both the prevertebral space and paraspinal components and extends from the skull base to the clavicle.
The prevertebral space is located directly anterior to the vertebral bodies and the prevertebral muscles (longus colli, longus capitis).
Lesion localization
Localization is guided by mass effect on the longus colli muscle:
- Anterior displacement: Suggests a perivertebral space lesion.
- Posterior displacement: Suggests pathology arising from the retropharyngeal space (e.g., retropharyngeal abscess, thyroid mass).
Differential Diagnosis
- Mesenchymal tumors (both benign and malignant)
- Pediatric: Rhabdomyosarcoma (primary consideration)
- Direct extension: Nasopharyngeal carcinoma, lymphoma
- Skeletal malignancies: Metastases, lymphoma, plasmacytoma, Ewing sarcoma, osteosarcoma
- Non-malignant pathology from the cervical spine especially spondylodiscitis
Tumor extension
Tumor spread into the danger space (DL) and deep cervical fascia (DCF) may fix and jeopardize the aerodigestive tract.
Always assess for epidural extension, and also consider the neural foraminas as a path of least resistance.
Acute calcific tendinitis of the longus colli
Case Presentation
A 48-year-old female presented with progressive neck pain since a few days followed by swallowing complaints and torticollis. She had no fever.
Endoscopy of the esophagus did not reveal any abnormalities
Imaging
- Location: The lesion displaces the longus colli muscles anteriorly, suggestiong a perivertebral space lesion
- Normal contents: vascular structures, nerves, vertebral bodies and disci, muscles, lymph nodes and fat
- MR Findings
- Sagittal and axial T2 show prevetebral soft tissue swelling (black arrow) including retropharyngeal edema, and swelling of the longus colli muscles.
- Axial T1 and CT show calcifications within the longus colli situated in the prevertebral space (yellow arrows).
Diagnosis
- Acute calcific tendinitis of the longus colli muscle.
Differential Diagnosis
- Retropharyngeal space abscess: Typically presents as a fluid collection with rim enhancement on imaging, without anterior displacement of the longus colli muscles.
- Spondylodiscitis: Usually demonstrates edema and possible erosions of the affected vertebral bodies, often accompanied by epidural or prevertebral phlegmon or abscess; prevertebral calcifications are absent.
Clinical Features
Acute calcific tendinitis of the longus colli is a self-limiting inflammatory condition characterized by the sudden onset of neck pain and stiffness, frequently associated with dysphagia. It results from the deposition of calcium hydroxyapatite crystals within the tendons of the longus colli muscle, triggering an acute inflammatory response.
Management
The patient was managed conservatively with nonsteroidal anti-inflammatory drugs (NSAIDs), achieving symptomatic relief within one week.
Companion case of a non-acute calcific tendinitis of the longus colli.
Imaging
- Faint fatline visible in the expected position of the prevertebral fascia with thickening of the posterior oropharyngeal wall (arrowhweads).
- Just posterior to this fatline: coarse macrocalcifications in the longus colli tendon (black arrow).
- No retropharyngeal effusion.

Spondylodiscitis with abscess
Case presentation
A 39-year-old female presented with chronic neck pain for months and since one week of progressive left arm weakness, gait deterioration and severe, debilitating neck pain leading to functional impairment.
Her medical history revealed a previous CMV infection.
She was EBV and HIV seropositive
Imaging
- Location: Anterior displacement of both longus colli muscles, indicative of a lesion located in the perivertebral space.
- Normal contents: vascular structures, nerves, vertebral bodiesy and disci, muscles, lymph nodes and fat
- Findings
- Perivertebral soft tissue swelling and enhancement with anterior displacement of the longus colli muscles.
- On the sagittal image a fluid collection with rim enhancement anterior of C2 (arrow).
- CT: angulation and erosion of the vertebral endplates of C2 and C3.
- B1000 series of the DWI sequences shows high signal in the fluid collection anterior of vertebra C2 (with low ADC values), indicating an abscess.
Diagnosis
- Spondylodiscitis
Typically presents with perivertebral soft tissue swelling, phlegmon or abscess formation, narrowed disc space, pathological enhancement, and endplate destruction. - Spinal biopsy: Necrotizing granulomatous inflammation.
- PCR: positive for Mycobacterium tuberculosis (TB).
Differential diagnosis
- Vertebral body metastasis: Usually characterized by vertebral body destruction that spares the disc space. Extravertebral soft tissue extension may mimic a phlegmon, but typically lacks edema. Additional metastases may be visible in the scan trajectory view.
Notes
- In the suprahyoid cervical spine, prevertebral and retropharyngeal spread is clinically critical, as it can cause airway compromise.
- The cervical spine is particularly important because infection can spread into
- Retropharyngeal space (airway compromise)
- Mediastinum (via danger space)
- Epidural space (cord compression risk)
- Disc involvement remains the key imaging feature distinguishing infection from tumor.
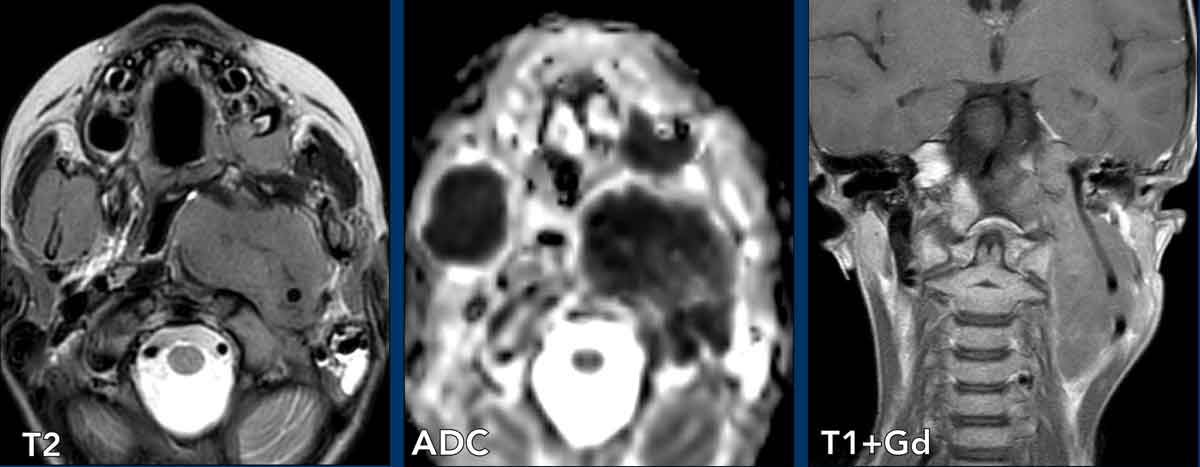
Chordoma
Case presentation
A 62-year-old male presented with a history of persistent nasal congestion and aural fullness for several months, accompanied by progressive hearing loss.
Otologic examination revealed dull sensation in both ears, with Weber lateralizing to the left and negative Rinne bilaterally.
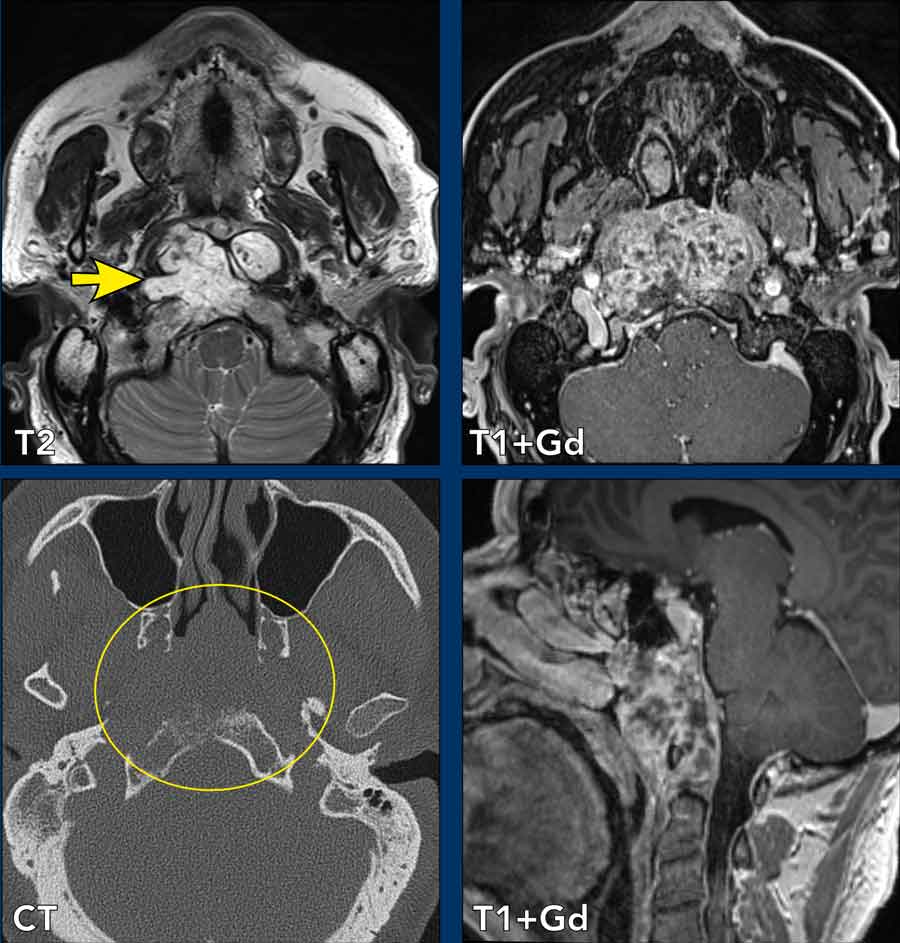
Imaging
- Location: Lesion centered in the clivus with anterior displacement of both longus colli muscles, indicative of a lesion located in the perivertebral space.
- Normal contents: vascular structures, nerves, vertebral bodiesy and disci, muscles, lymph nodes and fat
- Findings
- High T2 signal intensity lobulated mass centered in the clivus with low signal septations. The mass gives compression on the nasopharyngeal mucosal space. The appearance on T2 is somewhat ‘gelatinous’.
- Heterogenous enhancement
- CT: midline destructive lytical laesion at the skull base
Diagnosis
- Chordoma (most characteristic): Typically presents as a lobulated soft tissue mass lesion in the midline at the clival or C1–C2 region, demonstrating a very hyperintense T2 signal (soap or gelatinous appearance) with associated bone destruction.
Histopathological analysis confirmed the diagnosis of chordoma. The patient subsequently underwent transsphenoidal resection.
Differential diagnosis
- Chondrosarcoma: Usually an off-midline (paramedian) lesion originating from the skull base synchondrosis, often exhibiting "ring-and-arc" chondroid calcifications.
- Nasopharyngeal Carcinoma: Arises from the mucosa, typically shows less T2 hyperintensity, less bone destruction, and is often associated with lymphadenopathy.
- Metastasis or Lymphoma: Generally less T2 hyperintense; metastases tend to be more infiltrative or diffuse, while lymphoma often demonstrates homogeneous enhancement and diffusion restriction.
Benign mesenchymal tumor
Case presentation
An 18-year-old female presented with a mass in the posterior neck.
Imaging
- Location: Lesion centered between the left paraspinal cervical muscles, indicative of a lesion located in the perivertebral space.
- Normal contents: vascular structures, nerves, vertebral bodies and disci, muscles, lymph nodes and fat
- Findings
- Well -circumscribed soft tissue mass with isointense T1 signal to muscle, hyperintense T2 signal and moderate enhancement.
- Some restriction on ADC.
Differential diagnosis
- Benign mesenchymal tumor: usually well-defined, slow-growing and non-destructive to bone.
- Neurogenic tumor (schwannoma or neurofibroma): usually more T2 hyerpintens and more enhancing
- Malignant soft tissue tumor (sarcoma): usually heterogenous enhancement, more invasive and possible bone destruction.
Biopsy was performed.
Pathological diagnosis: benign mesenchymal tumor
Notes
The most common benign mesenchymal tumor in the perivertebral neck is lipoma.
Imaging behavior depends on tissue type:
- Fat → lipoma
- Myxoid → very T2 bright lesion
- Fibrous → low T2 signal
- Vascular → enhancement + phleboliths
Venolymphatic malformation
Case presentation
An 8-month-old female, born at 40+3 weeks with an uncomplicated neonatal period, was noted at birth to have a soft, nontender mass in the neck.
The swelling has persisted without change in size, and there is no associated erythema, pain, or discharge.
On examination, the mass is located left retroauricularly.
Based on the clinical findings the differential diagnosis was hemangioma, lipoma, skull defect, encephalocele, venolymphatic malformation.
Imaging
- Location: Lesion centered between the left paraspinal cervical muscles, indicative of a lesion located in the perivertebral space.
- Normal contents: vascular structures, nerves, vertebral bodiesy and disci, muscles, lymph nodes and fat.
- Findings
- US: Lesion with septations and with twinkling artifacts indicating calcifications
- MRI: Large left suboccipital well-demarcated lesion in the perivertebral space with high peripheral signal on T2W image with central low-signal areas, and fluid-fluid levels. On T1W image central low-signal regions slightly hyperintense, while the peripheral high T2 signal becomes hypointense.
- Post-Gd image shows inhomogeneous enhancement both centrally and peripherally.
- CT shows internal calcifications
Diagnosis
- Venolymphatic malformation: typically multiloculated cystic lesion, bright on T2, may show fluid-fluid levels and phleboliths. This is a congenital low-flow vascular malformation that may rise in the prevertebral muscles or paraspinal soft tissue.
Differential Diagnosis
- Venous Malformation: Phleboliths, bright T2 signal, contrast enhancement; slow Doppler flow.
- Lymphatic Malformation: often more cystic components with enhancement of septa
Transspatial pathology
The cervical neck spaces are delineated by surrounding fascial planes.
As a rule pathological processes are initially typically confined to a specific anatomical space, which aids in localizing disease and narrowing the differential diagnosis.
Pathology that can be located within multiple spaces include:
- Pathology that may extend across fascial boundaries: venolymphatic malformations, squamous cell carcinoma, and infections.
- Multifocal disease: lymphatic metastases.
Retropharyngeal abscess
Case 1
A 14-year-old male presented to the Emergency Department one week post-tonsillectomy with fever, neck swelling, and dyspnea, necessitating emergency intubation.
First look at the images
Review the imaging studies to assess the extent and spread of the infection.
CT shows a fluid collection with thick wall enhancement in the retropharyngeal space extending into various surrounding spaces
Question: Which spaces are involved?
- Retropharyngeal space (1)
- Carotid space (2,3)
- Perivertebral space (4)
- Epidural space (5)
A retropharyngeal abscess is not an isolated condition. It serves as a focal infection that can propagate along the cervical fascial planes into the following regions:
- Carotid space (risk of vascular complications)
- Perivertebral space (potential for osteomyelitis or discitis)
- Epidural space (risk of spinal cord compression)
Additionally, it may extend downward through the danger space, potentially reaching the mediastinum.
Case 2
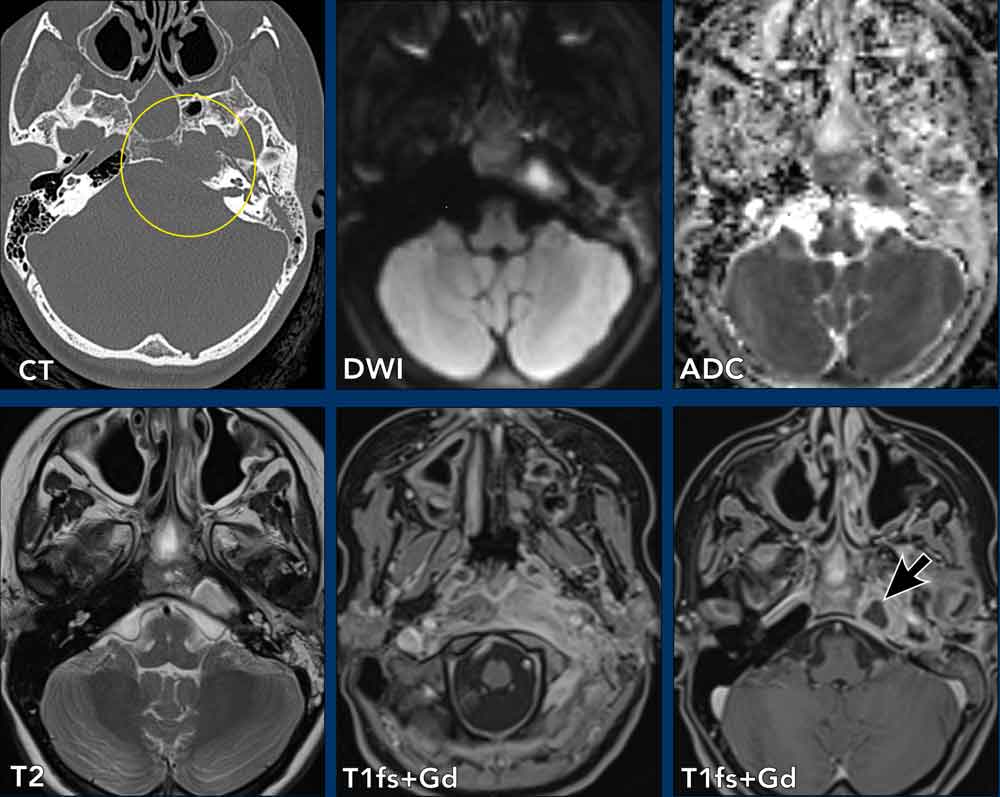
A 15-year-old female presented with persistent left otalgia, otorrhea, and progressive hearing loss since a few weeks, unresponsive to a 1-week course of amoxicillin.
Imaging
- Petrous Apex:
- Osteomyelitis of the left petrous apex (petrous apicitis), likely secondary to left otomastoiditis, complicated by a small abscess (refer to b1000 and ADC images).
Soft Tissue Involvement:- Extensive enhancing soft tissue inflammation in the left parapharyngeal space, extending into the prevertebral and paravertebral spaces, correlating with the clinical presentation of torticollis.
Intracranial Extension:- Inflammatory enhancement extending intracranially into the left cavernous sinus and Meckel’s cave.
- Enhancing dural thickening in the retroclival region and within the left internal auditory canal, consistent with skull base involvement.
Lymphadenopathy:- Enlarged retropharyngeal lymph nodes with suppurative features.
- Left cervical lymphadenopathy (levels I–V), most likely reactive in nature.
Diagnosis
Skull base osteomyelitis secondary to otomastoiditis with an abscess at the petrous apex
Treatment
Left tympanoplasty with tube insertion, and endonasal transsphenoidal drainage of purulent material from the sphenoid sinus, clivus, and petrous bone.
Cultures guided antibiotic adjustment, and the patient showed rapid clinical improvement.
Note
MRI of otomastoiditis is critical for detecting complications such as intracranial abscess, meningitis, cranial nerve complications, sigmoid sinus thrombosis, petrous apicitis, skull base osteomyelitis, and deep neck space extension into the parapharyngeal, retropharyngeal, and prevertebral spaces, all of which significantly increase morbidity and mortality.
Non Hodgkin Lymphoma
Lymphoma in the suprahyoid neck is a "transspatial" disease, characterized by its tendency to permeate along soft tissue planes rather than adhering to fascial boundaries.
Lymphoma spreads via submucosal lymphatic channels, interstitial infiltration and perivascular and perineural pathways.
Lymphoma is a “space-occupying but not space-limiting” tumor and results in extensive, bulky, yet relatively homogeneous masses that frequently cross multiple deep neck spaces.
Notably, it typically infiltrates rather than destroys and does not cause significant necrosis or obstruction in its early stages.
Case 3
Boy, 8 years. Diffuse large B cell NHL.
Question: which spaces are involved?
- Bilateral masticator space
- Left: carotid space (carotid encasement), retropharyngeal space, oral cavity (maxilla)
Case 4
Male, 77 years. Diffuse large B cell NHL
Which spaces are involved?
- Bilateral nasal cavity, sphenoid sinus
- Left masticator space, infratemporal fossa and pterypalatine fossa.

Case 5
Male, 76 years. Diffuse large B cell NHL
Which spaces are involved?
- Left perivertebral space, carotid space (carotid encasement), retropharyngeal space and (minimal) parotid space.
- Note: additional mildly enlarged lymph nodes (arrows).
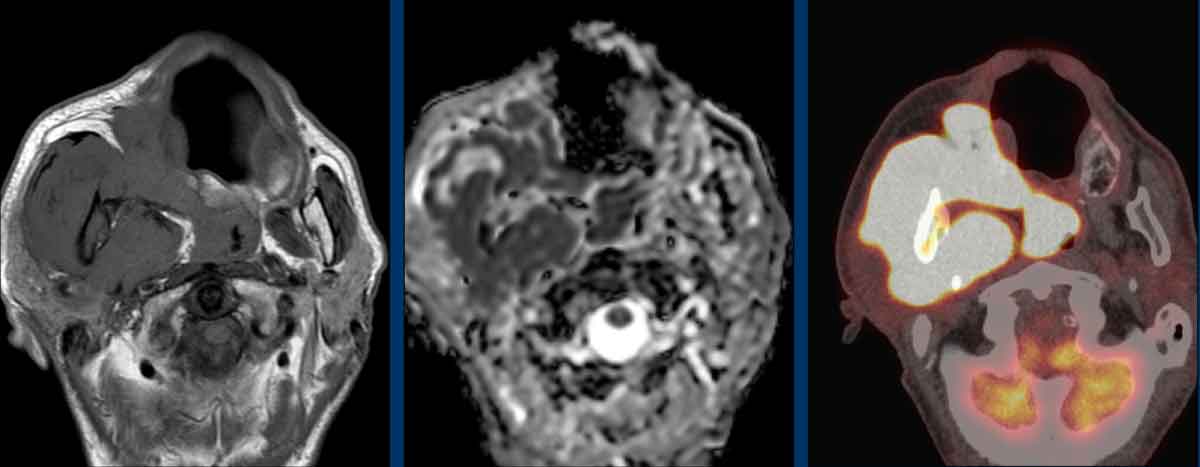
Case 6
Male, 70 years. Diffuse large B cell NHL
Which spaces are involved?
- Right masticator space, carotid space, retropharyngeal space, parotid space, pharyngeal mucosal space (nasopharynx).
- Note: abnormal bone marrow signal in the right mandibular ramus indicative of NHL-involvement.