Craniosynostosis
Joosje Bomer-Skogstad, Marjolein Dremmen, Irene Mathijssen and Robin Smithuis
Department of Radiology of Akershus University Hospital in Lørenskog, Norway, Departments of Radiology and Plastic Surgery of Erasmus Medical Center in Rotterdam and Department of Radiology of Alrijne Hospital in Leiderdorp, the Netherlands
In this review we will discuss imaging in craniosynostosis.
Craniosynostosis refers to the premature closure of sutures of the skull and results in an abnormal head shape.
It is a rare disorder with a prevalence of around 1 in 1500.
Most cases occur already prenatally and will be diagnosed in the first few months of life.
It may also be diagnosed intrauterine, but antenatal imaging is beyond the scope of this article.
Introduction
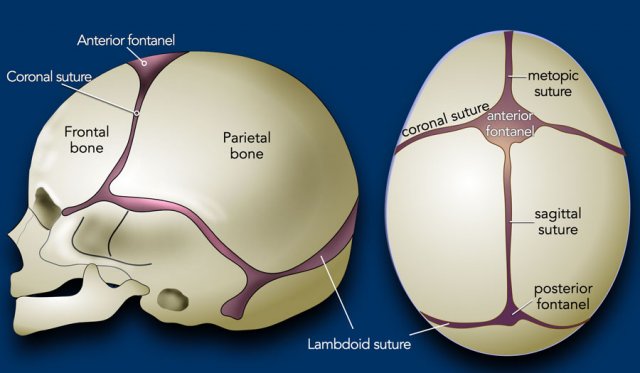
Normal skull
In the first few years of life the brain grows fast and the skull grows along with it.
This requires open sutures for enchondral growth.
At 1 year of age around 65% of skull growth is accomplished, with the growth rate thereafter slowing down, and reaching around 90% at 5 years of age.
Most craniosynostoses are the result of an intrinsic defect in the suture.
Craniosynostosis may be part of a syndrome and in those cases the craniosynostosis is often multi-sutural and there may be other anomalies (cardiac, kidney and skeletal).

Clinical evaluation
In the past decades there has been an increase in the number of children seeking medical attention because of an abnormal head shape, which is now reported as high as 1 in 5. Most cases are a positional plagiocephaly rather than a real craniosynostosis. This is often related to the advice of sleeping on the back to prevent sudden infant death syndrome.
A well-trained clinician will often be able to recognize the typical presentation of a positional plagiocephaly and distinguish from its main differential diagnosis of a unilateral lambdoid stenosis (see below).
The parents may then be reassured because the condition is self-limiting and with adequate advice usually reversible.
In case of a clinical high suspicion of a craniosynostosis timely reference to a specialized center may be advisable before diagnostic imaging is started (figure).
Overview craniosynostoses
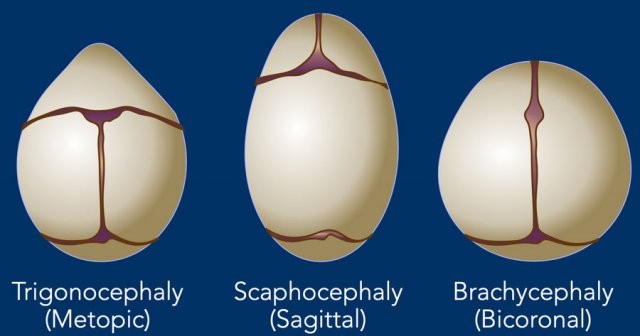
Unisutural and Bicoronal
In craniosynostosis the skull deformity is present from birth and will be progressive.
Timely diagnosis is important, as earlier treatment leads to a better outcome.
In unisutural and bicoronal craniosynostosis a specific head shape may be expected, depending on the involved suture.
This is depicted in the illustration.
In multisutural involvement the changes are more complex and cannot easily be predicted.

Plagiocephaly
In plagiocephaly, also known as flat head syndrome, there is an asymmetrical flattening of one side of the skull.
A mild and widespread form of plagiocephaly is caused by remaining in a supine position for prolonged periods, as discussed above.
This is called deformational plagiocephaly. There is no synostosis and all the sutures are open.
The synostotic form of plagiocephaly can be on the anterior side due to unicoronal closure or on the posterior side due to closure of a lambdoid suture on one side.
Imaging
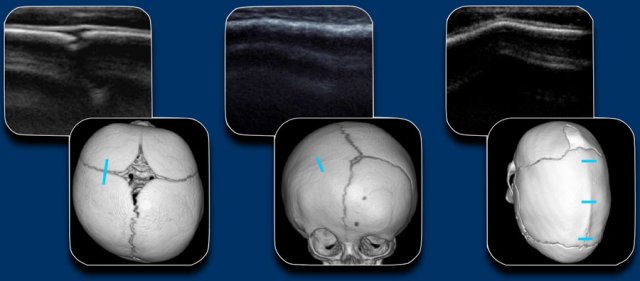
When a craniosynostosis is suspected, the first line imaging will be ultrasound or x-rays, depending on local expertise and preferences.
Because of lack of radiation, ultrasound is the preferred method.
In case of high clinical suspicion low dose 3D CT is preferred.
The figure shows the US of a normal suture, an unilateral coronal stenosis and a sagittal stenosis with ridge.
Skull radiographs
demonstrating open sutures.
Be aware that radiographs have a limited value for assessment of the sagittal suture and a partial closure of the sagittal suture may be overlooked.
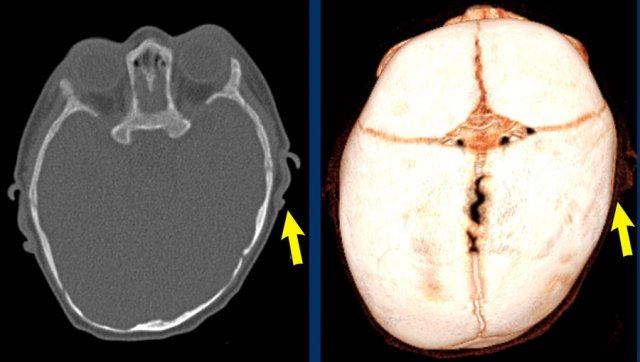
3D CT
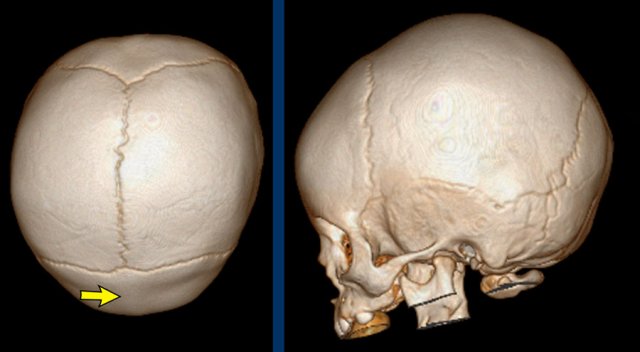
The images show open sutures in a child with a physiologically closed metopic suture (arrow).
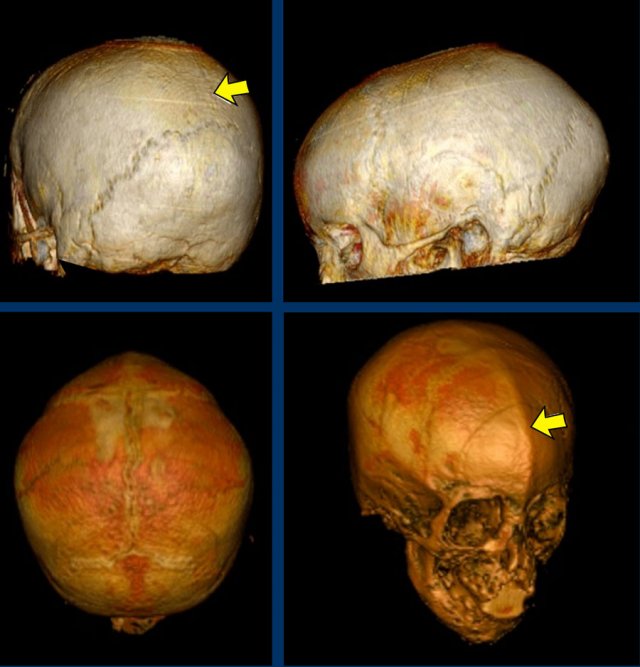 Images courtesy of Dr K.A. Eley and Dr C. Delso
Images courtesy of Dr K.A. Eley and Dr C. Delso
MRI
It is also possible to evaluate the sutures with black bone MRI, but as MRI often requires anaesthesia this will mainly be done in conjunction with an indication for evaluation of intracranial abnormalities and complications.
Images
Black bone MRI demonstrating
closed sagittal suture (top) and closed metopic suture (down) in two different
patients.
Positional plagiocephaly
Positional or deformational plagiocephaly refers to the flattening of the head due to the baby’s preferred position.
It is not a synostosis, but the most common form of temporary skull deformity.
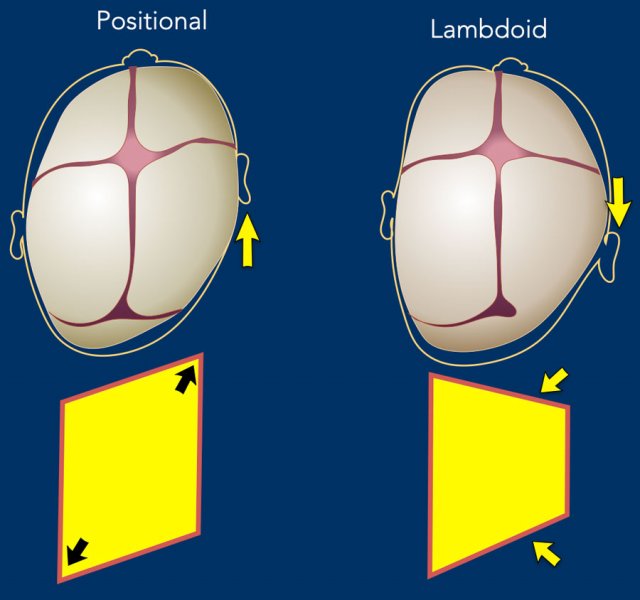
Typically, the entire side is pushed forward, hence the ear will be seen more anterior than on the contralateral side (arrow).
This is in contradiction to a posterior plagiocephaly resulting from a unilateral lambdoid suture stenosis, where the mastoid and the ear are pulled down and drawn back.
The drawing illustrates the differences.
In positional plagiocephaly the form of the head resembles a parallelogram.
In unilateral lambdoid stenosis the form of the head resembles a trapezium, because one side of the head is restricted in its growth.
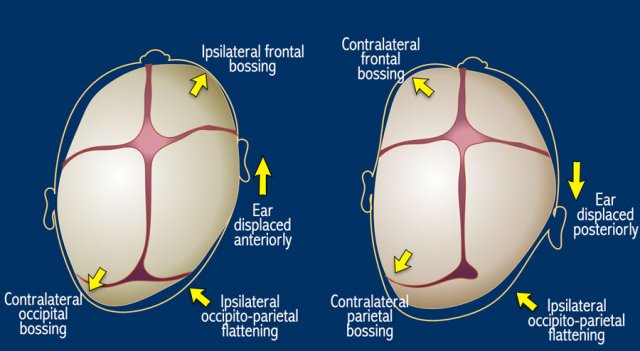
Here the same illustration with now all the differences between deformational and lambdoid plagiocephaly.
NOTE: unilateral coronal stenosis will also result in the ear being positioned more forward – however, flattening will be seen frontal (anterior plagiocephaly) instead of occipital and typically the eye is drawn up on the affected side.
Images
Positional
plagiocephaly. The left ear is pushed forward.
Note: Adequate clinical
evaluation and/or ultrasound should have obviated the need for CT.
Monosutural craniosynostosis
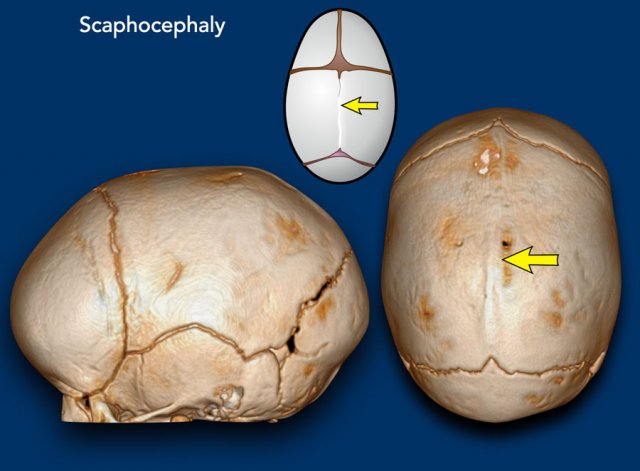
Scaphocephaly
Scaphocephaly means ‘boat shaped’ skull and results
from a premature closure of the sagittal suture (arrow).
The skull is narrow and long.
It is the most common monosutural craniosynostosis.
Sometimes it is called
dolichocephaly, as ‘dolicho’ means long.
Images
Scaphocephaly: The head has a short laterolateral and a long anteroposterior diameter.
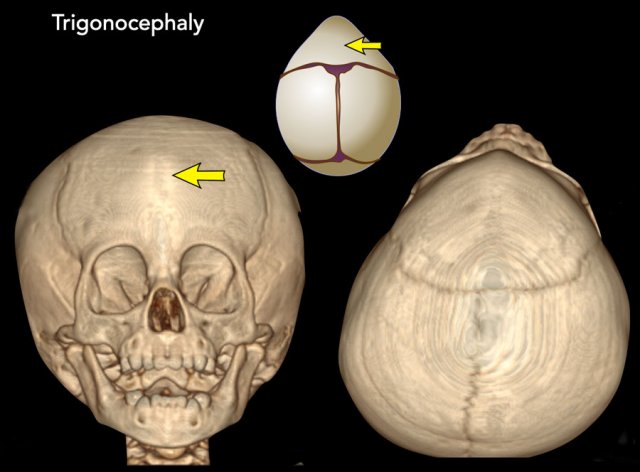
Trigonocephaly
Trigonocephaly refers to the triangular head form resulting from premature closure of the metopic suture (arrows).
Physiological closure can already start as early
as three months of age, so premature closure typically presents early.
The
frontal head volume is small with a pointy forehead and hypotelorism.
Only pronounced cases require surgery and if there is clinically no indication for surgery, a CT is not needed.
Images
Trigonocephaly: Pointy forehead and
hypotelorism. Seen from above the lateral orbital rim will be
visible.
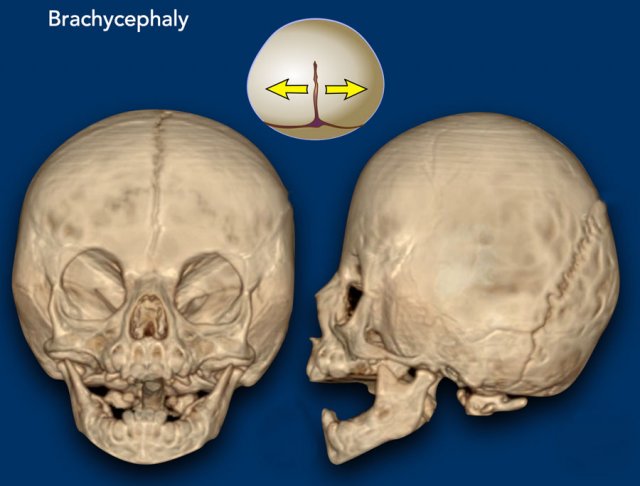
Brachycephaly
Brachycephaly results from the premature closure
of both coronal sutures.
The frontal skull base is small with
shallow eye sockets with the supraorbital rim drawn back and the head is shortened (‘brachy’) in the anteroposterior direction.
Images
Bilateral coronal synostosis with brachycephaly.
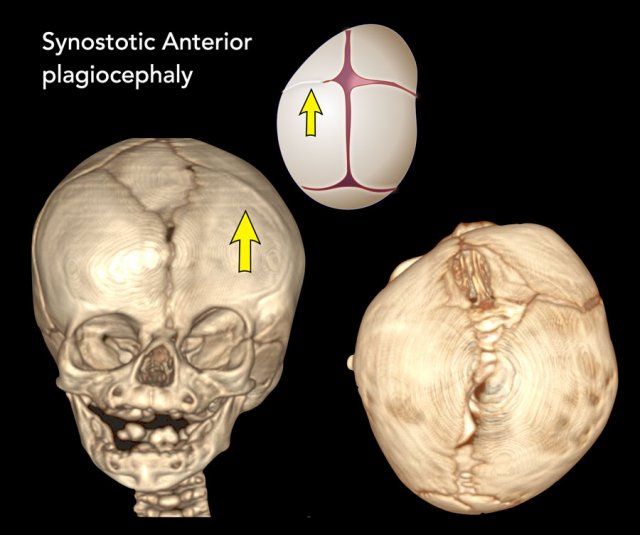
Synostotic Anterior plagiocephaly
One of the coronal sutures has closed prematurely.
The
forehead is flattened on the affected side with the eye socket drawn up, also
called a harlequin’s eye, and the nose may be deviated.
Images
Left sided coronal synostosis. The left forehead is
drawn back with the eye socket lifted up.
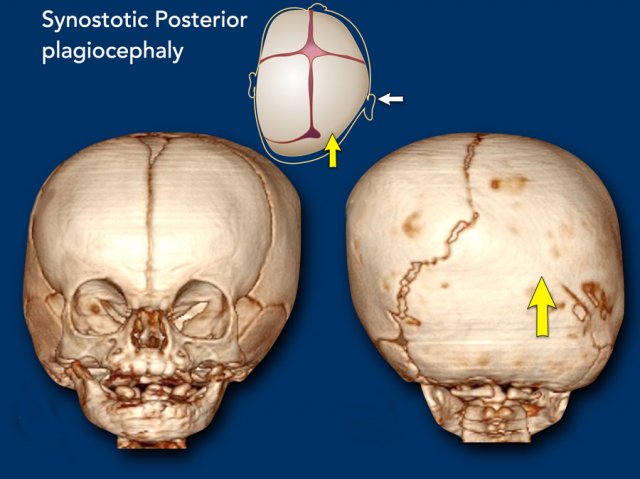
Synostotic posterior plagiocephaly
In this case the lambdoid suture has closed
prematurely.
It is the main differential diagnosis for positional plagiocephaly
(see above).
There is a risk for Chiari 1 malformation and MRI of the brain and craniocervical junction is advised.
Images
Right sided lambdoid synostose.
Contralateral occipitoparietal bossing is evident.
Multisutural craniosynostosis
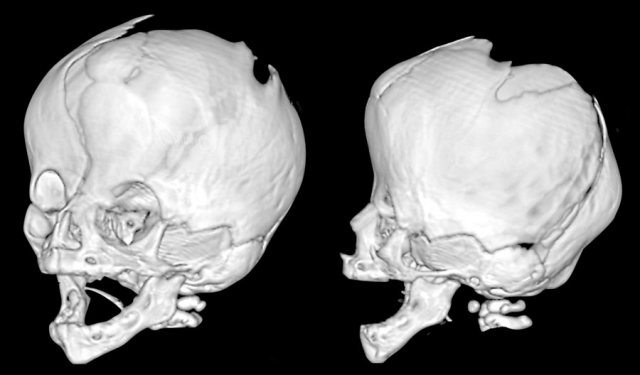
Multisutural craniosynostosis are complex
deformations.
They are usually linked to syndromes and there are several
genetic defects identified.
The best known
craniosynostoses syndromes are Pfeiffer/Crouzon, Apert, Saethre-Chotzen and
Muenke.
In the most severe cases all sutures will eventually close.
Such a
‘pansynostosis’ is a severe condition.
Images
Saethre-Chotzen syndrome. At two months of age there is a bilateral coronal
synostosis with a severely deformed head shape. The fontanel is grossly
enlarged.
Same patient as above.
At three years
old there is microcephaly from a near pan-synostosis.
Note enlarged bilateral
parietal foramina.
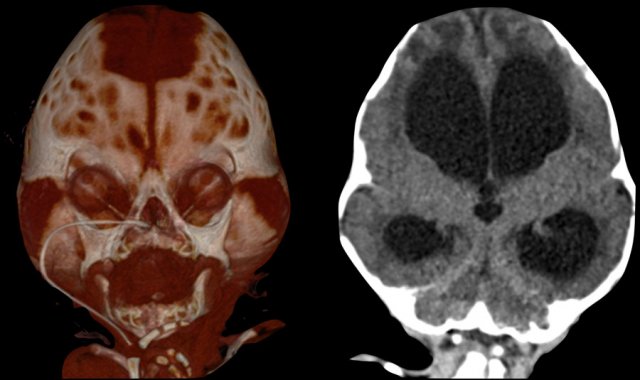
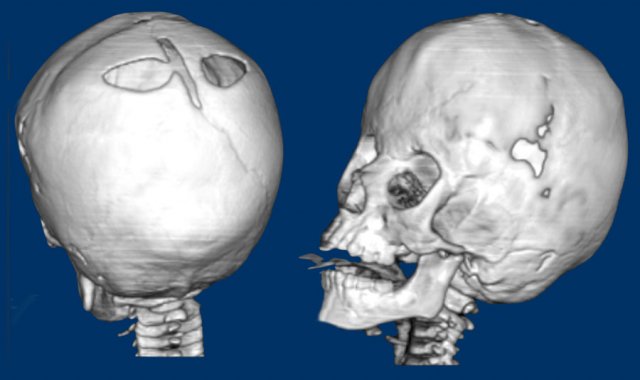
Three-month-old with Pfeiffer syndrome.
There is a bicoronal synostosis with enlarged anterior and mastoid
fontanels.
Temporal bulging give rise to a trilobate appearance, also called
‘clover leaf deformity’.
Note the ventriculomegaly with periventricular edema.
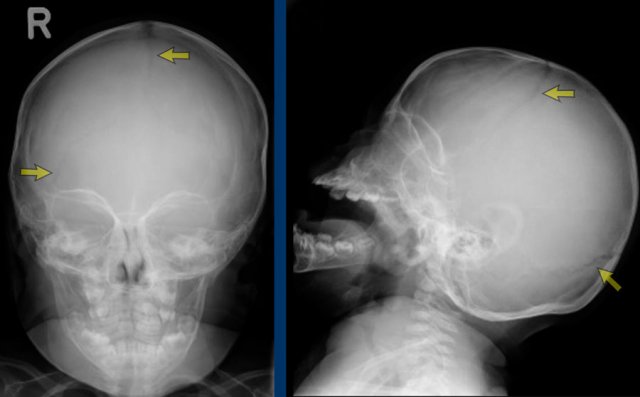
Intracranial complications
 Raised intracranial pressure
Raised intracranial pressure
MRI has a main role in detecting associated intracranial malformations and complications from multisutural craniosynostosis.
Images
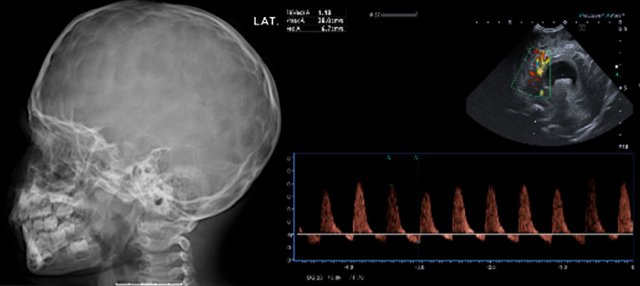
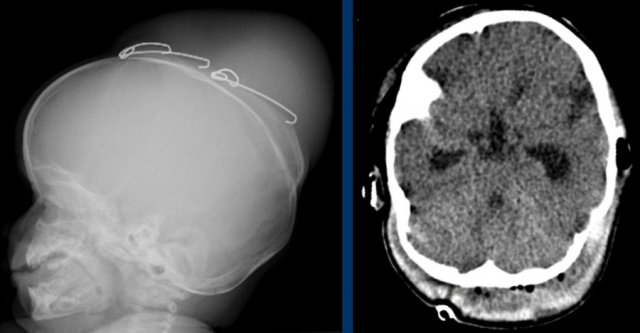
Raised intracranial
pressure.
LEFT: Impressions on a skull radiograph have a low sensitivity,
especially in young children, but when seen, are highly suspicious for raised
intracranial pressure.
RIGHT: Hydrocephalus
with inverted diastolic flow indicating high intracranial pressure.
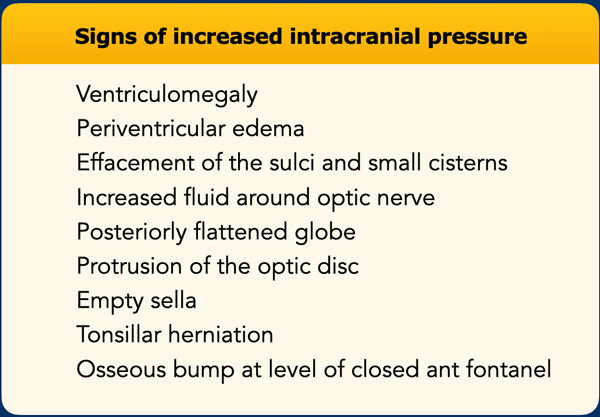
Signs that may indicate raised intracranial pressure are listed in the table on the left.
One of these findings is non-specific,
but a combination of findings should raise suspicion.
Increased intracranial
pressure may result in venous collaterals which may be important in
preoperative planning.
Chiari malformation may result in spinal syrinx.
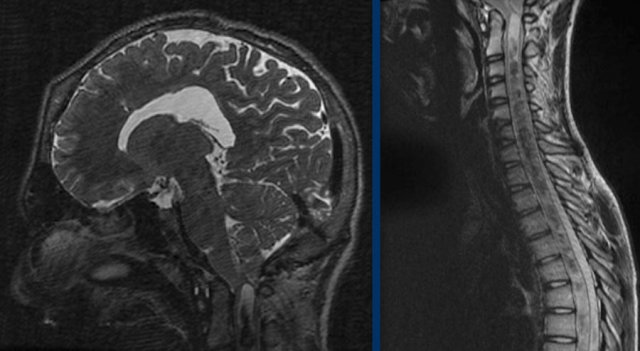
The images are of a patient with increased intracranial pressure.
There is tonsillar herniation with severe
crowding at the craniocervical junction.
This has resulted in a syrinx over the
entire length of the spinal cord.
Postoperative complications
Surgery should be conducted timely in order to reach an optimal outcome.
Timing is dependent on the deformity, but usually preferably under the age of 6 months. Post-operative complications include blood loss, infection, brain swelling and CSF leak.
Images
Direct complications:
LEFT Large effusion/hematoma
from migrating spring.
RIGHT
subgaleal hematoma with severe blood loss.
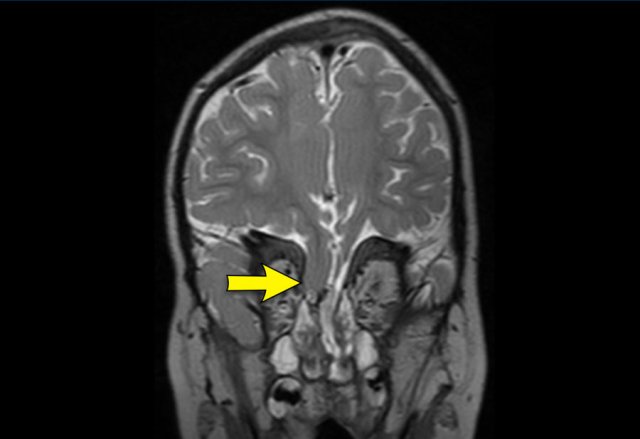
Image
Liquorroe due to CSF leak from a frontobasal
herniation in the upper nasal passage after midface surgery in a patient with Apert syndrome.
Pitfalls
 Metopic ridge
Metopic ridge
Metopic ridge
A metopic ridge alone is not equivalent to
trigonocephaly.
Children present at a later age, the frontal skull has a normal
volume and there is no hypotelorism.
It is a common deformity that can be
clinically diagnosed and does not need imaging.
As
with mild trigonocephaly, there is no need for surgery.
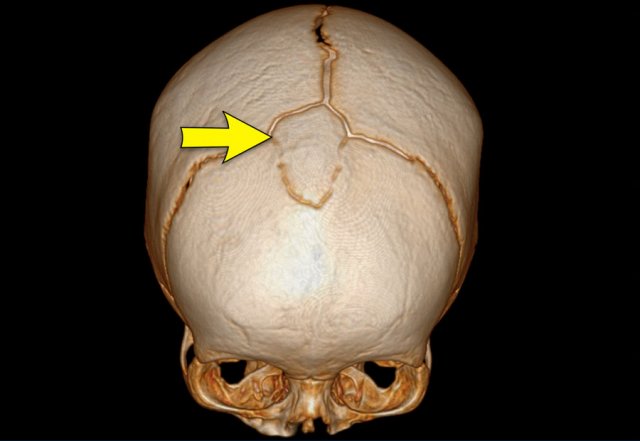
Images
Slight metopic ridge in a nine-month-old (arrow). Note that
the scan was taken for a different purpose.
Metopic ridge can be clinically
diagnosed and should not be imaged.
The anterior fontanelle has already closed
but apart from the metopic suture, the other sutures are still open.
Absent anterior fontanelle
An absent anterior fontanelle does not have to
be a reason for concern.
As long as the skull has a normal shape and
circumference, and the sutures are patent – it does not have any clinical
implications.
Image
Large wormian bone occupying the anterior
fontanelle (bregmatic bone) in a six-month-old.
The skull has a normal shape
and the sutures are open. The metopic suture has fused physiologically.