Carpal instability
Louis A. Gilula and Ileana Chesaru
Mallinckrodt Institute of Radiology Washington University St. Louis, Missouri, USA and the Westeinde hospital the Hague the Netherlands.
Publicationdate
This article is based on a presentation given by Louis Gilula and adapted for the Radiology Assistant by Ileana Chesaru.
First a systematic analysis of the wrist is presented to look for carpal instability and fracture dislocation.
Secondly cases are presented as examples in the chapter systematic review and diagnosis.
Wrist analysis
When you analyse the wrist to look for possible carpal instability and fracture dislocation, you should ask yourself the following questions:
- Is there good positioning of the patient. This is essential to be able to make statements about improper alignment or abnormal axes of carpal bones.
- Is there normal alignment between the carpal bones. The carpals should be parallel when profiled. Any overlap indicates abnormal tilting, dislocation or fracture.
- Is there any disruption of the three carpal archs. Disruption indicates ligament tear or a fracture.
- What is the shape and axis of the carpal bones. Give special attention to lunate, scaphoid and capitate. An abnormal shape indicates abnormal tilt with or without dislocation.
Answering these questions will help you find clues to carpal instability, dislocation and fractures.
Radiography

Positioning
PA view should be taken with the wrist and elbow at shoulder height. Only in this position, the radius and the ulna are parallel. Moving the arm down makes the radius cross the ulna and become relatively shorter. So it will be impossible to make any statements on the length of the ulna (plus or minus variant)
Lateral view is taken with the elbow adducted to the side. Shoulder, elbow and wrist are again in one plane. This positioning will make the lateral view exactly perpendicular to the PA view.
 Extensor carpi ulnaris groove (yellow arrow) seen radial to the midportion of the ulnar styloid.
Extensor carpi ulnaris groove (yellow arrow) seen radial to the midportion of the ulnar styloid.
PA view
A correctly positioned PA view will show the extensor carpi ulnaris groove radial to the midportion of the ulnar styloid.
The PA and lateral view are equally important and thus should both be studied carefully.
The PA view usually shows what is wrong and the lateral view shows in what direction the bones move.
Sometimes an oblique view will also be obtained, especially if you want to look at the trapezium-trapezoid joint in profile.

Lateral view
Only on a good positioned lateral view one can see the volar edges of respectively scaphoid, pisiform and capitate separately and lined up as shown on the left.
Lunate is the semilunar bone that fits in the distal radius. Looking through that, one can see the convexity of the scaphoid.
Distally from the scaphoid is the trapezium. The angular shaped bone visible dorsally is the triquetrum.
The square bone that bridges the proximal and distal half of the wrist is the pisiform.
Capitate is the rounded bone fitting inside the distal lunate.
Distally between the metacarpals, one can make out the hook of the hamate.
 Same projection of ulna and ulnar styloid on PA and lateral view due to malpositioning in a patient with a perilunate fracture dislocation.
Same projection of ulna and ulnar styloid on PA and lateral view due to malpositioning in a patient with a perilunate fracture dislocation.
Improper positioning may result in the same view of the ulna on both the PA and lateral view as shown in the case on the left. Nowhere in the body you would accept two views giving you the same image of a bone.
 Normal oblique radiograph of the wrist and schematic representation
Normal oblique radiograph of the wrist and schematic representation
Oblique view
An oblique view is not routinely performed. It is however the only view showing the trapezio-trapezoidal joint.
Joint spaces: parallelism and symmetry
The joint spaces of the wrist have a width of 2 mm or less. Only the radiocarpal joint is slightly wider. The carpometacarpal joints are slightly narrower than the midcarpal joints.
The capitolunate joint is considered the baseline joint width to which other joint spaces can be compared. One should make sure to look at all of them: the radiocarpal, the proximal intercarpal, the midcarpal, the distal intercarpal and the carpometacarpal joint spaces.
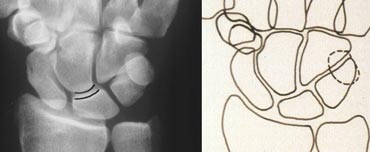
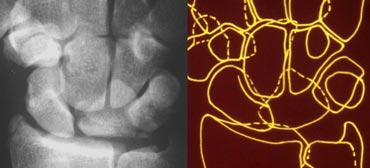
 Study the carpal bones as pieces of a jigsaw puzzleLEFT: Schematic representation of the wrist with the outlines tracing the outer margins of the bonesRIGHT: Schematic representation of the wrist with the lines tracing the carpal bones as pieces of a jigsaw puzzle
Study the carpal bones as pieces of a jigsaw puzzleLEFT: Schematic representation of the wrist with the outlines tracing the outer margins of the bonesRIGHT: Schematic representation of the wrist with the lines tracing the carpal bones as pieces of a jigsaw puzzle
Carpal joints should be symmetrical. Furthermore, when viewed in profile (tangentially), the cortical margins of the bones constituting that joint should be parallel. Bone edges that are not viewed in profile do not display this parallelism, e.g. the distal portion of the scaphoid that articulates with the capitate.
Studying this parallelism is easier when regarding the carpal bones as pieces of a jigsaw puzzle that all fit together, as opposed to tracing carpal bones by their outer cortical margins producing the outlines (figure).
When one bone is not paralleling the others, that is out of place. If the rest of the bones still parallel each other, they have stayed together.
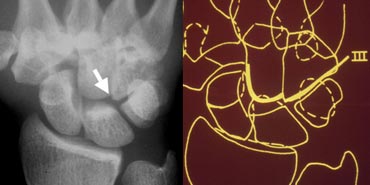
 PA radiograph and schematic representation of the wrist, with dislocation of the lunate
PA radiograph and schematic representation of the wrist, with dislocation of the lunate
The picture on the left shows abnormal overlapping of the lunate with the capitate, hamate and triquetrum. We also see the medial profile surface of the scaphoid, but nothing paralleling it. There is also abnormal widening of the radiolunate space. The other joints are nicely parallel and symmetric. This leads to the conclusion that the lunate is displaced while the other bones have stayed together.
Carpal arcs
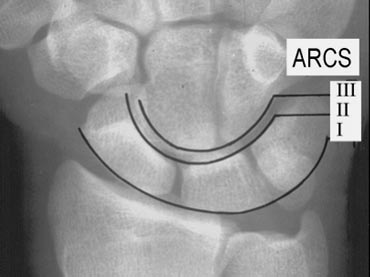 PA radiograph of the wrist. The three normal carpal arcs
PA radiograph of the wrist. The three normal carpal arcs
The next step is looking at the three carpal arcs: smooth curves joining the surfaces of the carpal bones as shown on the left.
The first arc is a smooth curve outlining the proximal convexities of the scaphoid, lunate and triquetrum.
The second arc traces the distal concave surfaces of the same bones, and the third arc follows the main proximal curvatures of the capitate and hamate.
 PA radiograph of the wrist and schematic representation showing disruption of the first carpal arc
PA radiograph of the wrist and schematic representation showing disruption of the first carpal arc
Distruption of carpal arcs
An arc is disrupted if it cannot be traced smoothly. A break in one of the arcs indicates a fracture or the disruption of a ligament leading to a subluxation or dislocation.
On the left one can note the disruption of arc I at the lunotriquetral joint.
 Disruption of the second carpal arc
Disruption of the second carpal arc
A disruption of the second carpal arc at the scapholunate joint and the lunotriquetral joint is seen on the left. Although there is a gap in the first arc, it can still be traced by a smooth curve so arc I is considered intact.
 Disruption of the third carpal arc at the capitohamate joint
Disruption of the third carpal arc at the capitohamate joint
Disruption of the third carpal arc is shown in the next case on the left. There is an abnormal step off at the capitohamate joint.
Shape of carpal bones
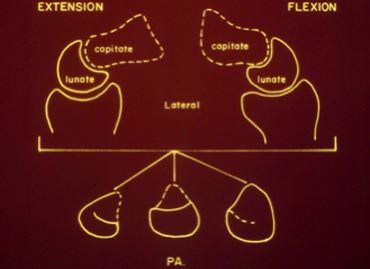 Schematic representation of the lunate shape in different positions
Schematic representation of the lunate shape in different positions
Lunate shape
The lunate has a trapezoidal shape, as the sides converge from the proximal surface to the distal surface, which are grossly parallel. If the lunate is tilted, it becomes triangular in shape. Awareness of this fact prevents thinking the lunate might be dislocated based only on its appearance, that in fact changes with its position.
So it may be dislocated with tilting or just be tilted.
 LEFT: Lunate dislocation: capitate is centered over the radius and lunate is tilted out.RIGHT: Perilunate dislocation: lunate is centered over the radius and capitate is tilted out dorsally.
LEFT: Lunate dislocation: capitate is centered over the radius and lunate is tilted out.RIGHT: Perilunate dislocation: lunate is centered over the radius and capitate is tilted out dorsally.
Lunate vs. perilunate dislocation
Common dislocations of the wrist are the lunate and perilunate dislocations. The key to differentiation between both is what is centered over the radius. If the capitate is centered over the radius and the lunate is tilted out, it is a lunate dislocation. If however the lunate centers over the distal radius and the capitate is dorsal, we are dealing with a perilunate dislocation (figure).
 LEFT: Lateral radiograph of the wrist in extention showing scaphoid elongationRIGHT: PA radiograph of the wrist in ulnar deviation showing elongation of the scaphoid
LEFT: Lateral radiograph of the wrist in extention showing scaphoid elongationRIGHT: PA radiograph of the wrist in ulnar deviation showing elongation of the scaphoid
Scaphoid shape
The scaphoid shape changes with movement of the wrist. In ulnar deviation or extension the scaphoid elongates to fill the space between the radial styloid and the base of the thumb (the trapezium).
 LEFT: PA radiograph of the wrist in radial deviation showing foreshortening of the scaphoid: signet ring signRIGHT: Schematic representation of the wrist in flexion showing tilting of the scaphoid towards the palm
LEFT: PA radiograph of the wrist in radial deviation showing foreshortening of the scaphoid: signet ring signRIGHT: Schematic representation of the wrist in flexion showing tilting of the scaphoid towards the palm
Both with radial deviation aswell as flexion of the wrist the space between the radial styloid and trapezium is reduced. As scaphoid fills this space it will foreshorten and tilt towards the palm. This will give scaphoid a signet ring appearance (figure).
Axis of the carpal bones
Drawing the longitudinal axes of some of the carpal bones on a lateral radiograph and measuring the angles between them is a good method of determining the wrist bones? spatial relationship. The three most important axes are those through the scaphoid, the lunate and the capitate, drawn on the lateral radiograph.
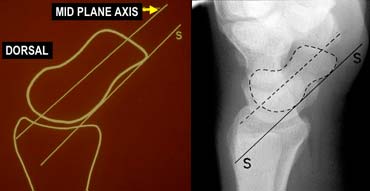
Scaphoid axis
The true axis of the scaphoid is the line through the midpoints of its proximal and distal poles. Since the midpoint of the proximal pole is often difficult to appreciate, an almost parallel line can be used that is traced along the most ventral points of the proximal and distal poles of the bone (figure).
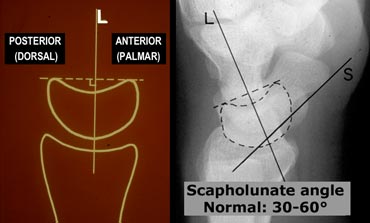 LEFT: Lunate axis drawn perpendicular to a line joining the distal palmar and dorsal bordersRIGHT: Radiograph with lunate and scaphoid axis drawn.
LEFT: Lunate axis drawn perpendicular to a line joining the distal palmar and dorsal bordersRIGHT: Radiograph with lunate and scaphoid axis drawn.
Lunate axis
The axis of the lunate runs through the midpoints of the convex proximal and concave distal joint surfaces and can best be drawn by finding the perpendicular to a line joining the distal palmar and dorsal borders of the bone as demonstrated on the left.
Scapholunate angle
Normal: 30 - 60?
Questionably abnormal: 60 - 80?
Abnormal: > 80? This indicates instability of the wrist.
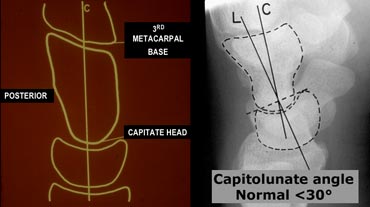 LEFT: Capitate axisRIGHT: Radiograph with lunate and capitate axis drawn.
LEFT: Capitate axisRIGHT: Radiograph with lunate and capitate axis drawn.
Capitate axis
The capitate axis joins the midportion of the proximal convexity of the third metacarpal and that of the proximal surface of the capitate.
Capitolunate angle
Normal:
Abnormal: > 30?.This indicates instability of the wrist.
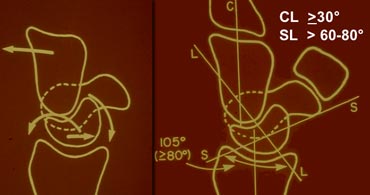 LEFT: Dorsal tilting of the lunate in DISIRIGHT: Scapholunate angle is > 80?
LEFT: Dorsal tilting of the lunate in DISIRIGHT: Scapholunate angle is > 80?
DISI or dorsiflexion instability
DISI is short for dorsal intercalated segmental instability.
The intercalated segment is the proximal carpal row identified by the lunate. The term 'intercalated segment' refers to it being the part in between the proximal segment of the wrist consisting of the radius and the ulna and the distal segment, represented by the distal carpal row and the metacarpals.
So all this means is that in DISI or dorsiflexion instability the lunate is angulated dorsally.
If you think lunate is tilted, measure the scapholunate angle ( 30-60?is normal, 60-80?is questionably abnormal, >80? is abnormal) and the capitolunate angle (
In the figure on the left the scapholunate angle is measured: it is 105 degrees. As mentioned before this angle is considered abnormal if greater then 80 degrees.
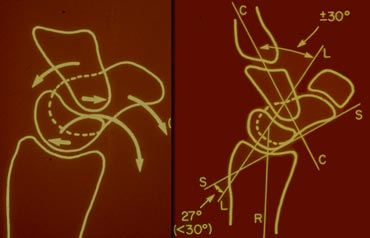 LEFT: Volar tilting of the lunate in VISIRIGHT: Scapholunate angle is
LEFT: Volar tilting of the lunate in VISIRIGHT: Scapholunate angle is
VISI or volarflexion instability
Volar intercalated segmental instability or palmar flexion instability is when the lunate is tilted palmarly too much.
While most DISI is abnormal, in many cases VISI is a normal variant, especially if the wrist is very lax.
Systematic review and diagnosis
In the next cases we advise you to first look at the images on the left and give a full description of the radiographs.
Look for symmetry, parallelism, and the shape and axis of the carpal bones. Find out if there are any fractures and then try to make the diagnosis
Then read the text on the right to see if you're right.
 PA and lateral view of the wrist
PA and lateral view of the wrist
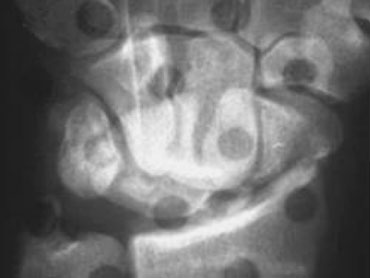
Case 1
Systematic interpretation of the case on the left shows us the following:
1. On the PA-view all the carpal bones parallel each other except for the lunate.
2. The carpal arcs I and II are disrupted at the LT and SL joints.
3. Triangular shaped lunate
So by just looking at the PA view we can make the diagnosis of lunate dislocation.

Case 2
Analysis:
1. No parallelism at the TL joint since there is overlapping of the triquetrum and the lunate.
2. Also overlapping of the hamate and the lunate.
3. There is parallelism between radius, lunate, proximal pole of scaphoid and proximal pole of capitate. So these bones form a unit.
4. Also parallelism between triquetrum, hamate, distal pole of capitate, trapezium and distal pole of scaphoid.
5. Fracture of capitate and scaphoid
So these findings indicate that this is a transscaphoid, transcapitate perilunate fracture-dislocation.
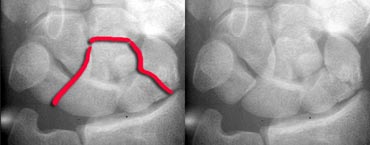
On the left you see the same case with a line indicating the fracture-dislocation line.

Same case with additional oblique and lateral view showing the dorsal dislocation.
Case 3
Analysis:
1. Fracture of scaphoid and ulnar styloid process.
2. Broken arcs I and II at LT joint.
3. Some parallelism between lunate and proximal pole of scaphoid with the radius.
4. Scaphoid is foreshortened so it is tilted and has moved towards the palm.
5. All the other carpals show parallelism exept for lunate, the proximal pole of scaphoid and the radius.
Although this probably is a perilunate dislocation, based on the PA-view alone it is very difficult to say if this is a lunate or perilunate dislocation. The triangular shape of the lunate could be the result of just tilting or dislocation with tilting.
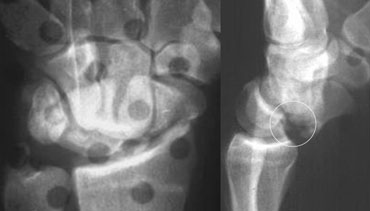 Perilunate dislocation with fracture of scaphoid and ulnar styloid processThe volar tip of lunate is also broken (see circle).
Perilunate dislocation with fracture of scaphoid and ulnar styloid processThe volar tip of lunate is also broken (see circle).
Same case with the lateral view also shown.
Now we see that there definitely is a perilunate dislocation.
So the triangular shape of the lunate is the result of just tilting.
On the lateral view a fracture of the volar tip of lunate is seen. So this patient is at risk for recurrent dislocation.

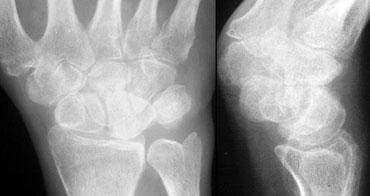
Case 4
Analysis:
The case on the left shows severe arthrosis at the STT joint and CMC1 joint with subluxation. Carpal arcs are normal and there is normal paralelism.The scaphoid is elongated which means it is dorsally tilted.
On the lateral view we can see that the lunate is also tilted dorsally. The proximal carpal row has moved as a unit, so there is no dissociation.
Final diagnosis: non-dissociated DISI with arthrosis and subluxation of STT joints.

Case 5
Analysis:
1. Loss of parallelism at LT joint resulting in broken arc I and II.
2. Lunate and scaphoid are parallel to each other but not to the other carpals.
3. Scaphoid is foreshortened due to palmar tilting.
4. Lunate is parallel to scaphoid. So the triangular shape must be the result of palmar tilting.
5. The proximal carpal row is not a unit since arc I is broken.
 Lateral view demonstrates the volar tilting of lunate which was already suspected on the PA view.
Lateral view demonstrates the volar tilting of lunate which was already suspected on the PA view.
Final diagnosis:
VISI with dissociation at the LT joint.

Case 6
Analysis:
1. Widened and narrowed joints, but there is normal parallelism , so there is no dislocation.
2. Scapholunate dissociation with widening of the SL joint and foreshortening of the scaphoid due to palmar tilt.
3. Arthrosis of the Radioscaphoid and Capitolunate joint due to the abnormal movements of scaphoid and lunate.
4. Dorsal tilt of lunate indicating DISI.
This condition is known as SLAC. In this case it is post-traumatic due to the SL-ligament tear.
SLAC (scapholunate advanced collapse) refers to a specific pattern of osteoarthritis and subluxation which results from untreated chronic scapholunate dissociation or from chronic scaphoid non-union
The degenerative changes occur in areas of abnormal loading, which is the radial-scaphoid joint, followed by degeneration in the unstable lunatocapitate joint, as capitate subluxates dorsally on lunate.
 SLAC of CPPD TYPE
SLAC of CPPD TYPE
On the left another case of SLAC. This case is due to CPPD.
Characteristics of CPPD with SLAC are:
- Decreased size of proximal scaphoid due to erosion and resorption.
- Scaphoid fossa erosion