Closed Loop in Small bowel obstruction
by Jay P. Heiken and Robin Smithuis
Mallinckrodt Institute of Radiology of the Washington University School of Medicine, St. Louis, Missouri and the Rijnland Hospital, Leiderdorp, the Netherlands
Publicationdate
This article is based on a presentation given by Jay Heiken in 2006 and adapted for the Radiology Assistant by Robin Smithuis.
In 2012 an updated version was presented.
Jay Heiken is professor of radiology at the Mallinckrodt Institute of Radiology of the Washington University School of Medicine in St. Louis.
He has a special interest in abdominal imaging and is co-author of the well known book 'Computed Body Tomography With MRI Correlation'.
Small Bowel Closed Loop Obstruction
Closed Loop Obstruction
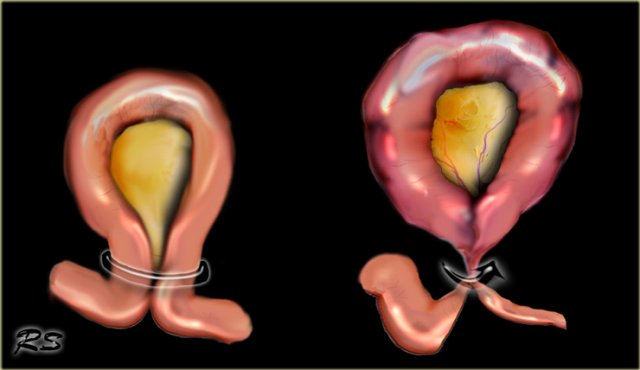
Closed loop obstruction is a specific type of obstruction in which two points along the course of a bowel are obstructed at a single location thus forming a closed loop.
Usually this is due to adhesions, a twist of the mesentery or internal herniation.
In the large bowel it is known as a volvulus.
In the small bowel it is simply known as small bowel closed loop obstruction.
Especially in the small bowel the risk of strangulation and bowel infarction is high with a mortality rate of 10-35%.
Case of small bowel obstruction
Let first start with a rather difficult case and then continue with some basic knowledge about closed loop obstruction.
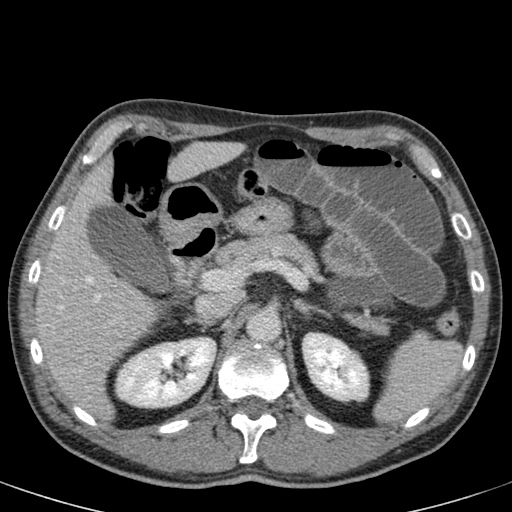
Here we have a patient with a small bowel obstruction.
So the most important question for you to answer is:
Is there a closed loop obstruction?
Because if there is, this patient is at risk for bowel infarction and surgery is the best option.
Scroll through the images.
Can you find the closed loop and what is the cause?
When we have a patient in the ER with what appears to be a small bowel obstruction (SBO), the most important thing we can do, besides making the diagnosis, is to identify the presence or absence of strangulation.
Strangulation is defined as obstruction associated with vascular compromise.
The morbidity and mortality rate in the SBO-group is mainly due to bowel infarction and subsequent necrosis.
This is most commonly caused by a closed loop obstruction.
CT is the imaging procedure of choice in the evaluation of patients suspected of SBO.
 'U' or 'C' shaped loops of bowel. Point of obstruction has a beak-like appearance
'U' or 'C' shaped loops of bowel. Point of obstruction has a beak-like appearance
The CT-presentation of a closed loop obstruction in the small bowel depends on two things:
- length of the bowel segment that forms the closed loop
- orientation of the loop in relation to the imaging plane
If we have a short closed loop oriented within the plane of imaging, we will see a U- or C-shaped loop of bowel.
 Closed loop obstruction with radial array of dilated loops. There is bowel wall thickening and mesenteric edema indicating ischemia
Closed loop obstruction with radial array of dilated loops. There is bowel wall thickening and mesenteric edema indicating ischemia
Another important appearance of a closed loop obstruction is that of a radial array of dilated small bowel loops with the mesenteric vessels converging to a central point.
This is almost always due to a small bowel volvulus.
The findings of ischemia in closed loop obstruction are the same as in patients with other causes of mesenteric ischemia:
- bowel wall thickening
- mesenteric edema
- ascites
- enhancement of the bowel in ischemia can be normal, increased or there can be lack of enhancement.
 Closed loop obstruction with bowel ischemia
Closed loop obstruction with bowel ischemia
The case on the left shows another patient with closed loop obstruction.
Although there is good enhancement of the vessels there seems to be a lack of enhancement of the bowel wall.
Other signs of ischemia in this case are mesenteric edema and bowel wall thickening.
Infarcted bowel was found at operation.
 Closed loop obstruction presenting as a clump of bowel loops
Closed loop obstruction presenting as a clump of bowel loops
If the closed loop is longer and is oriented perpendicular to the plane of section, we will see a clump of bowel loops as shown in the case on the left.
Sometimes this is difficult to appreciate on just the axial images and coronal or sagittal reconstructions can be helpful.
In this case there is also mesenteric edema and localised ascites in combination with dilated loops with wall thickening indicating strangulation and risk of infarction.
Imaging technique in SBO
CT is the imaging procedure of choise in patients who are suspected for bowel obstruction.
When we examine these patients, we should not give oral contrast for following reasons:
- There is already bowel distension and administering oral contrast material will make the patient even more uncomfortable and likely will cause emesis
- The bowel content serves as a neutral contrast agent and i.v. contrast is given to see if there is abnormal enhancement of the bowel wall.
- If positive contrast is given this will hamper our ability to assess the enhancement of the bowel wall.
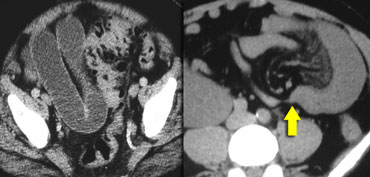
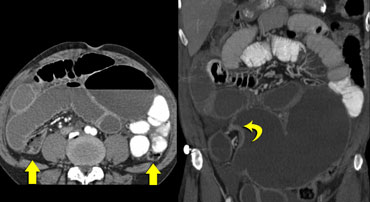
In some of the patients with a closed loop obstruction a bowel obstruction is not suspected.
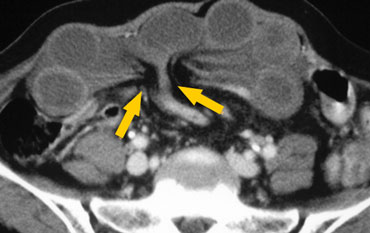
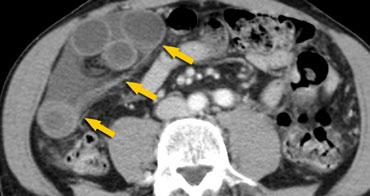
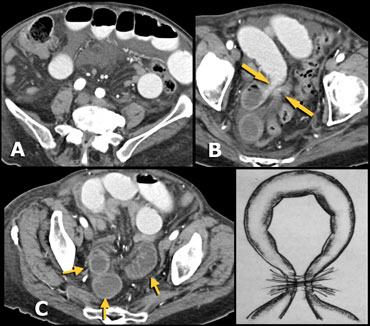
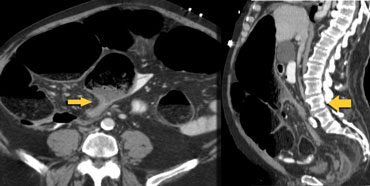
In the case on the left positive oral contrast was given.
Notice the constriction in the small bowel in figure B.
Distal to the constriction in figure C we see a cluster of dilated small bowel loops not filled with oral contrast, indicating the closed loop.
Only rarely contrast will pass the point of obstruction and enter the area of the closed loop.
If we go back to figure B, you may already have noticed that there are two points of narrowing in the small bowel (arrows).
Therefore we have two adjacent collapsed small bowel segments representing the point of the closed loop obstruction.
The bowel wall thickening, ascites and mesenteric edema indicate the presence of bowel ischemia.
Notice that you cannot appreciate the degree of bowel wall enhancement in the loops that are filled with oral contrast.
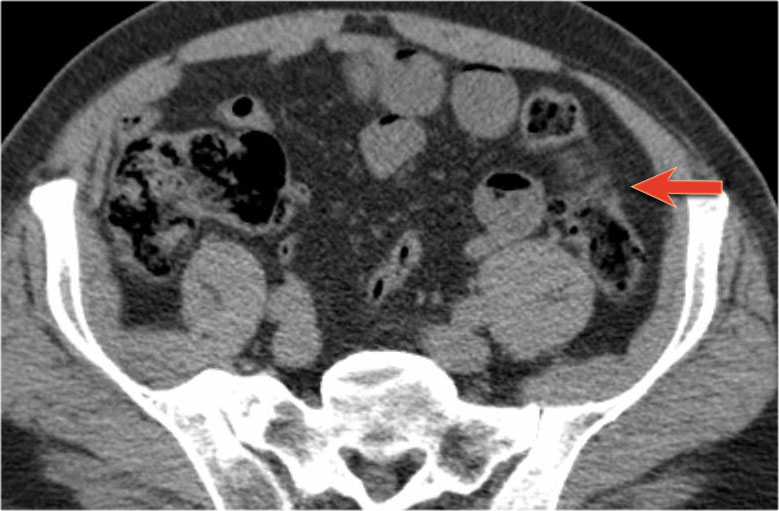
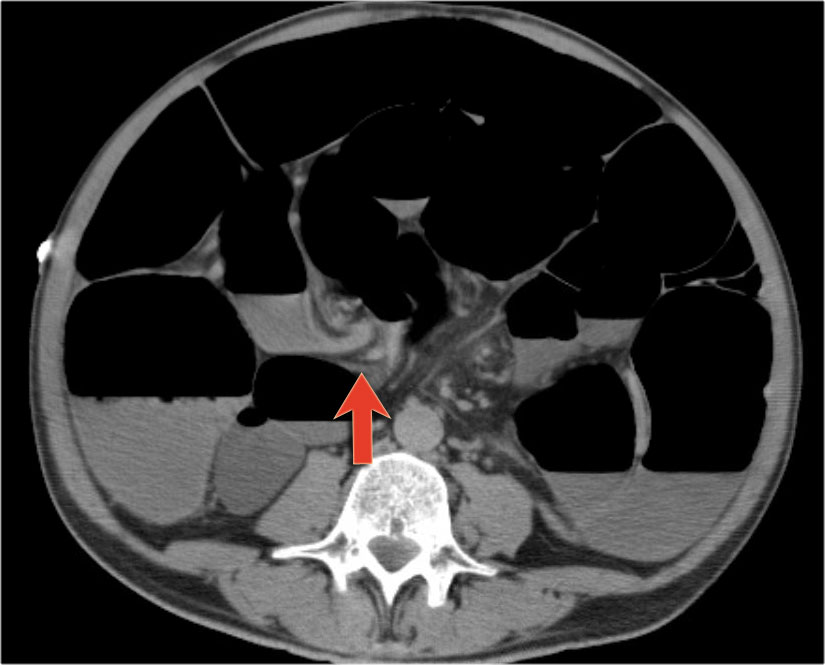
 Closed loop obstruction and small bowel feces sign in a patient with non-dilated proximal bowel
Closed loop obstruction and small bowel feces sign in a patient with non-dilated proximal bowel
Small Bowel Feces Sign
In some of these patients with SBO the proximal small bowel proximal to the point of obstruction may not be dilated.
On the left we see images of a patient in whom obstruction was not suspected.
This patient also received positive oral contrast.
Look for the major findings and then continue.
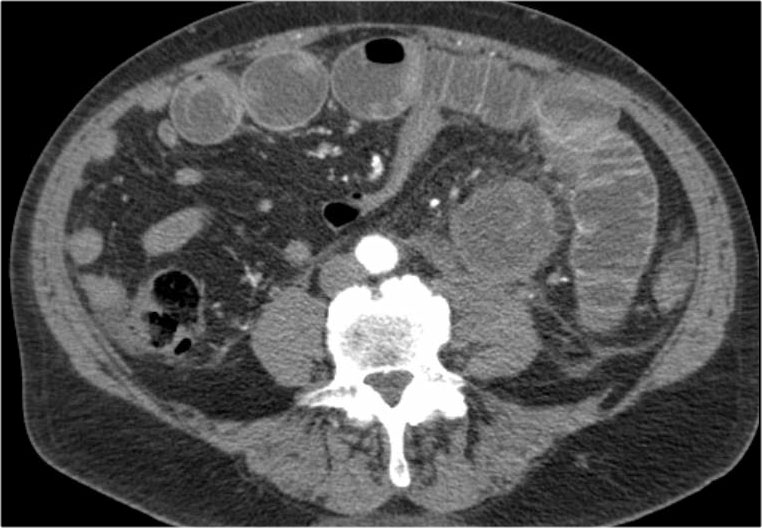
First you will notice that the small bowel is not dilated.
When you go down to the pelvis you see a dilated loop of bowel with inhomogeneous content and finally deep down in the pelvis there is a C-shaped dilated bowel indicating a closed loop obstruction.
The other important finding in this patient is the 'Small Bowel Feces Sign' (SBFS: arrow).
The SBFS is a very useful sign as it is seen at the zone of transition from normal to obstructed bowel and thus facilitating identification of the point and the cause of the bowel obstruction.
The SBFS has been defined as gas and solid material within a dilated small-bowel loop that simulates the appearance of feces.
Case of small bowel strangulation
The CT images are of a patient with mild left flank pain.
At presentation the lab findings were normal.
Based on this CT it was thought that this patient had a diverticulitis (red arrow).
The mild dilatation of the small bowel adjacent to the descending colon was thought to be a reactive sentinel loop.
Scroll through the axial images.
Notice the locally dilated small bowel with the radiating pattern of the mesentery (image 7/11).
Three days later the CT was repeated with i.v. contrast to get a better impression of the small bowel.
There is a progressive dilatation of the small bowel.
First study the images, then continue with the next series.

Notice the radial array of dilated small bowel loops on the left with the mesenteric vessels converging to a central point.
These bowel loops are wider than other loops and show less enhancement.
There are dilated mesenteric veins (yellow arrow).
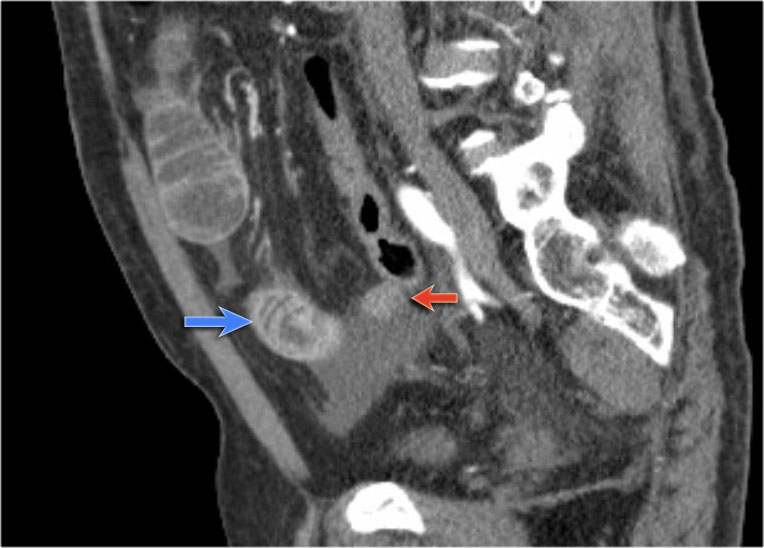
At the point of strangulation the afferent loop is dilated (blue arrow) and efferent loop is collapsed (red arrow).
The distal small bowel is collapsed (red arrows).
The proximal small bowel is dilated (blue arrow).
There is a large amount of ascites in Douglas cave, which also indicates the possibility of ischemia (blue arrow).
Sometimes multiplanar reconstructions can be helpful in making the diagnosis of closed loop obstruction.
Scroll through the sagittal images.
Notice how the afferent loop enters the strangulated bowel and mesentery (image 8-10/13).
Notice reactive changes in the mesocolon simulating diverticulitis.
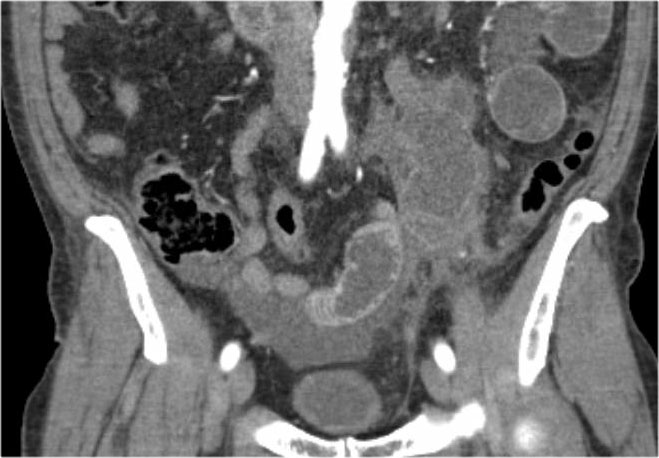
The coronal reconstruction demonstrates the point of strangulation with the dilated afferent loop, the strangulated loop and the collapsed efferent loop.
The yellow arrow marks the dilated veins.

At operation an ischemic strangulated small bowel was found, which was herniated through a hole in the mesocolon.
Here we see the resected part of the small bowel.
Notice the areas of necrosis and the dilated veins, which were also seen on the CT-images.
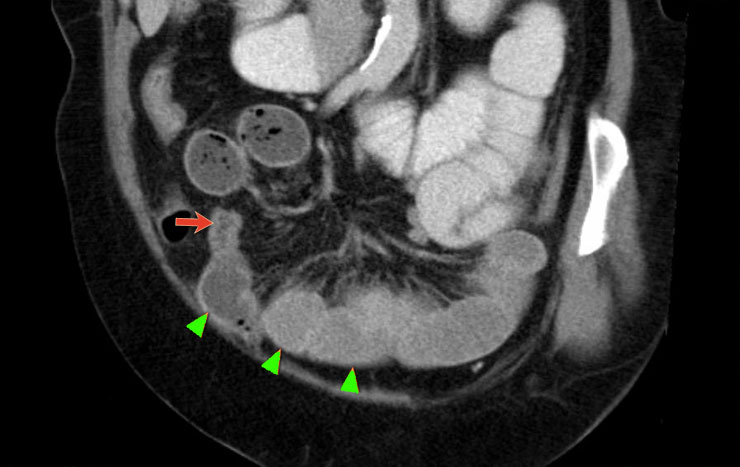
Coronal reconstructions of another patient with a closed loop obstruction.
The obstructed afferent loops are indicated in red arrowheads.
The collapsed efferent loop is indicated by a red arrow.
Notice the closed loop cranially to the area of obstruction.
At surgery the bowell was not ischemic.
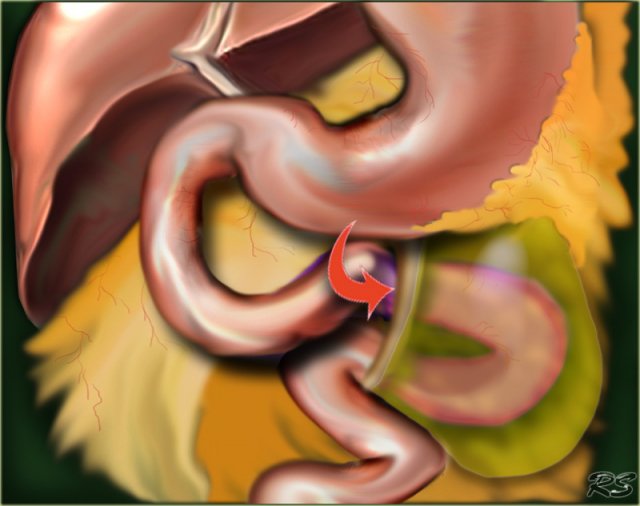
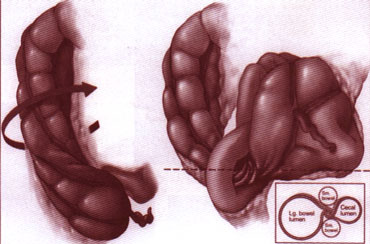
Paraduodenal herniation
There are various types of internal herniation.
The illustrations shows a left paraduodenal hernia.
This is an uncommon form of internal herniation.
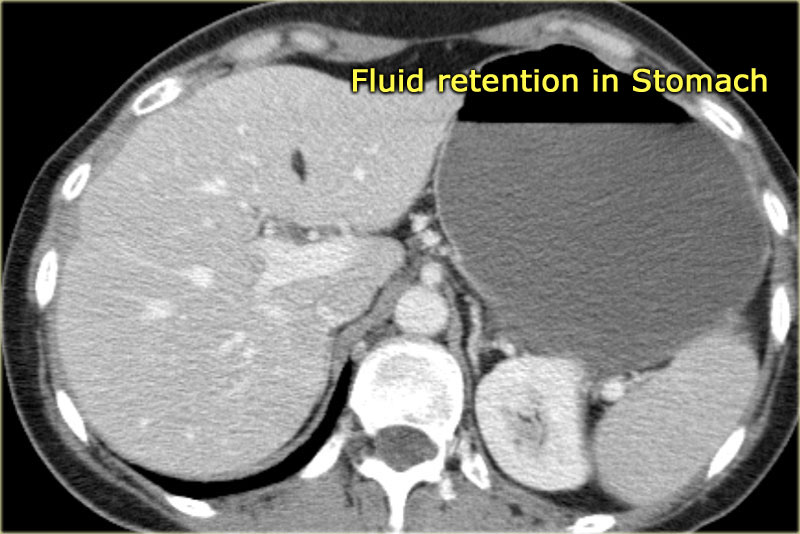
The CT-images show a left paraduodenal hernia.
Notice the engorged veins (blue arrow).
The duodenum is dilated (red arrow) and there is retention of fluid in the stomach.
At operation the herniated small bowel was not ischemic.
Volvulus of Large Bowel.

On the left a plain abdominal film is shown of a 57 year old man with a two day history of increasing abdominal pain and distension.
First look at the image and then continue.
Besides diffuse dilatation of the bowel, the major finding on this film is a large air containing structure in the pelvis.
An important diagnosis to consider would be a volvulus of the colon and many would diagnose this as a sigmoid volvulus because it is located in the pelvis.
However this actually is a cecal volvulus as will be explained below.
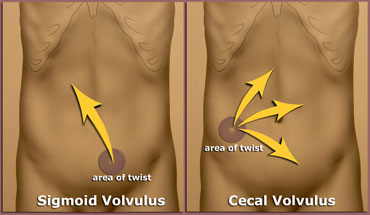 Cecal volvulus can go almost anywhere
Cecal volvulus can go almost anywhere
Cecal Volvulus
A volvulus always extends away from the area of bowel twist.
So a sigmoid volvulus can only move upwards and usually goes to the right upper quadrant.
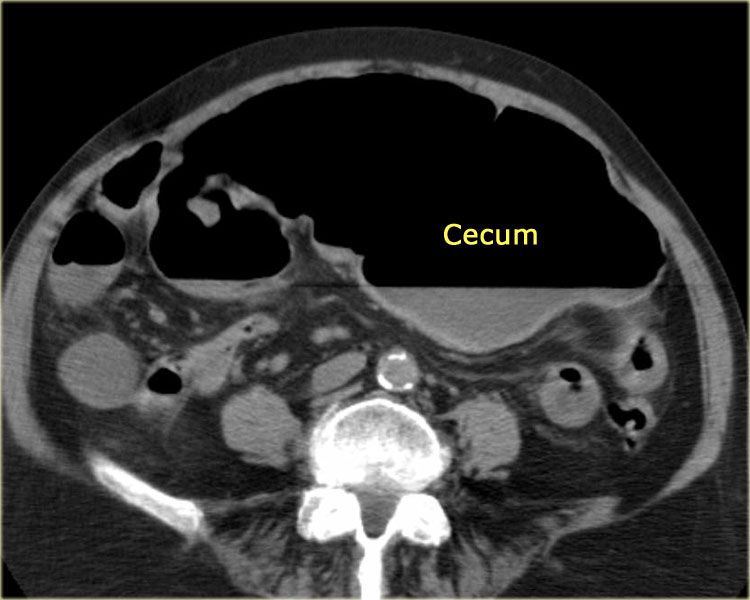
Cecal volvulus however can go almost anywhere and can even be located in the pelvis (figure).
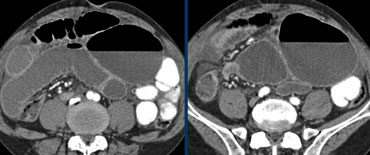
On the left there are additional CT-images of the same patient as above.
First look at these images and look for the major findings and then continue.
First we see a collapsed descending colon and a non-dilated ascending colon, so this cannot be a sigmoid volvulus.
Secondly, we see a beak-like structure in the right lower quadrant which is where the bowel is twisted.
In the left lower quadrant we see the dilated cecum.
Coronal recontructions can be very helpfull in demonstrating what is going on.
On the left we see the non-dilated ascending and descending colon (straight arrows) and the transition point of the volvulus (curved arrow).
Cecal volvulus is due to the cecum twisting around the ascending colon thus leading to small bowel obstruction.
A long narrow based mesentery predisposes to volvulus.
An incomplete midgut rotation is a predisposing factor.
Infarction is usually the result of venous congestion, while the arterial supply is rarely compromised.
Cecal volvulus accounts for about 25% of cases of colonic volvulus.
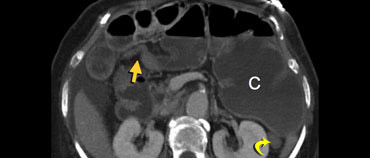 Dilated cecal volvulus (C) shifting away from the area of bowel twist (arrow)
Dilated cecal volvulus (C) shifting away from the area of bowel twist (arrow)
On the left a typical cecal volvulus is seen.
We can see the beak-like transition zone located in the right lower quadrant indicating that this is a cecal volvulus.
The dilated cecum is located in the left upper quadrant.
Also notice the collapsed descending colon posterior to the dilated cecum (curved arrow).
The x-rays show a typical cecal volvulus.
Notice that the dilated bowel points toward the area of twist, which is the area where you expect the cecum to be located.
Continue with the CT-images.
Scroll through the images.
The areas of twist and obstruction are marked.

Sigmoid Volvulus
On the left a patient with a sigmoid volvulus.
We can see the distended sigmoid extending from the pelvis way up into the right upper quadrant.
Look at the image and decide for yourself why this cannot be a cecal volvulus.
Then continue.
The key finding is the dilatation of the proximal colon.
The dilated loop seen on the left side is the dilated transverse colon.
At CT we can nicely appreciate the area of the twist with the sigmoid extending up to the diafragm.
The sigmoid is the commonest site of colonic volvulus.
It accounts for 75% of large bowel obstruction.
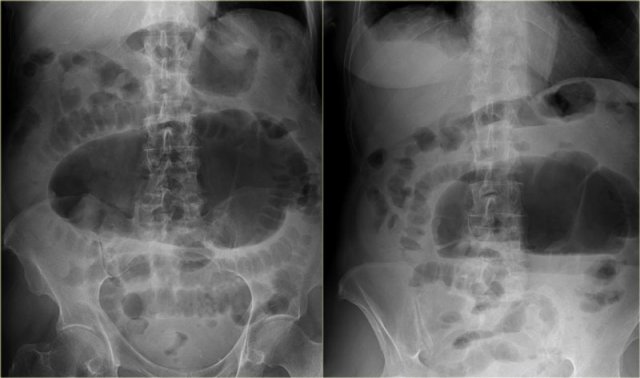
 Sigmoid volvulus
Sigmoid volvulus
AP supine and erect radiograph of the abdomen demonstrates the characteristic coffee bean sign in sigmoid volvulus.
Notice that the dilated loops point towards the sigmoid area.
Continue with the CT-images.

Scroll through the images.
Notice the transition point (red arrows).
 Sigmoid volvulus
Sigmoid volvulus
Here another sigmoid volvulus.
On the abdominal x-rays it is difficult to recognize what is going on, since so many bowel loops are dilated.
Continue with the CT-images.
CT is very helpful in this case and demonstrates the twist at the transition point (arrow).
The last image shows the collapsed rectum posterior to the dilated small bowel loops.

In the pelvis dilated small bowel loops were seen and a collapsed distal sigmoid (arrow).