Cervical injury
Adam Flanders
Department of Radiology and Regional Spinal Cord Injury Center of the Delaware Valley, Thomas Jefferson University Hospital, Philadelphia
Publicationdate
This review is based on a presentation given by Adam Flanders and adapted for the Radiology Assistant by Robin Smithuis.
Approximately 3 % of patients who present to the emergency department as the result of a motor vehicle accident or fall have a major injury to the cervical spine.
10-20% patients with head injury also have a cervical spine injury.
Up to 17% of patients have a missed or delayed diagnosis of cervical spine injury, with a risk of permanent neurologic deficit after missed injury of 29%.
Most cervical spine fractures occur predominantly at two levels.
One third of injuries occur at the level of C2, and one half of injuries occur at the level of C6 or C7.
In this overview we will discuss the most common cervical spine injuries.
You can click on some of the images to get a larger image.
Introduction
 Hyperflexion injuriesClick on the image to get a larger view.
Hyperflexion injuriesClick on the image to get a larger view.
Flexion injuries
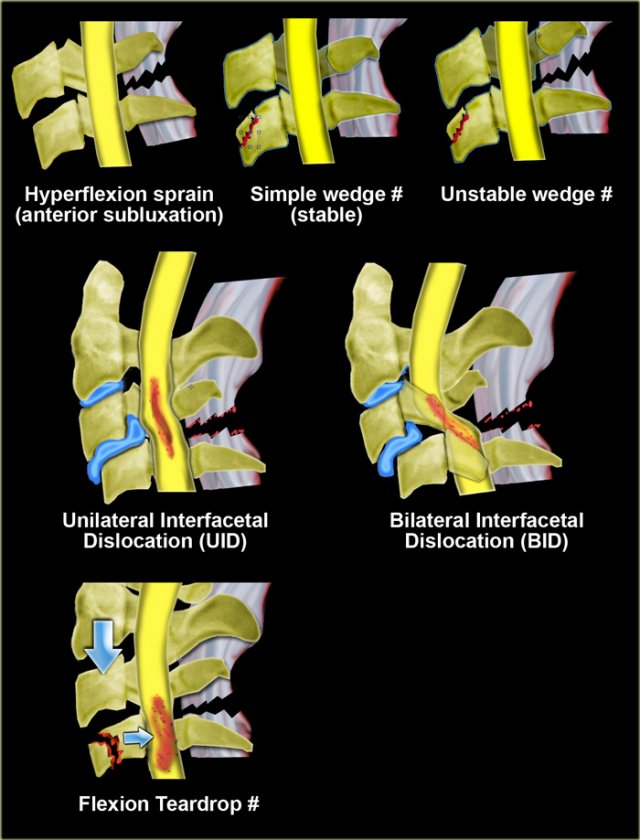
The most common fracture mechanism in cervical injuries is hyperflexion.
- Anterior subluxation occurs when the posterior ligaments rupture.
Since the anterior and middle columns remain intact, this fracture is stable. - Simple wedge fracture is the result of a pure flexion injury. The posterior ligaments remain intact. Anterior wedging of 3mm or more suggests fracture. Increased concavity along with increased density due to bony impaction. Usualy involves the upper endplate.
- Unstable wedge fracture is an unstable flexion injury due to damage to both the anterior column (anterior wedge fracture) as the posterior column (interspinous ligament).
- Unilateral interfacet dislocation is due to both flexion and rotation.
- Bilateral interfacet dislocation is the result of extreme flection. BID is unstable and is associated with a high incidence of cord damage.
- Flexion teardrop farcture is the result of extreme flection with axial loading. It is unstable and is associated with a high incidence of cord damage.
- Anterior atlantoaxial dislocation
 Hyperextension injuries
Hyperextension injuries
Extension injuries
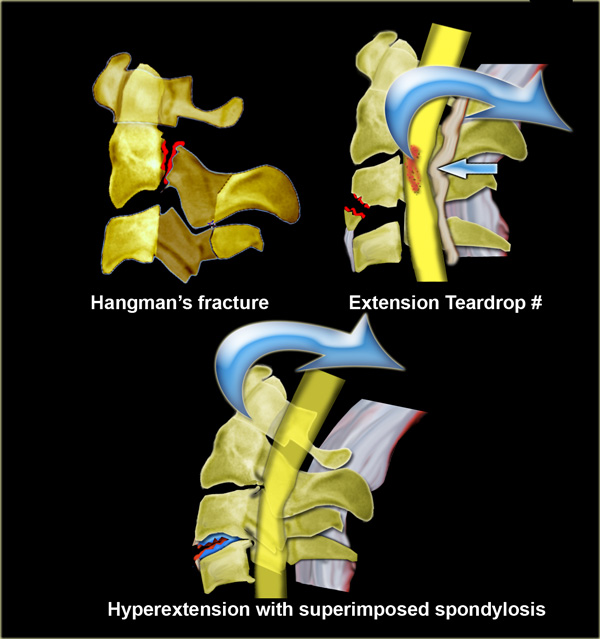
- Hangman's fracture
Traumatic spondylolisthesis of C2. -
Extension teardrop fracture
- Hyperextension in preexisting spondylosis
'Open mouth fracture'.
Axial compression injuries
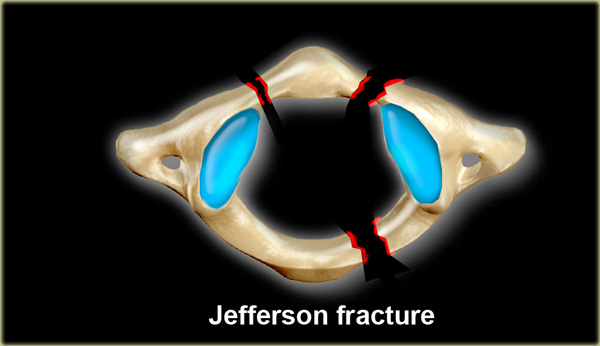
- Jefferson fracture is a burst fracture of the ring of C1 with lateral displacement of both articular masses .
- Burst fracture at lower cervical level
Stability
Unstable fractures:
-
Flexion
- Bilateral interfacetal dislocation
- Flexion teardrop fracture
- Wedge fracture with posterior ligamentous rupture
-
Extension
- Odontoid fracture type II
- Hangman's fracture
- Extension teardrop fracture
-
Vertical compression
- Burst fracture, e.g. Jefferson fracture
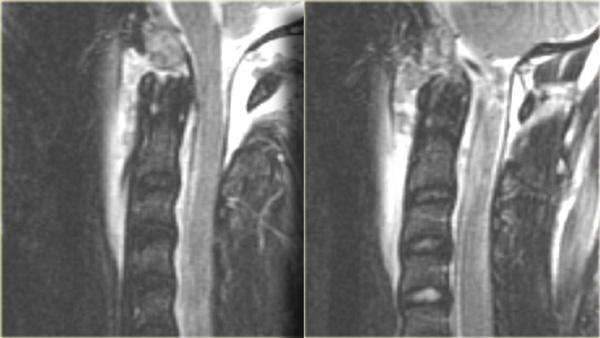
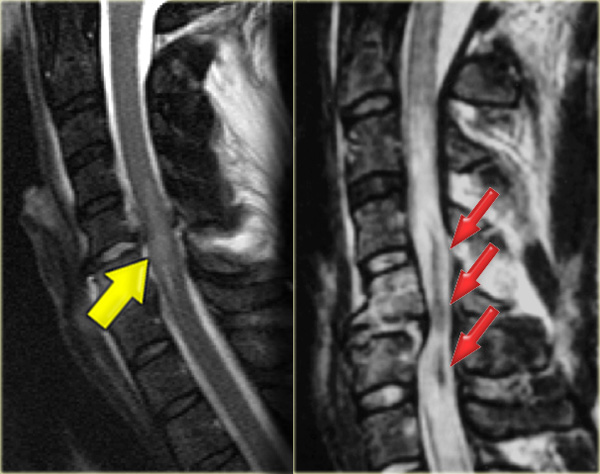 Non-hemorrhagic and hemorrhagic spinal cord injury
Non-hemorrhagic and hemorrhagic spinal cord injury
Spinal cord injury
There are two types of injury to the spinal cord:
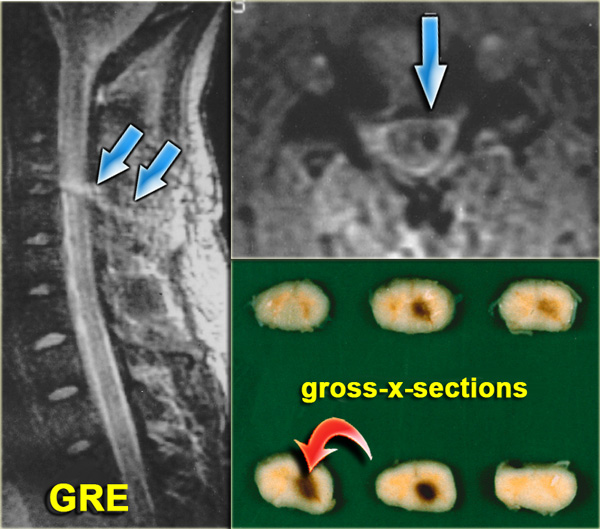
- Non-hemorrhagic with only high signal on MR due to edema.
- Hemorrhagic with areas of low signal intensity within the area of edema.
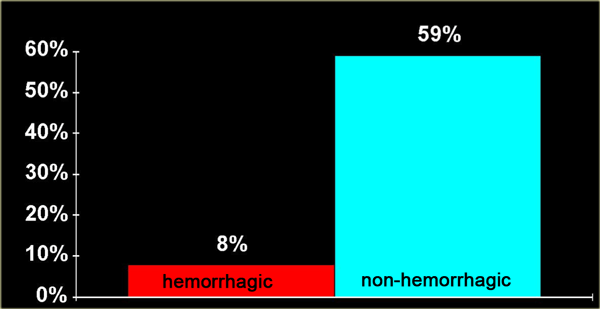 Effect of spinal cord hemorrhage on motor recovery of the legs at 12 months
Effect of spinal cord hemorrhage on motor recovery of the legs at 12 months
There is a strong correlation between the length of the spinal cord edema and the clinical outcome.
The most important factor however is whether there is hemorrhage, since hemorrhagic spinal cord injury has an extremely poor outcome.
The chart on the left is showing the motor recovery rate for patients with edema alone (in blue) versus edema plus cord hemorrhage (in red).
The motor recovery rate is for the legs only.
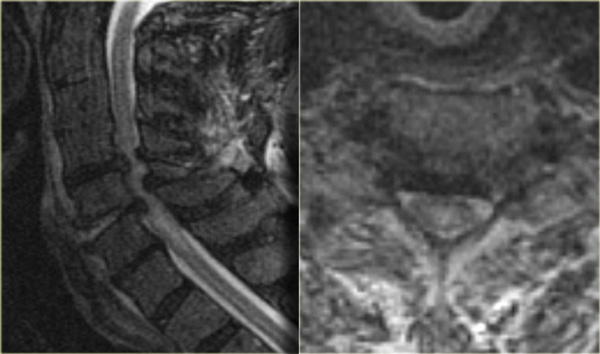 Central spinal cord injury in a patient with a hyperextension injury and preexisting spondylosis and stenosis.
Central spinal cord injury in a patient with a hyperextension injury and preexisting spondylosis and stenosis.
Spinal cord syndromes (2):
-
Central cord syndrome
- Most common incomplete cord syndrome.
- Frequently found in elderly with underlying spondylosis or younger people with severe extension injury (figure).
- Upper extremity deficit is greater than lower extremity deficit, because the lower extremity corticospinal tracts are located lateral in the cord.
-
Anterior cord syndrome
- Seen in flexion injuries e.g. burst fracture, flexion tear drop fracture and herniated disk.
- Presents with immediate paralysis, because the corticospinal tracts are located in the anterior aspect of the spinal cord.
-
Brown-Sequard syndrome
- Ipsilateral motor weakness and contralateral sensory deficit due to hemisection of the spinal cord.
- Brown-Sequard syndrome may result from rotational injury such as fracture-dislocation or from penetrating trauma such as stab wound.
-
Posterior cord syndrome
- Uncommon syndrome due to extension injury.
- Loss of positioning sense due to disruption of dorsal columns.
- Good prognosis.
-
Complete spinal cord injury
- Total absence of sensation and motor function caudal to the level of injury.
 Brown-Sequard Syndrome after stab wound with screwdriver
Brown-Sequard Syndrome after stab wound with screwdriver
On the left images of spinal cord injury after a stab wound with a screwdriver.
This resulted in a Brown-Sequard syndrome due to hemisection of the spinal cord.
Hyperflexion injuries
 Hyperflexion sprain without fracture
Hyperflexion sprain without fracture
Hyperflexion Sprain
Hyperflexion sprain injuries are injuries to the soft tissues of the spine without fracture.
On x-rays this can only be suspected when there is angulation or translation
MR will demonstrate subtle injuries to the soft tissues.
On the left images of a patient who has been in a car accident and complained of neck pain.
The x-rays were normal and there were no neurological symptoms.
First study the images on the left.
Then continue reading.
The findings are:
- Edema in the posterior soft tissues indicating a hyperflexion injury
- Edema in the vertebrae of the lower C-spine and upper T-spine indicating bone bruise as a result of axial loading.
In this patient we can conclude that there was mild hyperflexion strain and we do not know if a special treatment is required, since these were isolated MR-findings without evidence of fracture or abnormal positioning.
There is controversy regarding the meaning of soft tissue abnormalities detected only on MRI.
Signal changes do not necessarily equate with structural failure.
These findings still require better validation.
In trauma centres up to 25% of all patients with neck injury have signal abnormalities on MR and the significance is indeterminate.
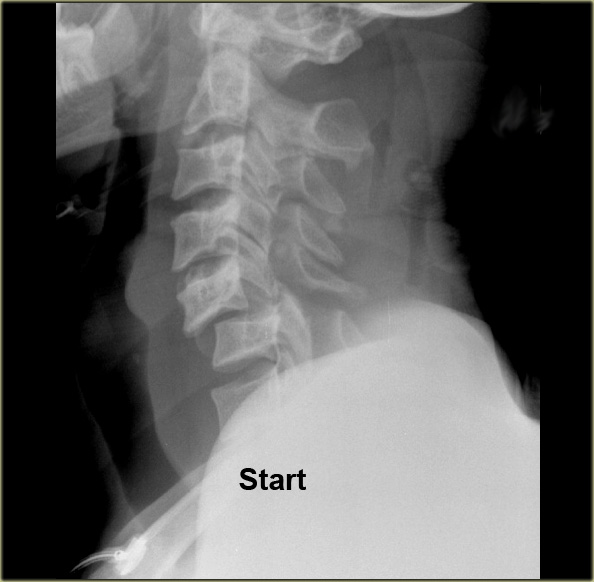
 Hyperflexion sprain
Hyperflexion sprain
Hyperflexion sprain (2)
On the left images of a 44 year old female, who sustained a fall on the ice.
She subsequently had a second fall the following morning, where after she had complete loss of motor and sensation.
On physical examination there was lower extremity paraparesis with some upper extremity weakness on the right.
Central cord injury was proposed initially.
The radiographs were normal.
First study the images on the left.
Then continue reading.
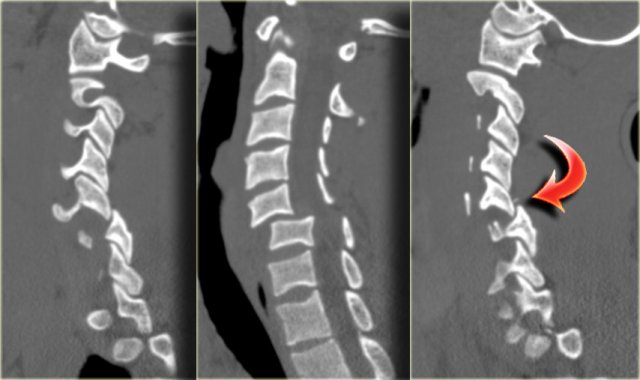
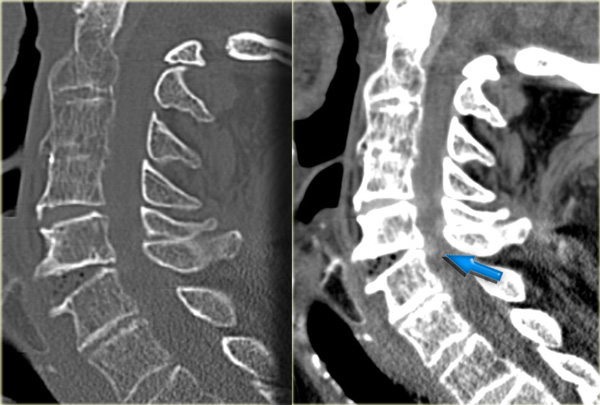
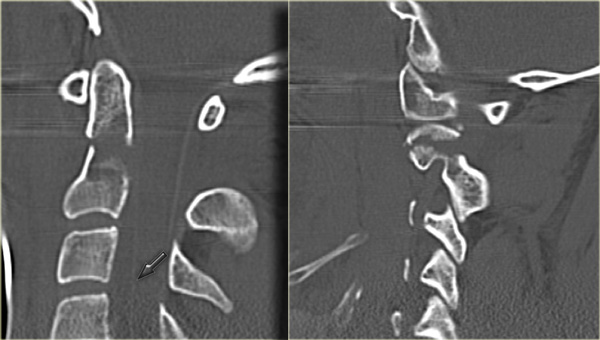
The findings are:
- Small bone fragmets comming off the superior and inferior facets
- Widened interspinous space at C5-6
- Soft tissue swelling at this level posteriorly
- Subtle narrowing of the disc space at the C5-6-level.
These CT-findings are very subtle and do not seem to match the neurological problem.
In such a case MRI is the next step.
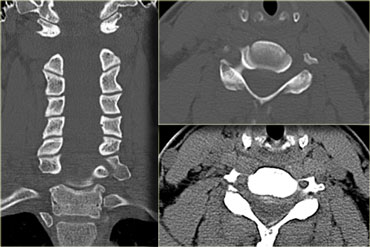
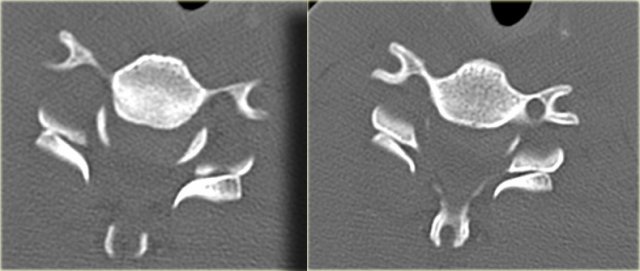
First we show you a coronal and axial CT with also a soft tissue window-setting.
There is high density material at the back of the disc space, which is very suggestive for a traumatic disc herniation.
A epidural hematoma should be in the differential, but this finding was limited to just the area of the disc space, unlike a hematoma.
Continue with the MR.
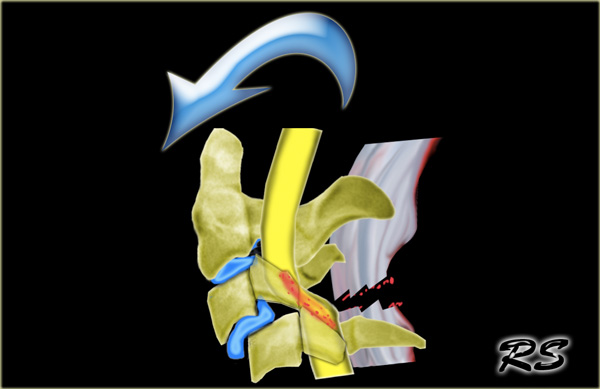
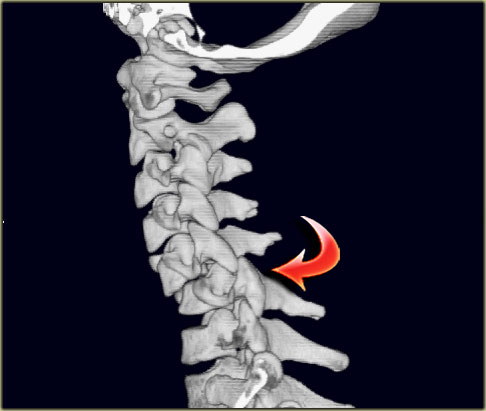
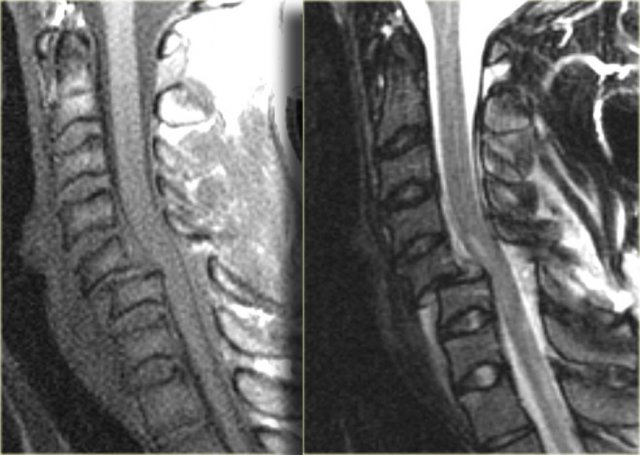
 Hyperflexion sprain with spinal cord injury
Hyperflexion sprain with spinal cord injury
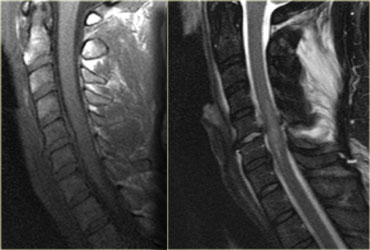
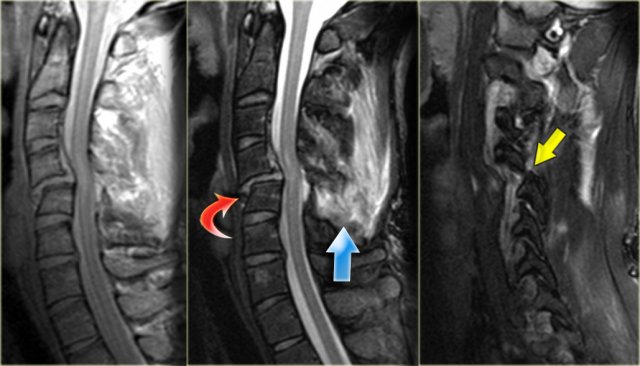
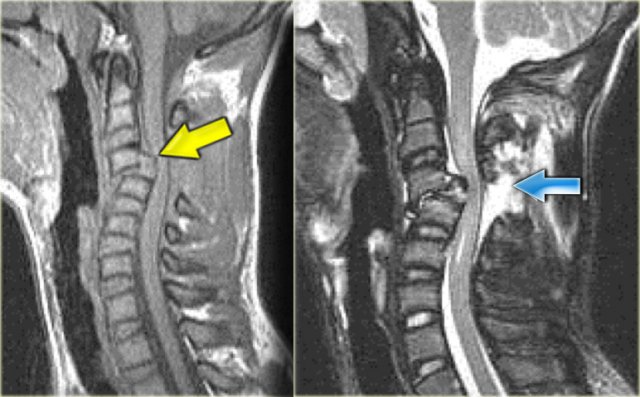
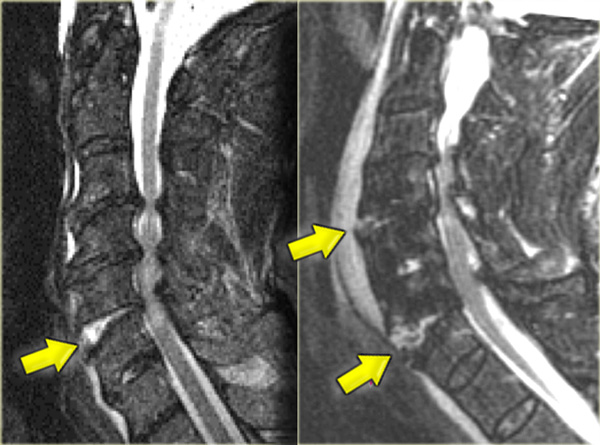
Hyperflexion sprain (3)
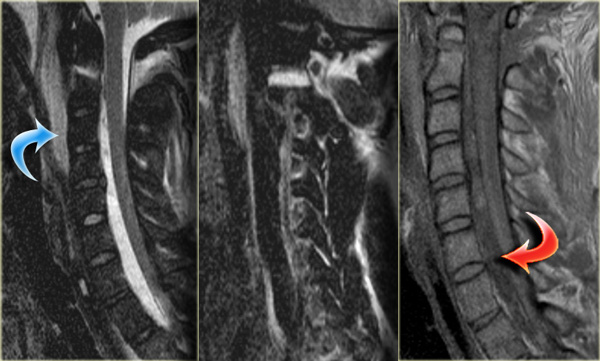
The MRI explains the neurological status of this patient.
First study the images on the left.
Then continue reading.
The MR-findings are:
- Severe soft tissue injury of the posterior paraspinal structures, especially at the C5-6 level, where the interspinous ligament and the ligamentum flavum is ruptured
- Disruption of the C5-6 disc with migration behind C5
- Large amount of spinal cord edema
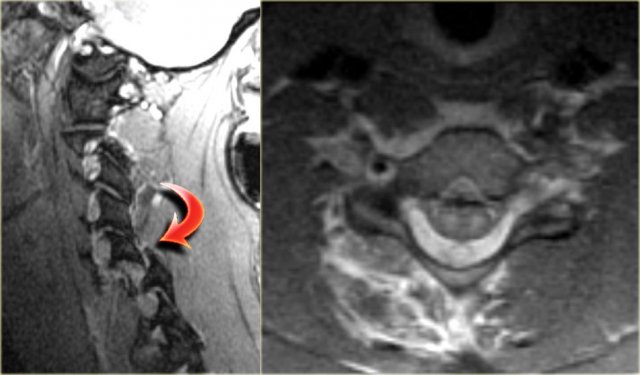
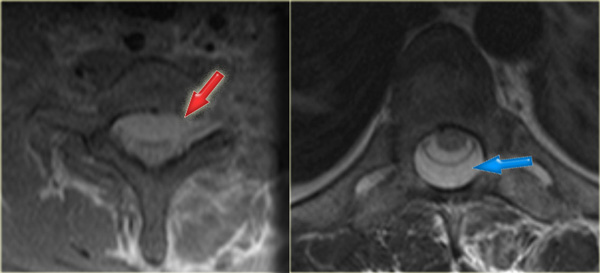
Continue with the axial image.
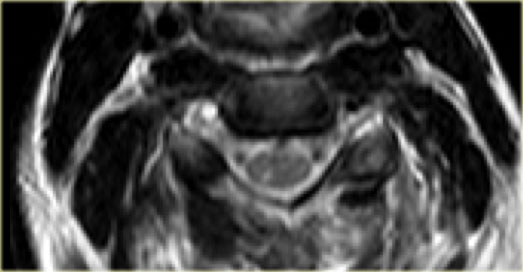 Vertebral artery thrombosis: no flow void in the right vertebral artery
Vertebral artery thrombosis: no flow void in the right vertebral artery
The axial image shows the spinal cord injury and in addition to it there is absence of flow void in the right vertebral artery.
This indicates thrombosis as a result of dissection.
In conclusion we can say that this patient had no fracture, but a severe hyperflexion sprain with acute disc herniation, non-hemorrhagic spinal cord injury and vertebral thrombosis.
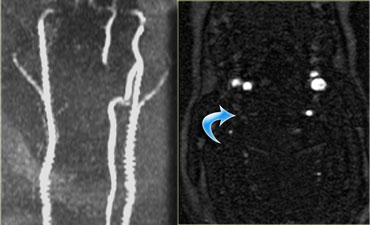 Right vertebral artery thrombosis
Right vertebral artery thrombosis
The MRA confirms the occlusion of the right vertebral artery.
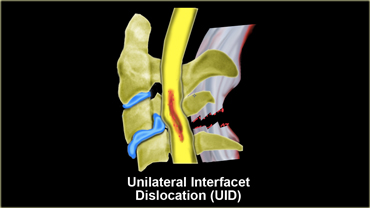
Unilateral interfacet dislocation
Unilateral interfacet dislocation is due to a hyperflexion injury with rotation.
The superior facet on one side slides over the inferior facet and becomes locked.
This results in an anterior subluxation of the upper vertebral body of about 25% of the AP diameter of the body.
Simple unilateral facet dislocation is a stable injury.
30% of patients have an associated neurologic defect.
MRI plays an important role in the diagnosis in order to see if there is disc extrusion leading to cord compression.
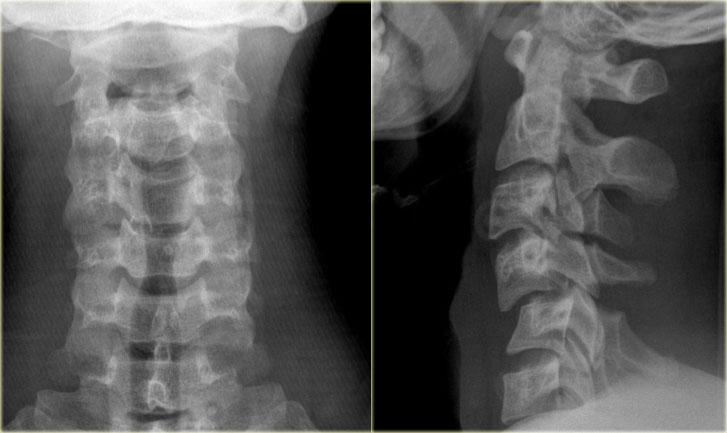
On the left images of a 20 year old male who had a rollover motor vehicle accident.
First study the images on the left.
Then continue reading.
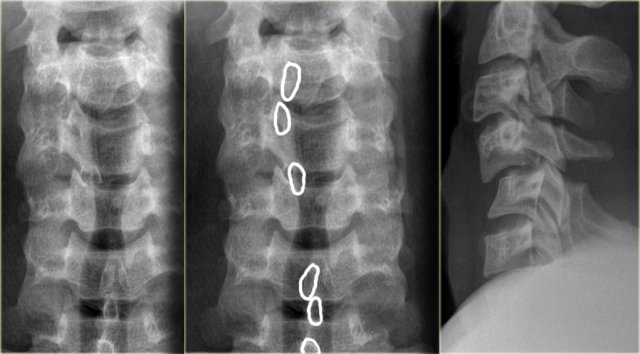
The radiographic findings are:
- Hyperflexion at the level of C4C5 with widening of the interspinous space
- Subluxation at the level of C4C5 with about 25% translation (i.e. anteroposition of 25% of the AP diameter of the vertebral body)
- Malalignment of the spinous processes as seen on the AP-view, which can only be produced by a rotatory injury. The involved spinous process points to the involved side
- Due to the rotation the spinous processes of C4 and C5 seem shorter on the lateral view

The CT confirms the unilateral dislocation.
The contralateral facetjoint is only distracted.
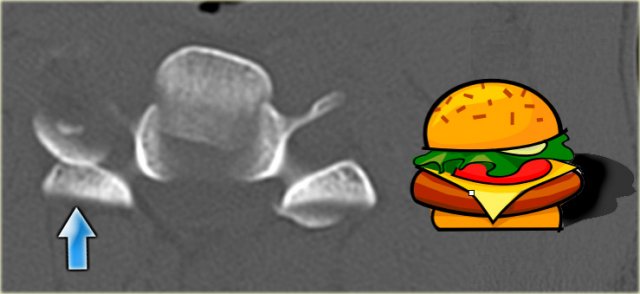 Inverted hamburger sign in unilateral interfacetal dislocation
Inverted hamburger sign in unilateral interfacetal dislocation
Unilateral interfacetal dislocation (2)
On the axial view the left facet joint is normal and the configuration has similarities with the hamburger.
On the right side the classic 'inverted hamburger sign' is seen.
Continue with the MR-images
 Unilateral interfacetal dislocation
Unilateral interfacetal dislocation
First study the MR-images.
Then continue reading.
The MRI-findings are:
- Spinal cord lesion, which can be described as contusion, edema or non-hemorrhagic spinal cord injury.
- Rupture of the spinous ligaments.
- Rupture of the ligamentum flavum.
-
Rupture of the disc with migration of disc material on the posterior side of C4 and even on the anterior side of C5.
The disc space is always disrupted in this kind of injury due to the extreme rotation.
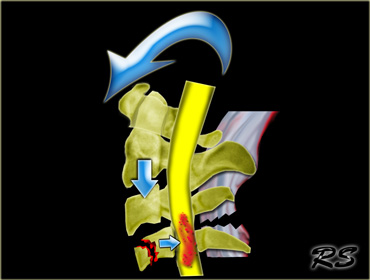
Bilateral Interfacetal Dislocation
Bilateral interfacetal dislocation (BID) is the result of extreme hyperflection.
There is anterior dislocation of the articular masses with disruption of the posterior ligament complex, posterior longitudinal ligament, the disc and usually also the anterior longitudinal ligament.
When the dislocation is complete, the dislocated vertebra is anteriorly displaced one-half of the AP diameter of the vertebral body.
Because of its extensive soft tissue damage and dislocated facet joints, BID is unstable and is associated with a high incidence of cord damage.
 Bilateral interfacetal dislocation
Bilateral interfacetal dislocation
First study the images on the left.
Then continue reading.
The findings are:
- Bilateral interfacetal dislocation.
-
50% anteroposition C5C6 as a result of the dislocation.
In unilateral dislocation the anteroposition is usually only 25%. - Widened space between spinous processes C5 and C6 due to ligament rupture.
- Ruptured disc space.
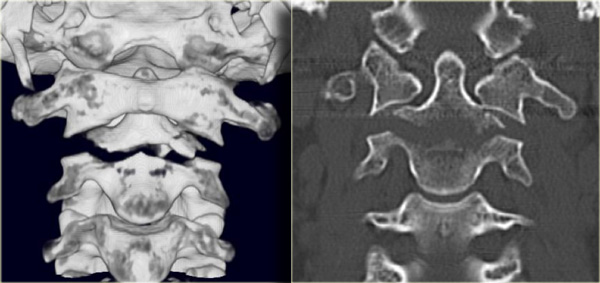
On the left CT-images of the same patient, which confirm the bilateral dislocation.
Near one of the facets there is a small fleck of bone, but there is no major fracture, so this is basically just a hyperflexion soft tissue injury.
 Double inverted hamburger sign in bilateral facetal dislocation
Double inverted hamburger sign in bilateral facetal dislocation
On the axial images the inverted hamburger sign is seen on both sides.
Bilateral interfacetal dislocation (2)
On the left you can scroll through the 3D-reconstructions.
Bilateral interfacetal dislocation (3)
First study the MR-images for additional findings.
Then continue reading.
The MRI-findings are:
- Soft tissue swelling anteriorly
- Disruption of the disc
- Non-hemorrhagic cord injury
Continue with the axial image.
Notice on the axial image that the cord injury is located in the grey matter, which is more sensitive to damage.
--> Reduction under fluoroscopy
In order to regain normal alignment, progressive weights are used to lengthen the spine until reduction is achieved.
Scroll through the images on the left.
Notice, that with 60 pounds the facets start to move, but it finally takes about 110 pounds before the neck is reduced.
Because someone is holding on to the neck while more weight is added, an actual 'clunk' can be felt in the neck indicating that reduction is achieved.
Continue with the MR-images after reduction.
Bilateral interfacetal dislocation (5)
On the left images of a 15-year old, who was injuried during wrestling.
There is 50% anteroposition of C3 on C4 as a result of bilateral interfacetal dislocation.
There is complete disruption of the posterior complex.
This boy had severe neurologic deficit.

Bilateral interfacetal dislocation (6)
On the left another bilateral interfacetal dislocation with complete transsection of the cord.
This is a very uncommon finding, since the spinal cord is very plastic.
 Flexion tear drop fracture
Flexion tear drop fracture
Flexion tear drop fracture
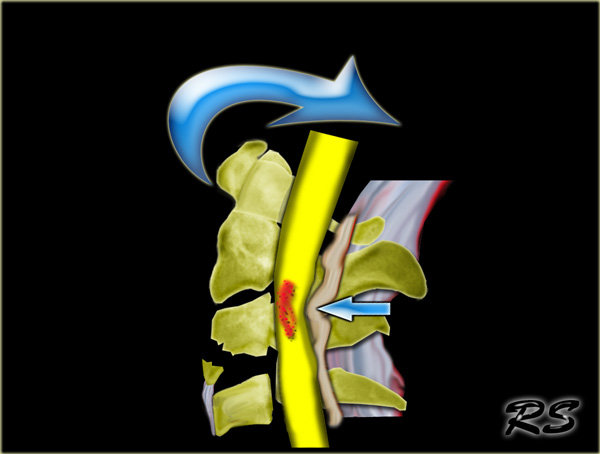
This fracture is the result of a combination of flexion and compression,
which is usually the result of a motor vehicle accident.
The teardrop fragment comes from the anteroinferior aspect of the vertebral body.
The larger posterior part of the vertebral body is displaced backward into the spinal canal.
On x-rays the facet joints and interspinous distances are usually widened and the disk space may be narrowed.
70% of patients have neurologic deficit.
It is an unstable fracture associated with complete disruption of ligaments and anterior cord syndrome.
 Flexion tear drop fracture due to diving injury
Flexion tear drop fracture due to diving injury
On the left images of a 21 year old male who sustained a diving injury, striking his head in a swimming pool.
He had immediate onset of upper and lower extremity weakness.
First study the images.
Then continue reading.
The findings are:
- Fracture of the body of C5 with a small fragment anteriorly
- Fracture of the spinous processus of C4
- Acute angulation at the level of C5C6 with displacement of C5 in posterior direction
Some would just call this a severe hyperflexion injury, but this entity is better known as a 'flexion tear drop' fracture.
Look for additional findings on the CT-images and then continue reading.
The findings are:
- Abnormal positioning of some of the facet joints due to distraction but no dislocation
- Additional fracture of the body of C4
-
The vertical orientation of the fractures of the bodies of C4 and C5 indicate that there was severe axial loading.
In fact these vertebral bodies kind of 'exploded' with propulsion of a bone fragment anteriorly (teardrop) and the larger part posteriorly against the spinal cord.
Continue with the MR-images.
Flexion tear drop fracture (2)
Look for additional findings on the MR-images and then continue reading.
The findings are:
- Sof tissue injuries anteriorly and posteriorly with flavum and interspinous ligament rupture and CSF leakage.
- Hemorrhagic spinal cord injury!
Flexion tear drop fracture (3)
On the left images of a similar case.
There is a C5 flexion teardrop fracture.
Notice that the lower cervical area is not visualised well and additional imaging is required.

The CT-images demonstrate the extreme axial loading.
The tear drop fragment is displaced anteriorly and the larger part of the vertebral body is displaced posteriorly compressing the spinal cord.
Continue with the MR-images.
 T1W- and T2W-images with fatsat.
T1W- and T2W-images with fatsat.
The MR-images demonstrate the spinal injury.
It is a hemorrhagic injury, which has a poor outcome.
Also notice the posterior ligamentous injury as a result of the hyperflexion with rupture of the ligamentum flavum and CSF leakage.
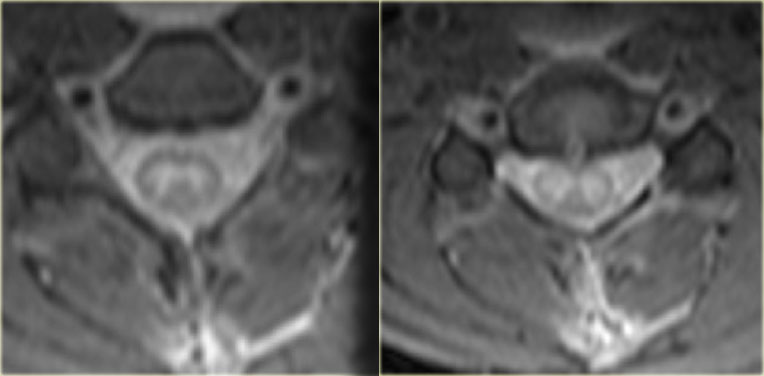 Central spinal cord injury
Central spinal cord injury
Notice the central location of the spinal cord injury.
Hyperextension injuries
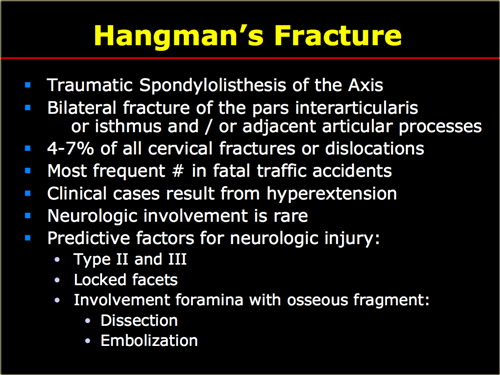
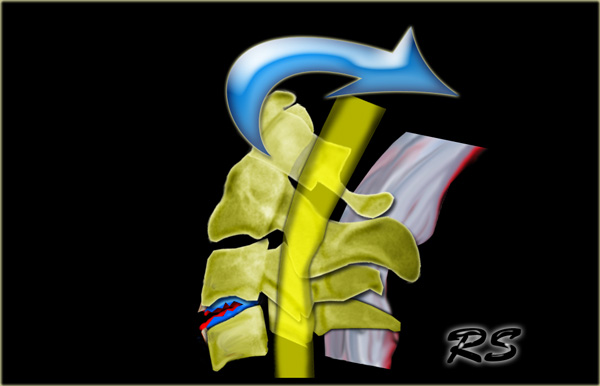
Hangman' s fracture
The Hangman' s fracture is the most common cervical spine fracture.
Classically it is an extension-fracture as the hangman puts the knot under the chin to produce maximal extension-force.
That is why we discuss the hangman' s fracture in the chapter on hyperextension injuries.
In some situations however it can also be the result of extreme flexion.
The hangman's fracture is common in diving accidents.
Although considered an unstable fracture, it seldom is associated with spinal injury, since the anteroposterior diameter of the spinal canal is greatest at this level, and the fractured pedicles allow decompression.
When associated with unilateral or bilateral facet dislocation at the level of C2, this type of hangman's fracture is unstable and has a high rate of neurologic complications.
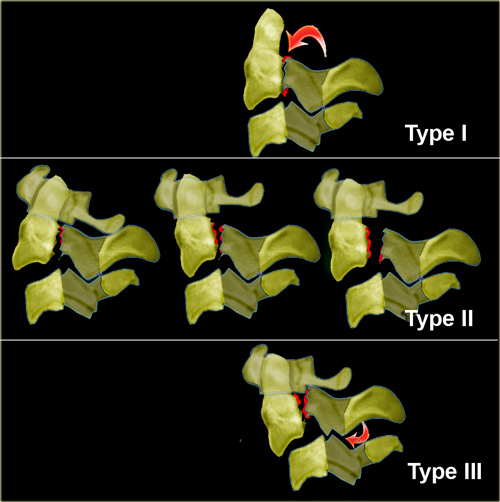
Classification of Hangman' s fractures
- Type I (65%)
- hair-line fracture
- C2-3 disc normal
- Type II (28%)
- displaced C2
- disrupted C2-3 disc
- ligamentous rupture with instability
- C3 anterosuperior compression fracture
- Type III (7%)
- displaced C2
- C2-3 Bilateral interfacet dislocation
- Severe instability
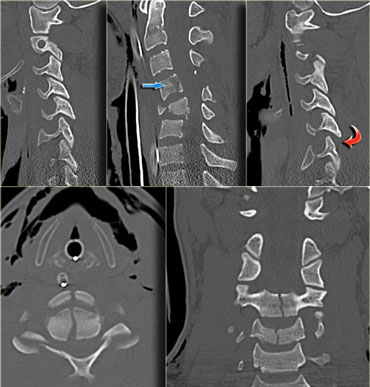
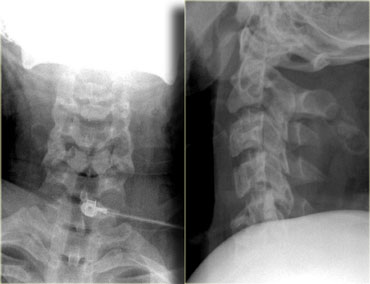
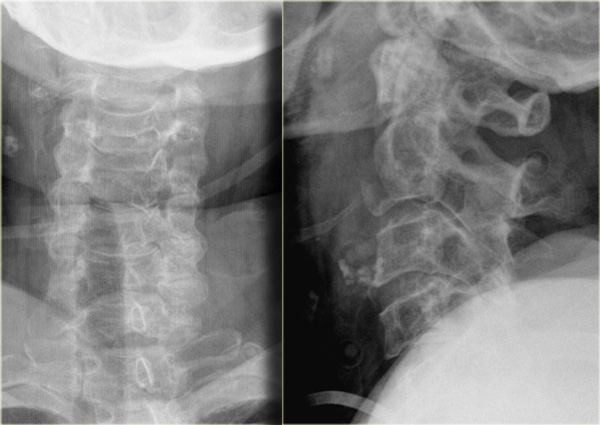
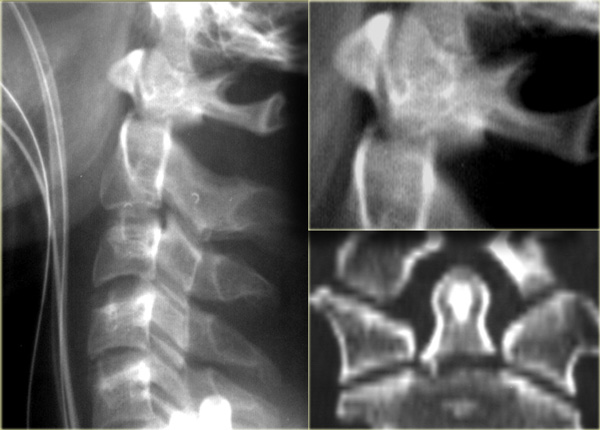
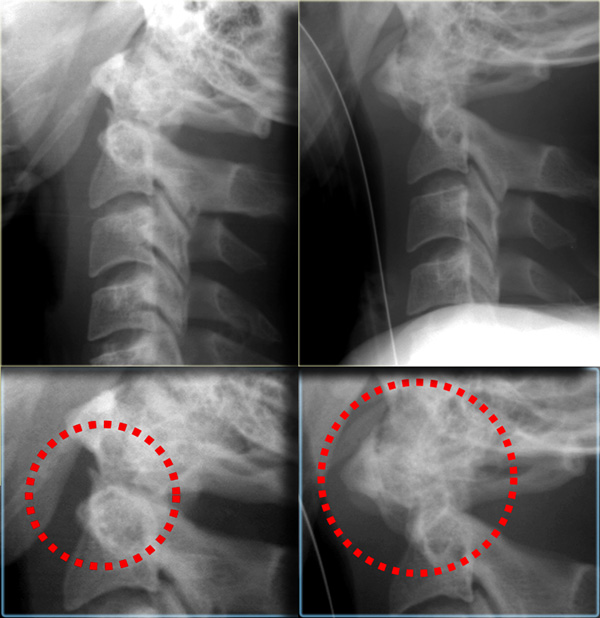
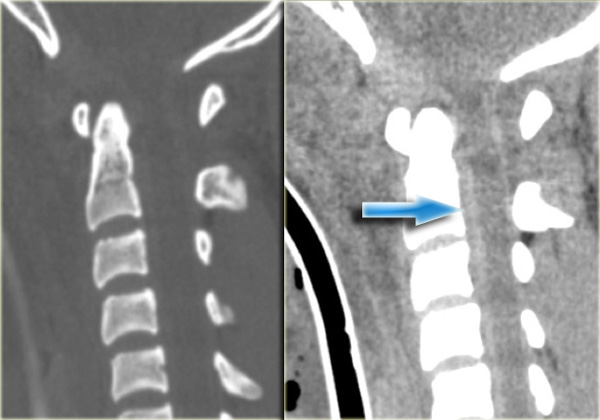
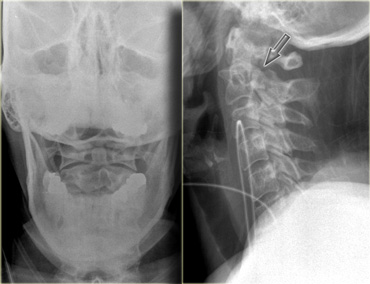 Hangman' s fracture type I
Hangman' s fracture type I
On the left images of a restrained passenger in a vehicle going about 55 miles per hour .
She ran into a tree at about 9 p.m. the previous night with questionable loss of consciousness.
She had cervical tenderness to palpation, but was alert and had no neurologic abnormalities on examination.
First study the images on the left.
Then continue reading.
The findings are:
- Subtle lucent line at the back of the corpus of C2 as seen on the lateral view (arrow).
- Subtle discontinuity of the arch of C2
Continue with the CT-images.
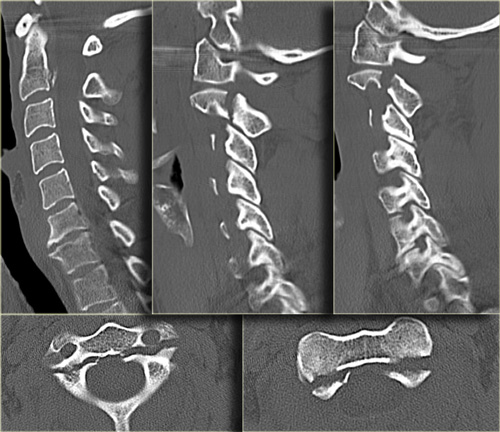
The CT-images confirm the fracture-lines of the hangman's fracture.
They run through the pars interarticularis resulting in a traumatic spondylolysis.
In this case there was no neurologic deficit, because the spinal canal is widened at the level of the fracture.
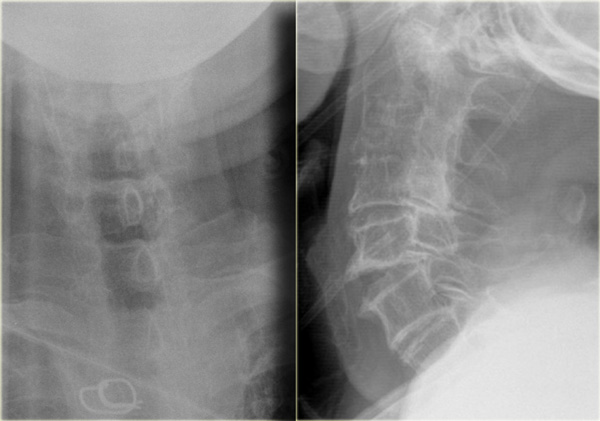
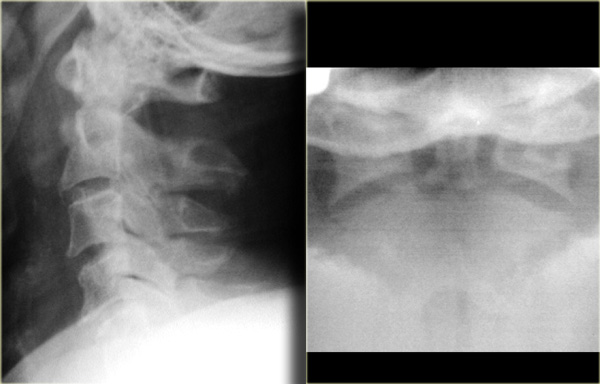
 Hangman' s fracture type I
Hangman' s fracture type I
On the left images of another patient with a type I Hangman' s fracture.
There is a hair-line fracture and there is no displacement.
Hyperextension with superimposed spondylosis
On the left images of a 90-year-old male who tripped and fell on his back and the back of his head.
He had immediate quadriparesis after the event with no loss of consciousness.
First study the images on the left.
Then continue reading.
The findings are:
- Widening of the disc space C5C6 in the front and narrowing in the back.
- This is also called 'an open book'.
- It tells us that there was a hyperextension injury.
Continue with the CT-images.
On CT we also see that there has been a hyperextension injury.
The small black dots in the disc space are the result of a vacuum phenomena.
The negative pressure resulted in a vacuum phenomena in the injured disc space.
There is also some hyperdensity at the back of C5C6, which could be a herniated disc or just preexisting disc degeneration.
In such a patient with spondylosis which has led to narrowing of the canal, a low velocity injury can lead to spinal cord injury.
Continue with the MR-images.
The MR shows a subtle increase in signal intensity of the spinal cord.
Most of the time these patiets get a central cord injury.
There is only injury to the central part of the cord and these patients have disproportioned weakness of their arms and normal strength in their legs.
These injuries can be devastating, although it is uncommon that they are hemorrhagic.
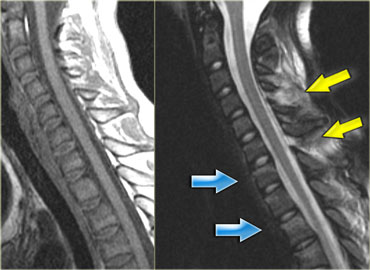
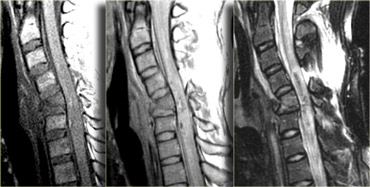
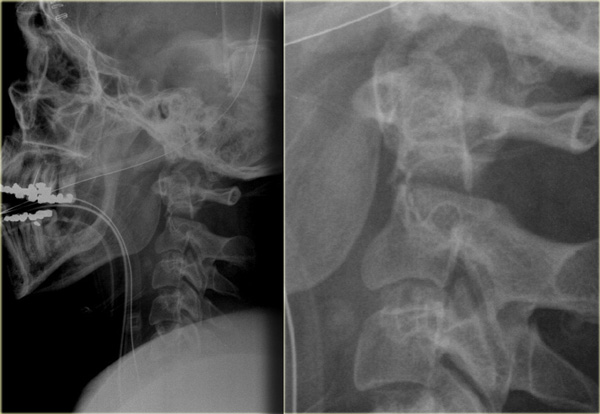
 Hyperextension with superimposed spondylosis
Hyperextension with superimposed spondylosis
Hyperextension injury (3)
On the left two other examples of this hyperextension injury.
It is easy to find the injured disc, since it is the one with the high signal (arrows).
Notice the prevertebral soft tissue swelling in the case on the right.
Extension teardrop fracture
As with flexion teardrop fracture, extension teardrop fracture also manifests with a displaced anteroinferior bony fragment (6).
This fracture occurs when the anterior longitudinal ligament pulls a bony fragment away from the inferior aspect of the vertebra because of the sudden hyperextension.
The fragment is a true avulsion, in contrast to the flexion teardrop fracture in which the fragment is produced by compression.
This type of fracture is commonly seen in diving accidents and tends to occur at lower cervical levels.
It also may be associated with the central cord syndrome due to buckling of the ligamenta flava into spinal canal during the hyperextension phase of injury.
This injury is stable in flexion but highly unstable in extension.
On the left images of a 70 year old female who fell down ten steps striking her head resulting in a subgaleal hematoma with possible loss of consciousness.
There was no neurologic deficit.
Notice the anteroinferior bony fragment of C2.
Continue with the CT images.

The CT confirms the displaced anteroinferior bony fragment.
This fragment is a true avulsion, in contrast to the flexion teardrop fracture in which the fragment is produced by compression of the anterior vertebral aspect due to hyperflexion.
Continue with the MR images.
The MR also confirms that this is not a flexion injury, since the soft tissue injury is located anteriorly.
Extension-teardrop fracture (2)
On the left another extension-teardrop fracture of C2.
Fractures due to axial loading
Jefferson fracture
This fracture is caused by a compressive downward force that is transmitted evenly through the occipital condyles to the superior articular surfaces of the lateral masses of C1.
This process displaces the masses laterally and causes fractures of the anterior and posterior arches, along with possible disruption of the transverse ligament.
Radiographically the fracture is characterized by bilateral lateral displacement of the articular masses of C1.
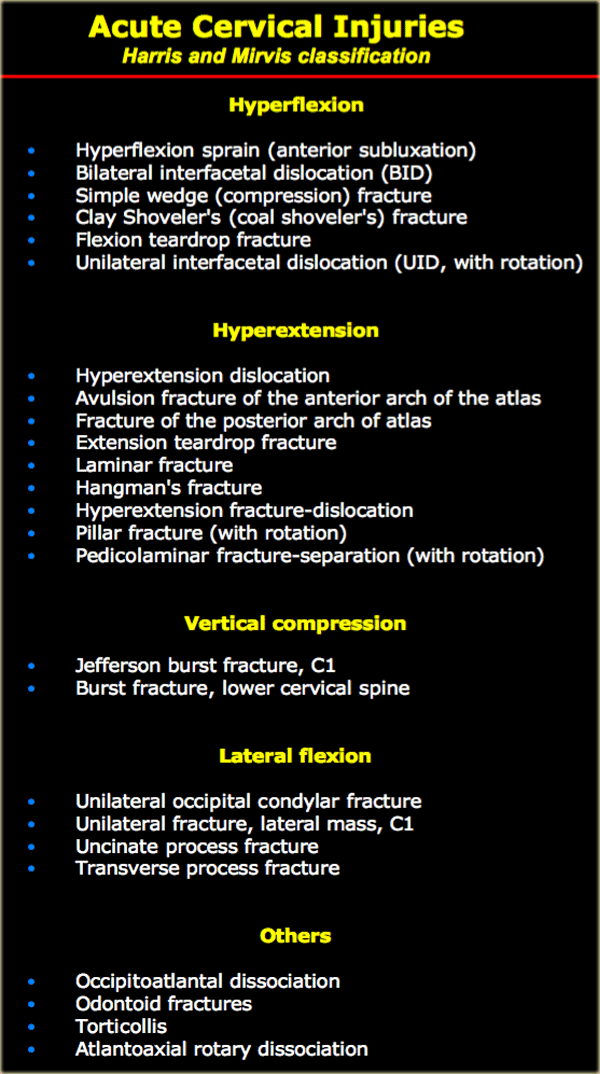
Other injuries
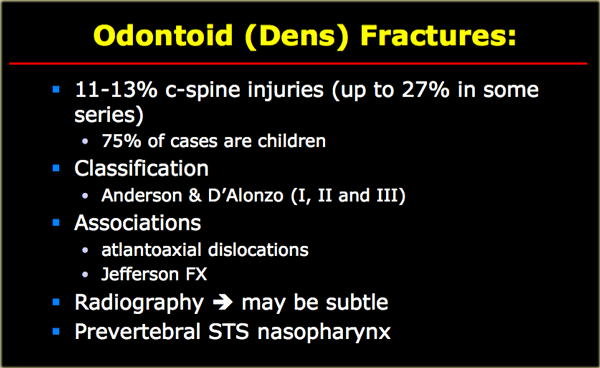
Odontoid fracture
Odontoid or dens-fractures are very common.
They are seen in elderly, but also frequently in children due to the relatively large head-to-spine ratio.
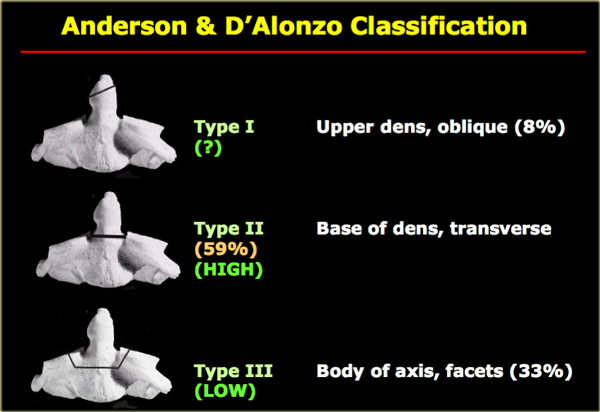
Classification
-
Type I: Avulsion of the tip of the dens where it is attached to C1.
This is a rare fracture.
It is stable, since the fracture line is above the transverse ligament. -
Type II: Through the base of the dens.
Most common fracture.
Always unstable and poor healing. -
Type III: Fracture through the body of the axis and sometimes facets.
Can be unstable, but has a better prognosis than type II due to better healing of the fracture which runs through the metaphyseal bone of the body of C2.
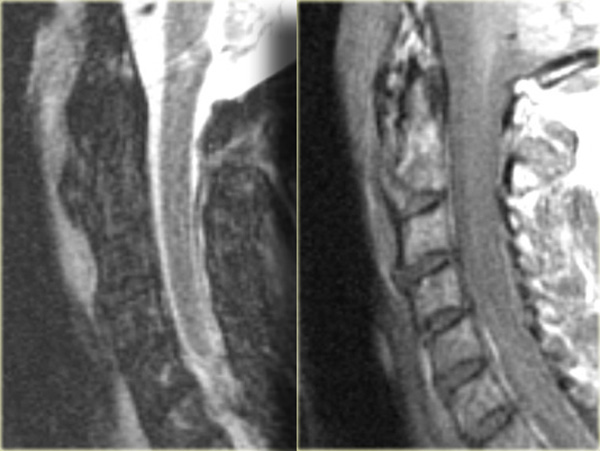
 Odontoid fracture type II
Odontoid fracture type II
On the left the most common type of odontoid fracture, which is type II through the base of the odontoid.
These type II fractures have a tendency to nonunion, which occurs in 64%.
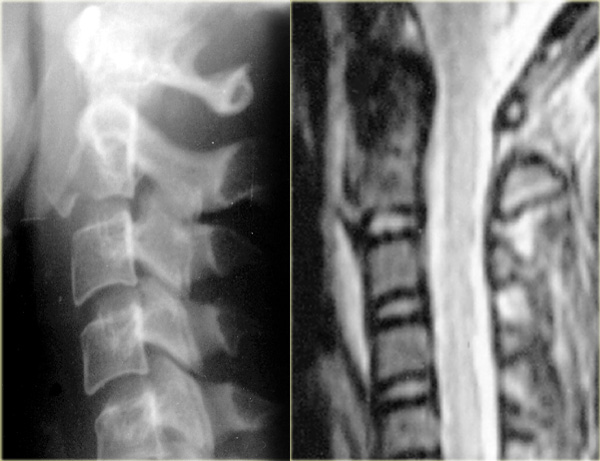
 Odontoid fracture type II
Odontoid fracture type II
On the left another type II odontoid fracture.
Sometimes these fracture-lines can be difficult to see.
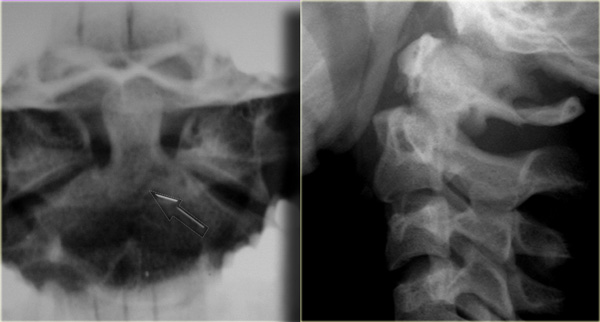
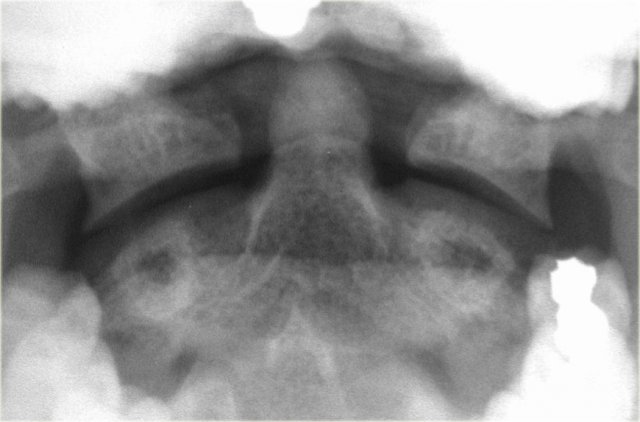 Prominent mach line mimicking an odontoid fracture
Prominent mach line mimicking an odontoid fracture
There are fracture mimics like lucent lines as a result of overprojection or a prominent mach line (figure).
Odontoid fracture (2)
On the left images of a 26-year-old unrestrained passenger in a MVC who was ejected from the automobile.
He had multiple injuries including subdural hematoma, hemothorax, epidural cord bleed, and a T-spine fracture, left L3 transverse process fracture as well as a left clavicle fracture.
There was no neurologic deficit at physiacl examination.
First study the images, then continue reading.
The findings are:
- Fracture through the base of the dens
- Prevertebral soft tissue swelling
- Rupture of C1C2 interspinous ligament
- No visualisation of lower C-spine
Look at the CT-images and then continue reading.
 Odontoid fracture type III
Odontoid fracture type III
The CT confirm the x-ray findings and shows two additional findings:
- The image through the lateral part of C2 nicely shows, that the fracture runs through the body of C2, i.e. a type III odontoid fracture.
-
The posterior dura is in a normal position, but the anterior dura is displaced (arrow).
Continue with the MR-images
The MR demonstrates:
- Fracture through the base of the odontoid
- Prevertebral soft tissue swelling
- Rupture of interspinous ligament
- Displacement of the cord by an epidural fluid collection (could be blood or CSF due to arachnoid rupture)
On the left transverse MR-images at the level of the cervical spine and the thoracic spine.
Notice that at the thoracic level, there is also a epidural fluid collection, but it is located posteriorly.
This resuted from the T-spine fracture.
Continue with the axial images.
 Type III odontoid fracture
Type III odontoid fracture
Odontoid fracture (3)
On the left coronal CT-images of another type III odontoid fracture.
 Unstable type II odontoid fracture
Unstable type II odontoid fracture
Odontoid fracture (4)
On the left images of a type II unstable odontoid fracture.
 Unstable type III odontoid fracture
Unstable type III odontoid fracture
On the left an unstable type III odontoid fracture.
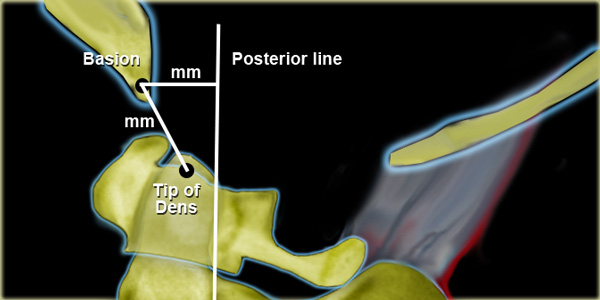 Harris' measurement for AO-DissociationRule of twelves= distance from tip of dens to basion or from basion to posterior line should not exceed 12 mm in an adult.
Harris' measurement for AO-DissociationRule of twelves= distance from tip of dens to basion or from basion to posterior line should not exceed 12 mm in an adult.
Atlanto-occipital dislocation
Atlanto-occipital dislocation is an uncommon injury characterized by complete disruption of all ligaments between occiput and atlas with subluxation or complete dislocation of the occipitoatlantal factes.
Anterior translation of the skull on the vertebral column is the most common presentation.
Death usually occurs immediately from stretching of the brainstem, which causes respiratory arrest.
It is reported to occur in 31% of fatal MVAs.
It is more common in children due to the larger head.
Up to 50% of atlanto-occipital dislocations are overlooked initially, which can have catastrophic results, since cervical traction can be fatal.
Power's ratio is sometimes used as a measurement for the relationship between skull base and spine, but Harris' measurement for AO-dissociation has a greater sensitivity (figure).
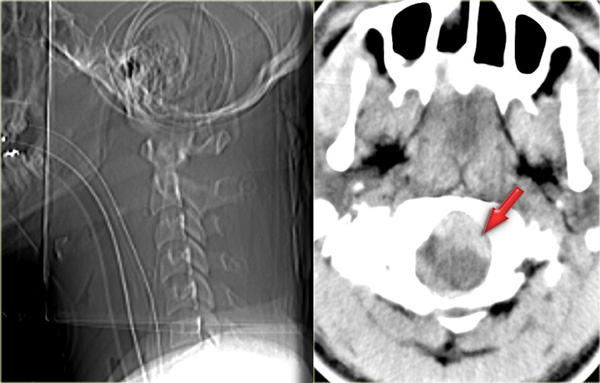
On the left images of an unrestrained passenger, who was ejected from a vehicle and found confused and combative at the scene.
He was intubated and taken to a hospital, where he was found to be quadriplegic.
On the scout view the abnormal relationship between skull and cervical spine is seen.
The axial CT-image demonstrates blood surrounding the brainstem.
On the images on the left notice the abnormal relationships of the basion, opisthion and the tip of the dens and the posterior arch of the atlas.
The subarachnoid space is hyperdense due to the hemorrhage (arrow).
On the left the MR-images.
Notice the prevertebral hemorrhage and the compression on the cord.
Harris classification
NEXUS criteria
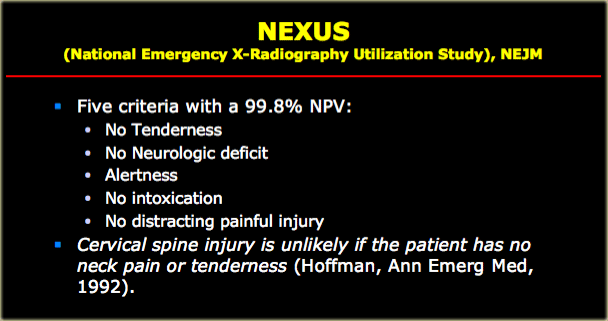
The NEXUS criteria state that a patient with suspected c-spine injury can be cleared providing the following:
- No posterior midline cervical spine tenderness is present.
- No evidence of intoxication is present.
- The patient has a normal level of alertness.
- No focal neurologic deficit is present.
- The patient does not have a painful distracting injury.
Lateral view
The lateral view is the most useful view. Approximately 85-90% of spinal injuries are evident on this view.
Systematic approach:
-
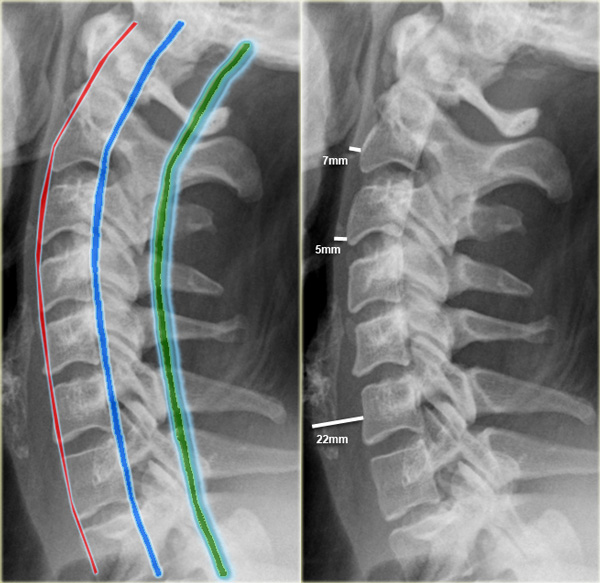
Check alignment by following 3 contour lines:
- Anterior contour line connects the anterior margins of the vertebrae.
- Posterior contour line connects the posterior aspect of the vertebrae.
- Spinolaminar contour line connects the bases of the spinous processes.
- Young children may have pseudosubluxation in upper cervical spine.
-
Prevertebral space:
- at C2 no more than 7 mm.
- at C3 and C4 no more than 5 mm.
- at C6 it is wider due to esophagus and cricopharyngeal muscle, but should not exceed 22 mm in adults or 14 mm in children younger than 15 years.
- In children younger than 24 months there can be physiologic widening of the prevertebral space during forcefull expiration (i.e.crying).
- Widening of the space between spinous processes suggests ligamentous disruption.