Lines and tubes in Neonates
Joost van Schuppen, W. Onland and Rick van Rijn
Paediatric Radiology and Neonatology of the Emma's Children Hospital, Academical Medical Center, Amsterdam
Publicationdate
In this review we will discuss the normal and abnormal position of tubes and lines on a neonatal chest x-ray.
Umbilical artery line
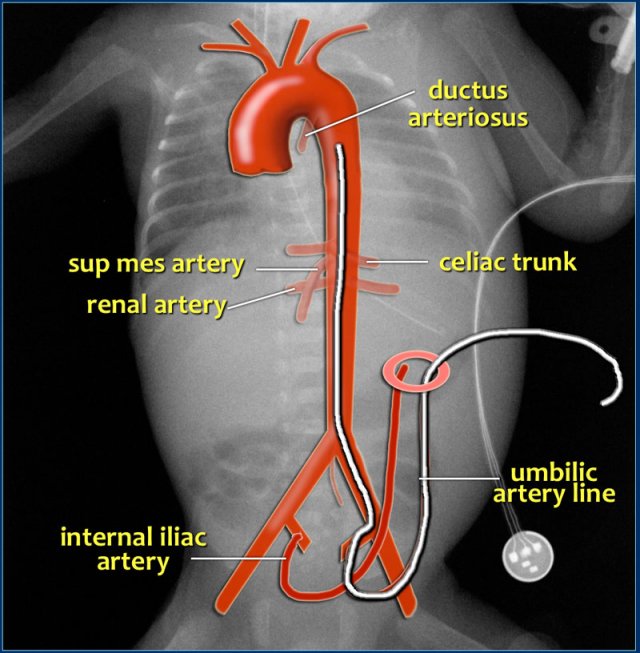
Umbilical artery catheterization provides direct access to the arterial system and allows accurate measurement of arterial blood pressure, blood sampling and intravascular access for fluids and medications.
The catheter should be passed through the umbilic artery and enter the aorta via the internal iliac artery.
It should demonstrate the typical loop from the umbilicus inferiorly into the internal iliac artery.
In order to avoid placement into aortic branches, the catheter should be either in a high position above the celiac, mesenteric and renal arteries or in a low position below the inferior mesenteric artery:
- high position: T6-T9
- low position: L3-L5
The high position is advisable since it leads to less vascular complications (15).
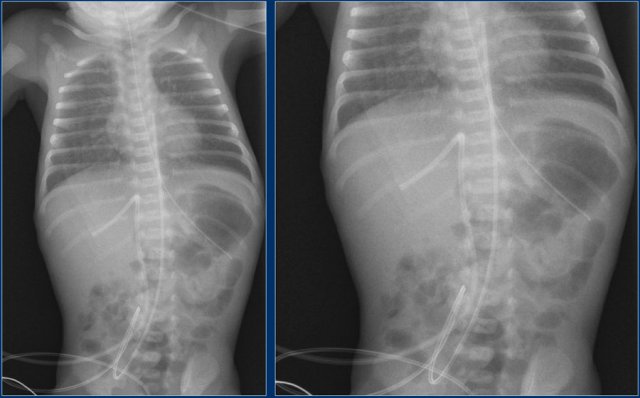
Umbilical artery line (2)
First study the images.
Then continue reading.
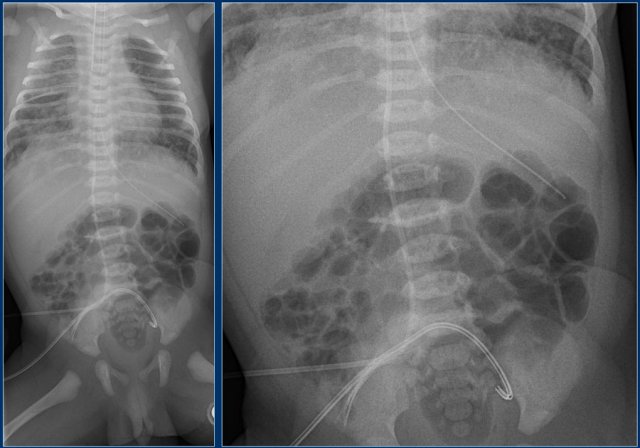
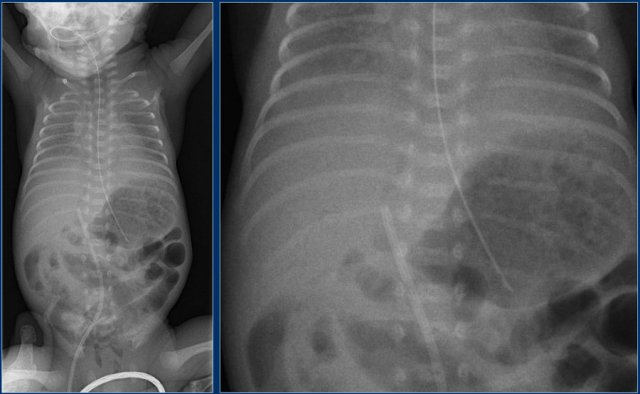
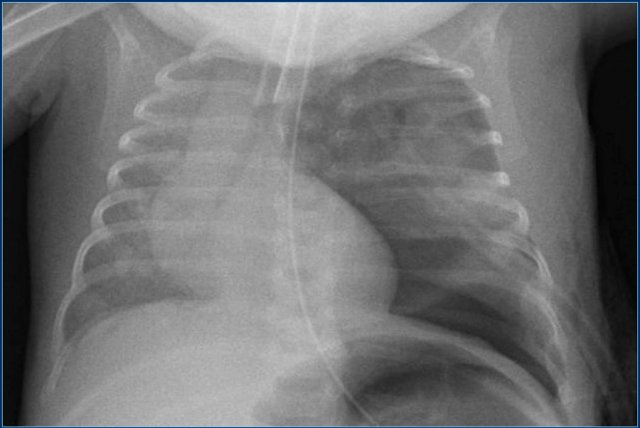
The findings are:
- Umbilical artery line in a good high position.
- Malposition of umbilical vein line in right portal vein.
- Skin folds over right basal thorax, which should not be mistaken for a pneumothorax. They typically do not follow anatomical borders.
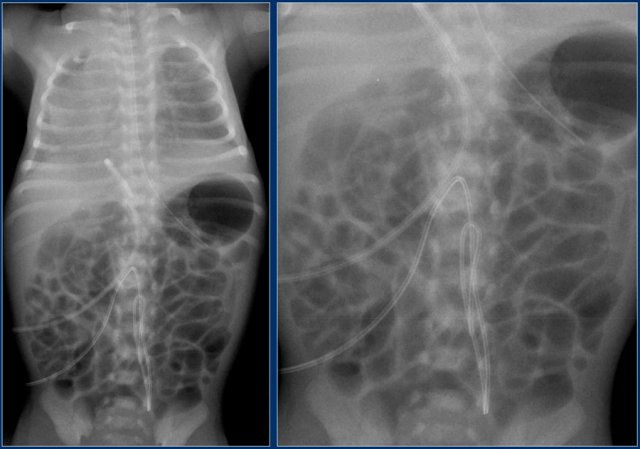
Umbilical artery line (3)
First study the images.
Then continue reading.
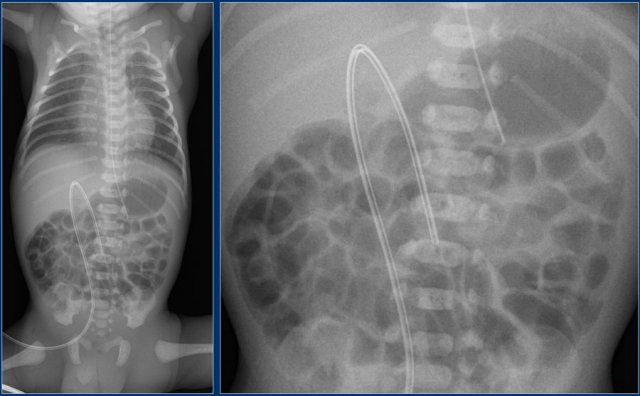
The findings are:
- Malposition of umbilical artery line, folded in the abdominal aorta.
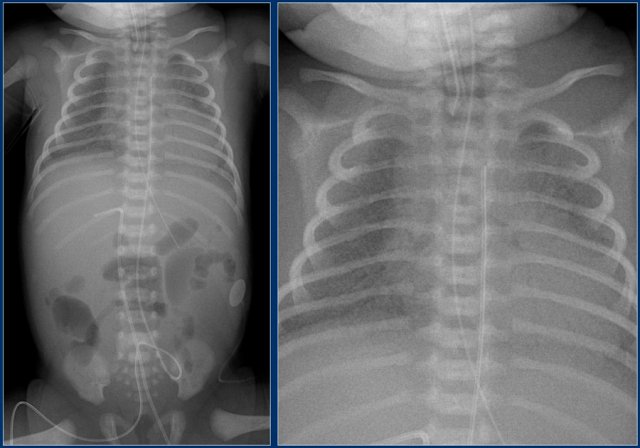
Umbilical artery line (4)
First study the images.
Then continue reading.
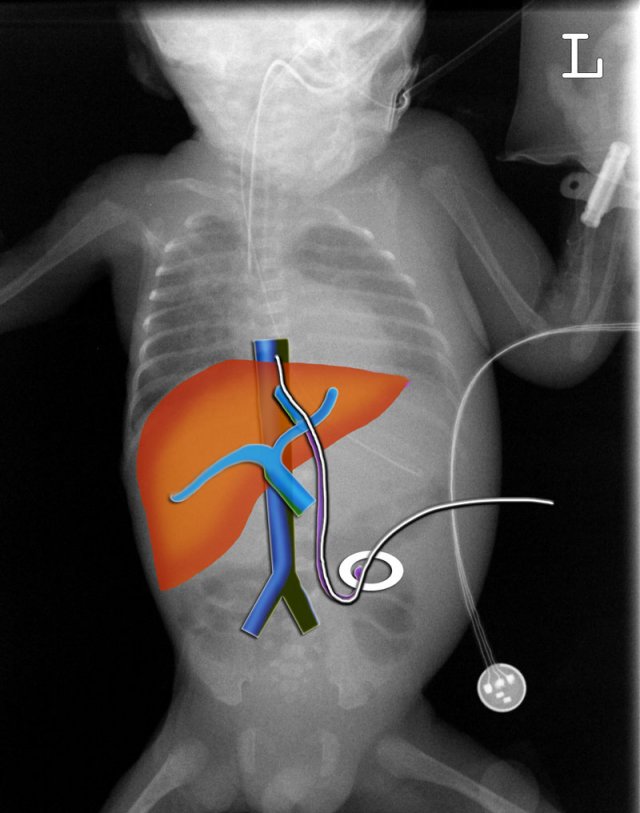
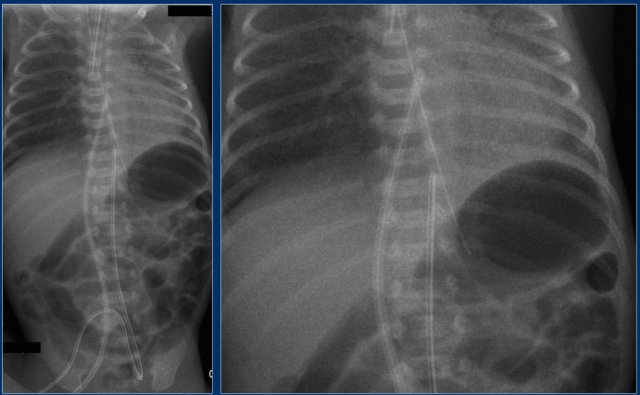
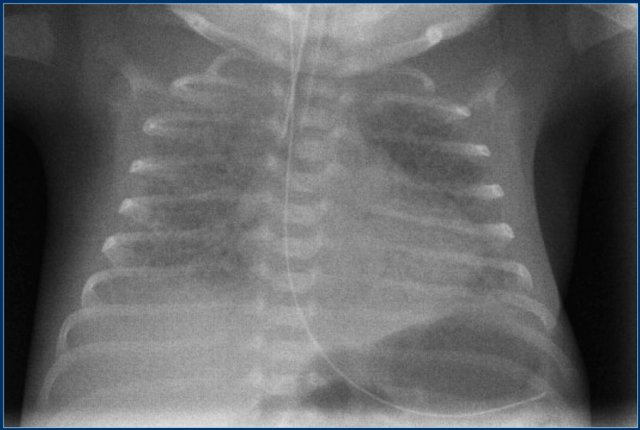
The findings are:
- Deep position of umbilical artery line, in aortic arch.
- Umbilical vein line with tip in right portal vein.
Umbilical artery line (5)
First study the images.
Then continue reading.
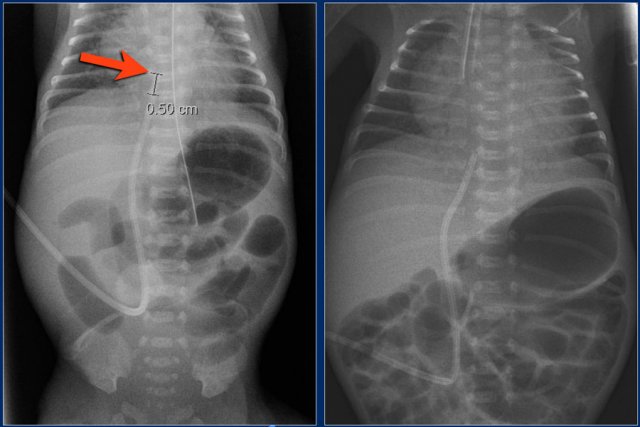
The findings are:
- Malposition of umbilical artery line in left iliac artery.
- Deep position of umbilical vein line in right atrium.
- Good position of gastric tube.
Umbilical vein catheter
An umbilical vein catheter should pass through the umbilic vein into the left portal vein.
Then through the ductus venosus into a hepatic vein and the inferior caval vein (IVC).
The tip should be positioned in the IVC at the level of the diaphragm.
Several line malpositions are possible:
- Low position in the umbilical vein.
Not all medication can be administered through a line in this position. - Intrahepatic into the portal venous system, both right and left, or even into the superior mesenteric or splenic vein.
This can cause thrombosis. - Perforation of the portal vein can cause haemorrhage or abscess formation in the liver.
- Position too deep in right atrium or in the left atrium through a patent foramen ovale or atrial septal defect.
This can lead to cardiac arrhythmias or perforation.
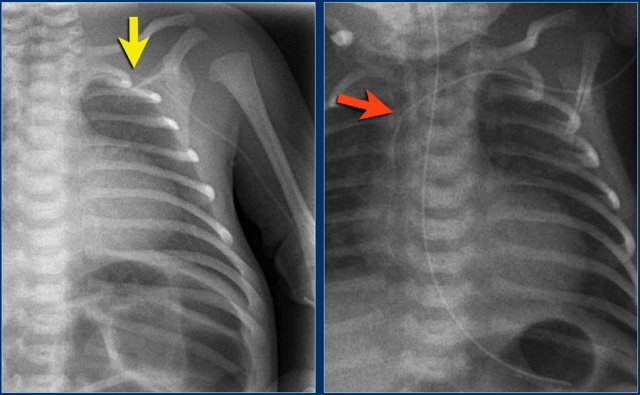
Umbilical venous line (2)
First study the images.
Then continue reading.
The findings are:
- Umbilical vein line positioned in the periphery of the liver through the right portal vein.
- Artery line in the left subclavian artery.
Umbilical venous line (3)
First study the images.
Then continue reading.
The findings are:
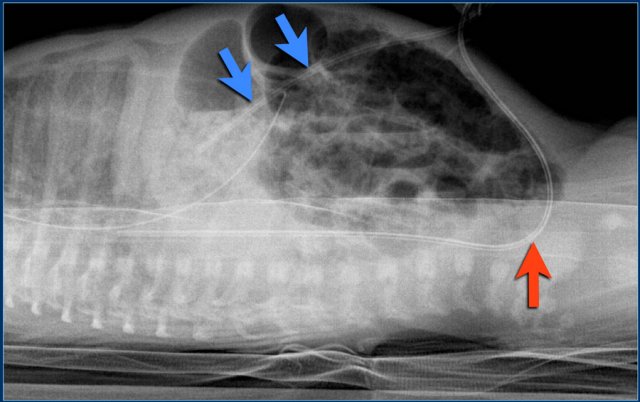
- This is a lateral horizontal beam radiograph.
It illustrates the umbilical vein line following the traject of the umbilical vein into the liver (blue arrow).
The line is not deep enough. - The umbilical arterial line first passes caudally and enters the iliac artery (red arrow).
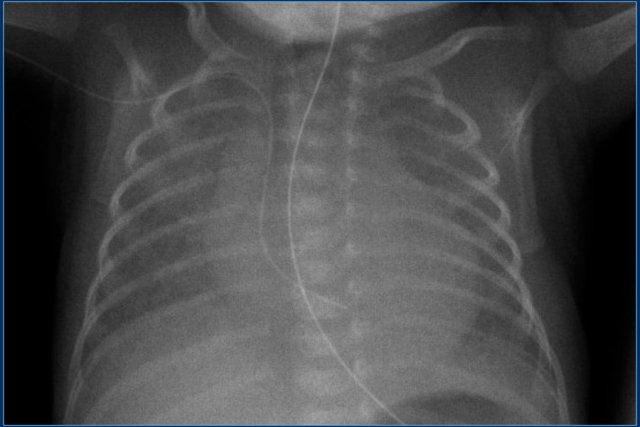
Umbilical venous line (4)
Study the image.
Then continue reading.
The findings are:
- The umbilical vein line is positioned in the umbilical vein and not deep enough.
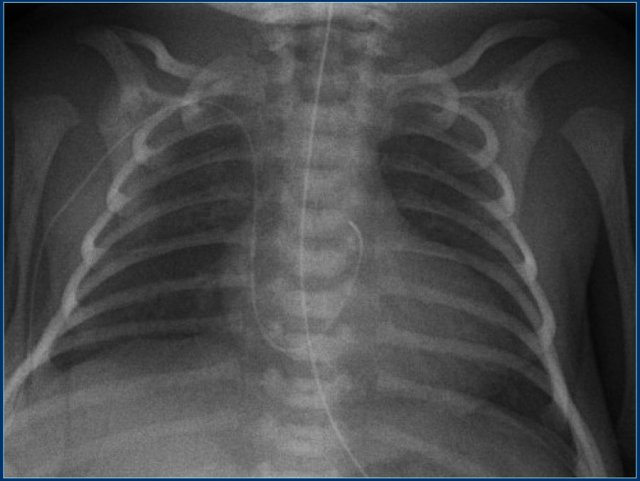
Umbilical venous line (5)
Study the image.
Then continue reading.
The findings are:
- The tip of the umbilical vein line is pointed downwards and probably situated in the mesenterical vein.
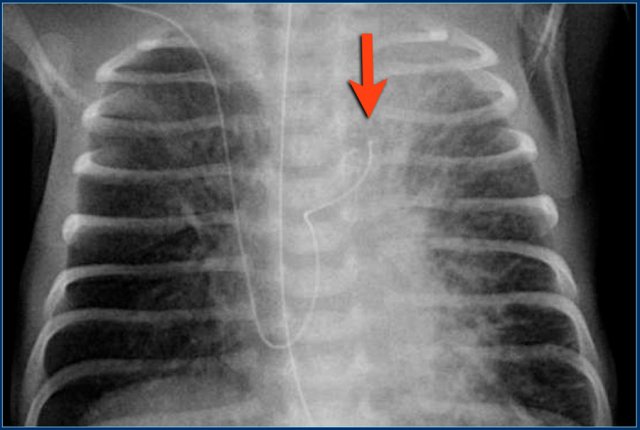
Umbilical venous line (6)
Study the images.
Then continue reading.
The findings are:
- The umbilical venous line is too deep and positioned in the right atrium.
- The umbilical arterial line is at the level of T10 (preferrably at level T6-T9).
- The endotracheal tube is positioned too deep.
It should be 1 cm above the trachea bifurcation.

Umbilical venous line (7 )
Study the images.
Then continue reading.
The findings are:
- The umbilical venous line is too deep.
The line probably went through a patent foramen ovale and through the left atrium into a pulmonary vein.

In this patient ultrasound detected a thrombus in the left portal vein after umbilical venous line (arrows).
Catheter malposition in the left portal vein increases the occurrence of portal venous thrombosis.
Clinically silent portal venous thrombosis is frequently associated with catheterization of the umbilical vein in critically ill neonates, and spontaneous resolution without any treatment is expected in many cases.
Umbilical venous line (8 )
Study the images.
Then continue reading.
The findings are:
- The umbilical venous line is too deep
- After repositioning the tip is in a good position.
Notice that the endotracheal tube is too deep.
Peripherally Inserted Central Catheter
A peripheral inserted central catheter or PICC line is positioned in the great vessels, preferably in the superior or inferior caval vein.
It is important for the neonatologist to know if the line is in a superficial position, because then not all medication can be given.
The left image shows a PICC line, that was placed in the left arm.
It was hard to determine the exact location of the tip.
The lumen of the line was filled with contrast, showing the tip of the line high in the superior caval vein.
It is advised not to use more contrast than the volume of the line, in order to prevent hypothyroidism in reaction to iodine containing contrast, although the risk is low. (16)
PICC line (2)
Study the image.
Then continue reading.
The findings are:
- Malpositioned PICC line in the right atrium.
PICC line (3)
Study the image.
Then continue reading.
The findings are:
- Malpositioned PICC line.
Probably located in the coronary sinus or in the left atrium after passing through a patent foramen ovale.
PICC line (4)
Study the image.
Then continue reading.
The findings are:
- Malpositioned PICC line through a patent foramen ovale into the left atrium and subsequently into a pulmonary vein.
Endotracheal tube
The tip of an endotracheal tube should be inbetween the thoracic aperture and 1 cm above the carina.
The tip travels downward if the neck is flexed or upward if the neck is extended.
The most common malpositioning is in the right mainstem bronchus, because of the shallower angle of the right main bronchus.
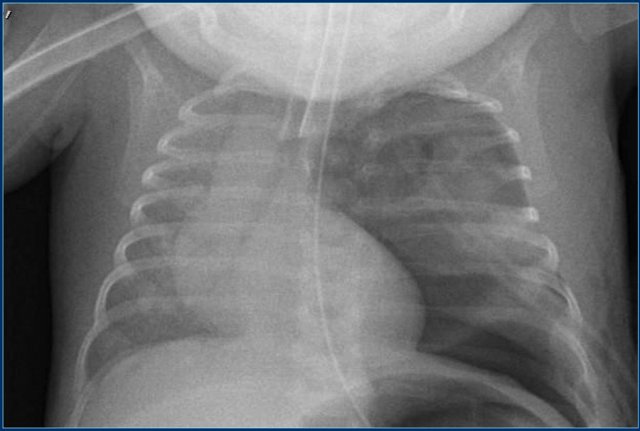
Here a good positioned tube in a patient with a pneumothorax on the left.
Endotracheal tube (2)
Study the image.
Then continue reading.
The findings are:
- Right mainstem bronchus intubation with atelectasis of the entire left lung.
Endotracheal tube (3)
Study the image.
Then continue reading.
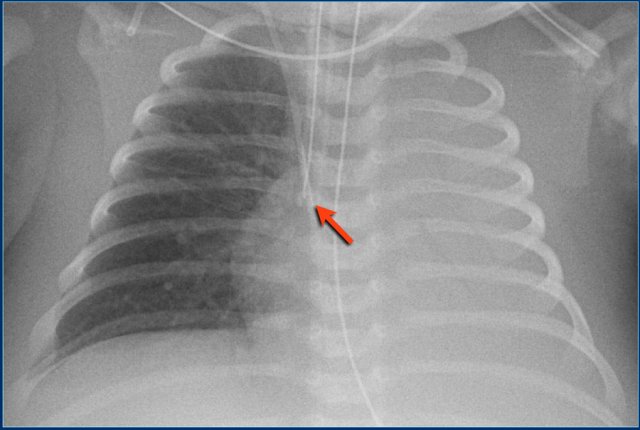
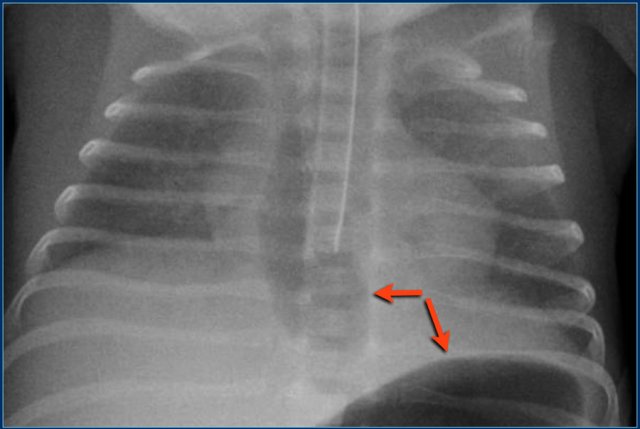
The findings are:
- Endotracheal tube is positioned in the oesophagus.
- Chest radiograph shows dilatation of the esophagus and stomach, that are filled with air (arrows).
Endotracheal tube (4)
Study the image.
Then continue reading.
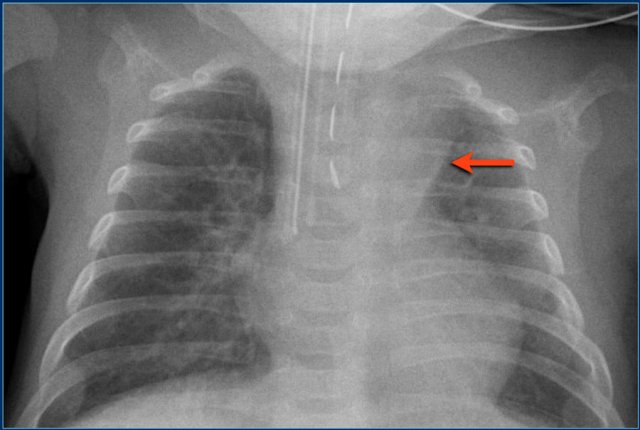
The findings are:
- Endotracheal tube is positioned in the right main bronchus.
- Atelectasis of left upper lobe of the lung.
Chest drainage tube
Chest drainage tube are placed in case of respiratory distress caused by pleural fluid or pneumothorax in order to allow sufficient expansion of the lung for ventilation.
The tube should be positioned in the midaxillary line via the 4th - 6th intercostal space.
The position should be apical anterior in patients with a pneumothorax.
Study the image.
Then continue reading.
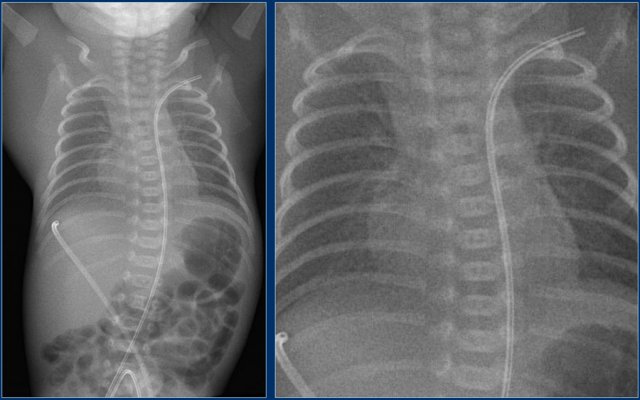
The findings are:
- Endotracheal tube in good position.
- Straight chest drain tube in good position. Drainage however is not optimal.
- Mediastinal shift to the right. There is however no tension-pneumothorax, since the diaphragm has a normal convex upper border.
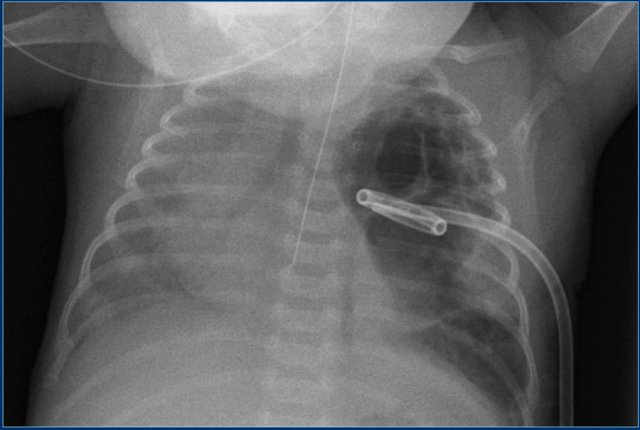
In this patient, who has a large pneumatocele, a pigtail catheter is placed in the pneumatocele.
Complications of chest tubes are:
- Perforation of vessels or pericardium. This may cause hematothorax.
- Subcutaneous or subpleural position.
This will result in an aberrant position of the drain and dysfunction.
Gastric catheters
Gastric catheters should be positioned with the tip in the stomach.
Reploggel's suction catheter
Replogle's suction catheters are used in case of oesophageal atresia to remove saliva.
They are positioned in the blind ending oesophagus.
The markings of a Replogle's suction catheter form a dashed line.
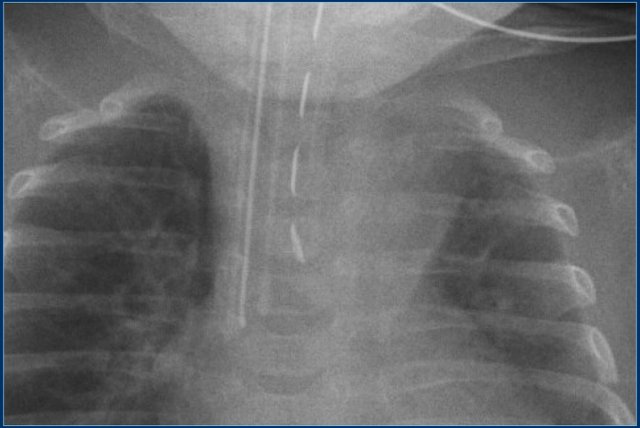
Here a preterm infant with oesophageal atresia with a fistula.
There is a Reploggel's drain in situ.
Notice deep position of endotracheal tube and atelectasis of left upper lobe.
Extracorporeal membrane oxygenation

Extra corporal membrane oxygenation or ECMO is a extracorporeal technique to oxygenate the child when conventional circulatory and respiratory supportfails.
One sheet is placed in the superior caval vein and one in the brachiocephalic artery.