Lumbar Disc Nomenclature 2.0
Robin Smithuis
Radiology department of the Alrijne Hospital in Leiderdorp, the Netherlands
Publicationdate
This is an updated version largely based on the recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology and the American Society of Neuroradiology in 2014 (1)
Normal Disc
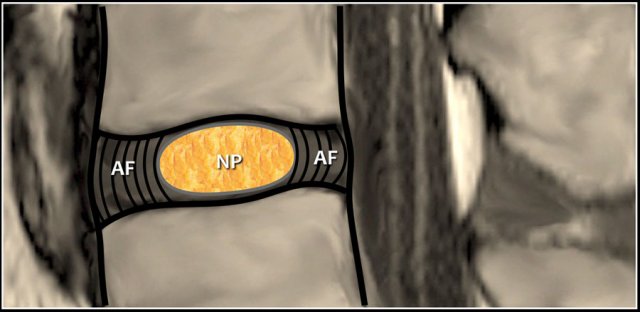 Disc is composed of soft nucleus pulposus (NP) surrounded by strong annulus fibrosus (AF)
Disc is composed of soft nucleus pulposus (NP) surrounded by strong annulus fibrosus (AF)
A normal disc is composed of a central nucleus pulposus and peripheral annulus fibrosus.
The disc is within the boundaries of the disc space, as defined, craniad and caudad by the vertebral body end plates and peripherally by the planes of the outer edges of the vertebral apophyses.
Degeneration includes any of the following: desiccation, fibrosis, narrowing of the disc space, diffuse bulging of the annulus beyond the disc space, annular fissures, mucinous degeneration of the annulus, intradiscal gas, osteophytes of the vertebral apophyses, inflammatory changes, and sclerosis of the end plates.
Bulging disc
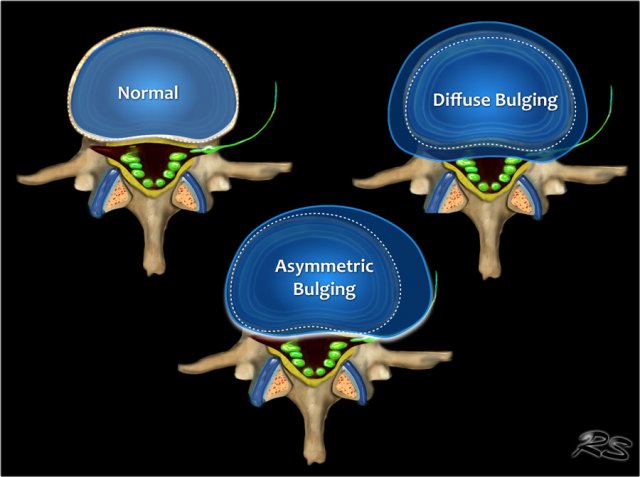
The presence of disc tissue extending beyond the edges of the ring apophyses, throughout the circumference of the disc, is called ''bulging'' and is not considered a form of herniation.
It is the result of tears in the annulus fibrosus.
Asymmetric bulging of disc tissue greater than 25% of the disc circumference is often seen as an adaptation to adjacent deformity.
Annular fissure
Annular fissures are separations between annular fibers, seen as high intensity zones on T2W-images representing fluid or granulation tissue and may enhance with gadolinium.
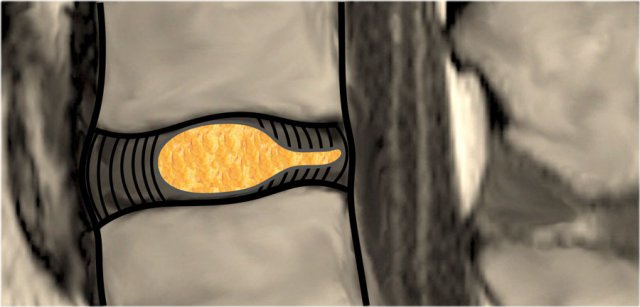
Disc Herniation
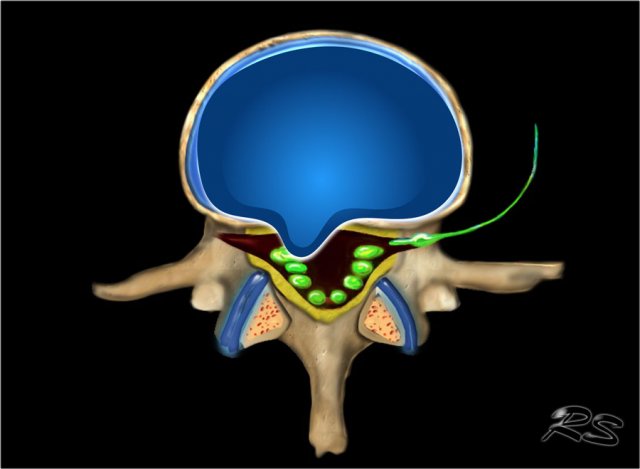
Disc herniation is defined as a focal displacement of disc material ( < 25% of the disc circumference) beyond the limits of the intervertebral disc space.
A herniated disc can be contained (covered by outer annulus fibrosus) or uncontained.
Contained herniation
Disc herniations are contained, if the displaced portion is covered by outer annulus fibers and/or the posterior longitudinal ligament.
The margins of the contained disc protrusions are smooth on imaging.
Disc herniations are uncontained when there is no such covering.
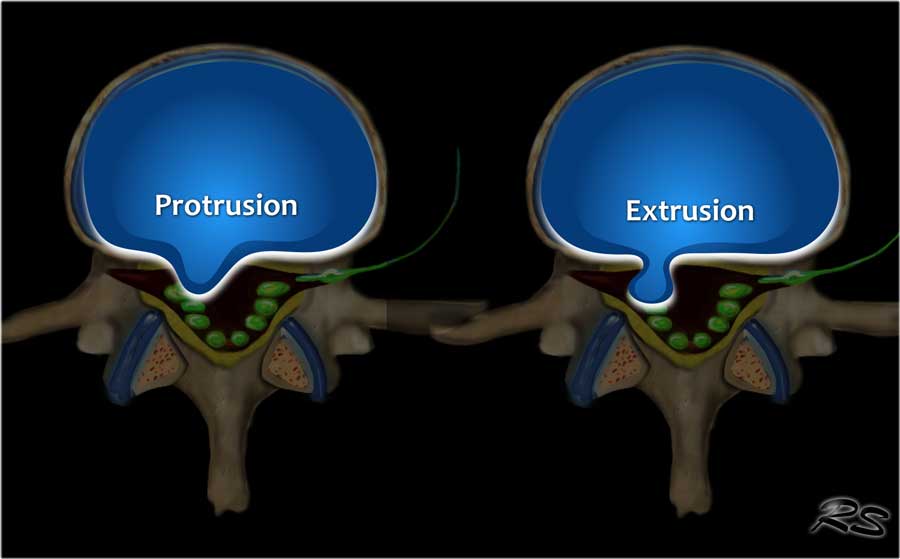 Disc Protrusion versus Extrusion
Disc Protrusion versus Extrusion
Protrusion - Extrusion
Protrusion indicates that the distance between the edges of the disc herniation is less than the distance between the edges of the base.
Extrusion is present when the distance between the edges of the disc material is greater than the distance at the base.
Extrusion is associated with a defect in the annulus fibrosus and are usually noncontained.
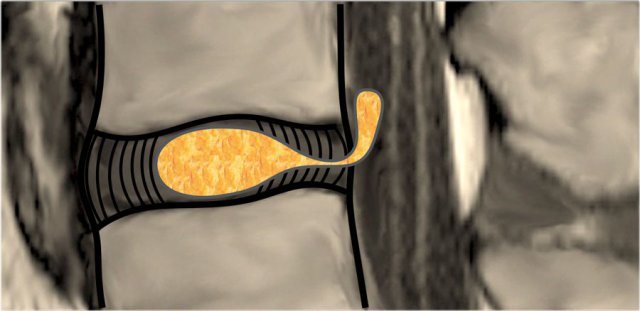 Migration of herniated disc material
Migration of herniated disc material
Migration
Migration indicates displacement of disc material away from the site of extrusion, regardless of whether sequestrated or not.
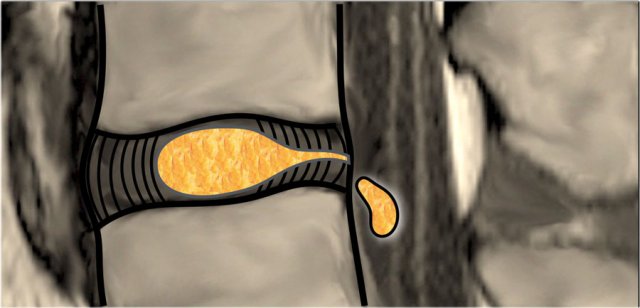
Sequestration
The term sequestration is used to indicate that the displaced disc material has lost continuity with the parent disc.
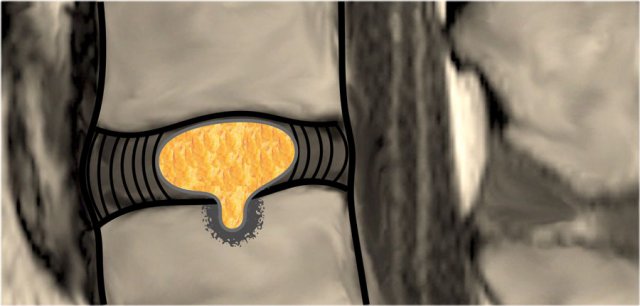
Intravertebral herniation
Intravertebral herniation or Schmorl node is herniation of disc material in the vertical direction through a gap in the vertebral end plate.
Localization of Herniated Discs
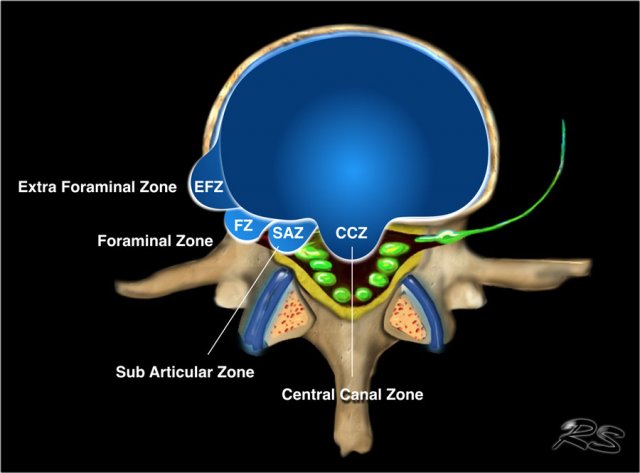
Axial plane
Central
Since the posterior longitudinal ligament (PLL) is at its thickest in this region, the disc usually herniates slightly to the left or right of this central zone.
Subarticular
Because the PLL is not as thick in this region, this is the number one region for disc herniations.
Foraminal
It is rare for a disc to herniate into the intervertebral foramen.
Only 5% to 10% of all disc herniation occur here or farther out.
When herniations do occur in this zone, they are often very troublesome for the patient.
This is because a super-delicate neural structure called the 'Dorsal Root Ganglion' (DRG) lives in this zone resulting in severe pain, sciatica and nerve cell damage.
Extraforaminal
Disc herniations in this region are uncommon.
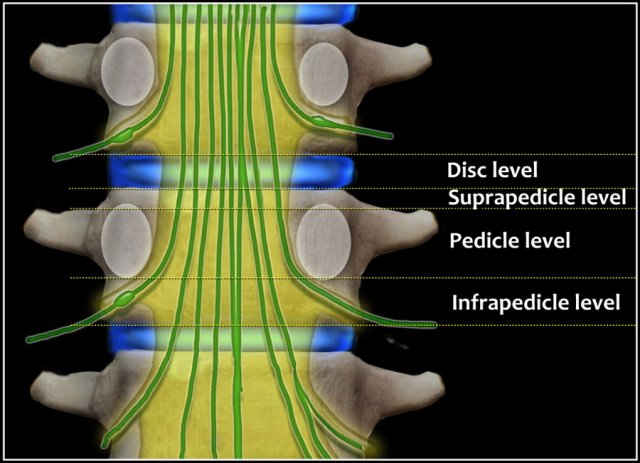
Craniocaudal plane
In the craniocaudal plane disc herniations are described as at disc level, suprapedicular level, pedicular level and infrapedicular level.
Modic classification
The Modic classification describes degenerative and inflammatory changes involving the vertebral endplates and adjacent vertebral bodies as seen on MRI.

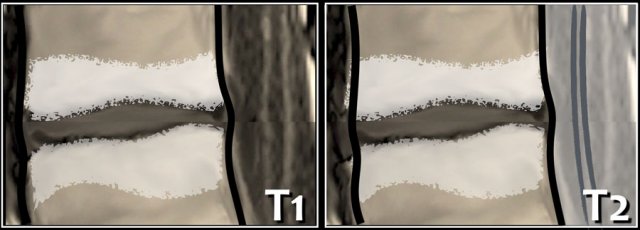
Modic Type 1
Modic Type 1 is seen as low signal intensity on T1WI and high on T2WI, representing fibrovascular tissue, inflammatory changes, and perhaps edema.
Type I changes may be chronic or acute.
There is a correlation between low back pain and Modic changes, especially Modic type 1.
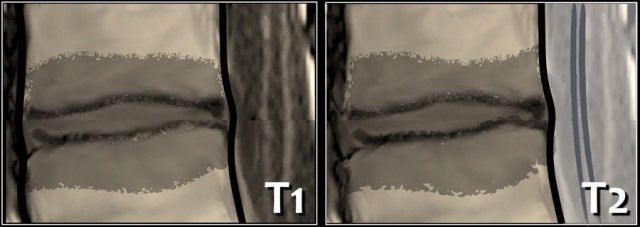
Modic Type 2
Modic Type 2 is seen as high signal intensity on T1WI and isointense or high on T2WI, representing bone marrow replacement by fat.
Modic Type 3
Modic Type 3 is seen as low signal intensity on T1WI and low on T2WI, representing reactive sclerosis.